
Abstract
Objectives
Eustachian tube dysfunction (ETD) is a common disease associated with chronic otitis media. A standard diagnostic tool for ETD in patients with tympanic membrane perforation is still lacking. We developed and validated a new diagnostic model for ETD in patients with tympanic membrane perforation.
Methods
A prospective study was conducted in patients who had tympanic membrane perforation from February to August 2023. We collected clinical characteristics and examination results including otoscopy, nasal endoscopy, tubomanometry, and 5-item Eustachian Tube Score (ETS-5). Univariate and multivariate logistic regression analysis was performed to determine the independent diagnostic factors. Based on this, the nomogram model was constructed. The discrimination and calibration of the nomogram were evaluated using the area under the curve (AUC), the C-index, the calibration curve, and the decision curve analysis (DCA).
Results
A total of 40 participants were enrolled in the study. ETS-5 score and Eustachian tube opening mucosa inflammation in the nasopharynx were significant predictors in identifying ETD. Based on the above independent predictors, a diagnostic nomogram was successfully established. The sensitivity and specificity of the diagnostic model were 80.0% and 90.0%, respectively. The AUC and the C-index of the diagnostic model were both 0.901, which suggested that the model had a good discrimination power. The calibration curve indicated a good calibration degree of the model. DCA showed that the proposed model was useful for clinical practice.
Conclusion
The nomogram model is effective and reliable in identifying ETD in patients with tympanic membrane perforation.

Keywords
Introduction
Eustachian tube dysfunction (ETD) describes a series of signs and symptoms including ear fullness, otalgia, muffle hearing, tinnitus, and hearing loss, that are due to abnormally delayed or decreased opening of the Eustachian tube (ET). 1 ETD is a common condition with a worldwide prevalence of 1% to 5% 2 and is reported to be responsible for more than 2 million physician visits and associated costs of $4 billion annually in the United States. 3 In an international cross-sectional study, 142,889 patients per year were diagnosed with chronic ETD. 4 However, ETD is often considered a “black box” due to its complex anatomy, multiple functions, and the impact of intrinsic and external factors. 5 Previous studies have shown that Eustachian tube plays an important role in various middle ear pathologies.6,7 ETD is commonly considered to be the cause of otitis media with effusion, tympanic membrane retraction, chronic suppurative otitis media (CSOM), and cholesteatoma.8,9 However, it is controversial whether ETD is related to the outcome of middle ear surgery or not. The important issue might be how to recognize ETD in patients with tympanic membrane perforation. For example, Takahashi et al. reported that mechanical ET obstruction and impaired middle ear pressure-regulation functions might cause the poor outcome of tympanoplasty. In the study, they found that none of poor positive and negative middle ear pressure-equalizing functions and mastoid aeration were individually linked to the poor outcome of tympanoplasty unless all the 3 parameters were poor. 10 Moneir et al. reported saccharine and pressure swallow equalization tests had a good positive correlation with graft success in tympanoplasty, while the methylene blue test had no impact on the graft success rate. 11 Furthermore, Li et al. showed the graft healing rate of ETD group (diagnosed by Eustachian Tube Score) was not significantly different from the normal group, indicating ETD may not affect the outcomes of type I tympanoplasty for CSOM. 12 From the above studies, we can see that the correlation between ETD and the outcome of tympanoplasty varied from different diagnostic methods of ETD. Therefore, it’s important to validate a valid and general measurement for ETD in patients with tympanic membrane perforation.
Although a variety of tests have been used to assess the function of ET, none of them can provide reliable and high-level evidence for the diagnostic criteria of ETD. 5 There is no gold standard method for diagnosing ETD. Therefore, most clinicians must rely on clinical symptoms in conjunction with objective tests such as tympanogram, otoscopy, endoscopy, and Valsalva maneuvers as potential diagnostic markers for ETD. 13 To increase the accuracy of the tests, efforts have been made to develop patient-reported outcome measures, such as the 7-item Eustachian Tube Dysfunction Questionnaire (ETDQ-7) 14 and the Cambridge ETD Assessment 15 and the Eustachian Tube Score (ETS). 16 After evaluating the diagnostic pathway of ETD, it became apparent that ETD should be diagnosed based on clinical assessments and ET opening tests. 17 Therefore, Lu et al combined objective tubomanometry and subjective ETDQ-7 to create a new evaluation standard for ET function, the T-ETDQ, which has good discriminant for ETD in patients with the intact tympanic membrane. 18 Similarly, in our previous study, we used the ETDQ-7 and the ETS-5 together to successfully diagnose ETD in patients with chronic rhinosinusitis. 19
However, based on previous studies,20,21 the ETDQ-7 is designed for patients with intact tympanic membranes. Because of the more severe symptoms caused by CSOM or cholesteatoma, the ETDQ-7 and other ear symptomatic assessments are not appropriate for patients with tympanic membrane perforation. T-ETDQ is not recommended for individuals with tympanic membrane perforation in this situation. Fortunately, Schroder et al have indicated that ETS can be a useful diagnostic approach in individuals with perforated tympanic membranes. 16 Therefore, ETS-5 and other endoscopic results were emphasized in this study.
The aim of this prospective study is to develop and validate a new diagnostic nomogram model in patients with tympanic membrane perforation. We hope to develop appropriate diagnostic techniques for ETD in different types of patients that will guide the selection of medical or surgical interventions.
Materials and Methods
Patient Selection
We prospectively enrolled patients from February to August 2023 in the Department of Otorhinolaryngology, Head and Neck Surgery in the New Territories East Cluster of the Hong Kong Hospital Authority. The study was approved for human studies by the Institutional Review Board of the Joint Chinese University of Hong Kong-New Territories East Cluster Clinical Research Ethics Committee (2022.483).
Inclusion and Exclusion Criteria
Inclusion criteria were as follows
(1) Age 18 to 70 years old.
(2) Suffering from unilateral chronic otitis media (COM) with tympanic membrane perforation (patients diagnosed with CSOM or cholesteatoma).
(3) Assessments including ETS-5 score, otoscopy, nasal endoscopy, tubomanometry, and pure tone audiometry (PTA) were completely documented.
Exclusion criteria included the following
(1) History of Meniere’s disease (based on the guideline published in 2015 22 ) and temporomandibular joint dysfunction (TMJD, based on the diagnostic criteria published in 2014 23 ). Both of them can cause similar symptoms to ETD, and TMJD has been recognized as a potential confounding condition in patients presenting with ETD symptoms. 24
Data Collection
Patients’ demography (i.e., age, gender, and center), clinical history (i.e., onset time, diagnosis, chronic rhinitis, and chronic rhinosinusitis) were collected. Objective measurements, including otoscopy, nasal endoscopy, PTA, tympanogram, tubomanometry, and ETS-5 were recorded.
Sample Size
The sample size was calculated for multivariate analysis. A “rule of thumb” based on Monte Carlo simulations with different data sets suggests ≥5× as many cases as the number of items are required. 25 It was estimated that at least 20 ETD ears and 20 non-ETD ears were needed.
5-Item Eustachian Tube Score
ETS-5 contains the results of 3 different tubomanometry’s pressures and 2 subjective performances of positive Valsalva and Toynbee maneuvers. The positive Toynbee click during swallowing and the positive Valsalva maneuvers are scored as 0 points for “never,” 1 point for “sometimes,” and 2 points for “always.” The patient’s response should have persisted for at least the past 2 months. Tubomanometry (Spiggle & Theis, Overath, Germany) results at 30, 40, and 50 mbar are also included. Immediate opening of the ET (R < 1) scores 2 points, delayed opening (R > 1) scores 1 point, and no opening (negative or unmeasurable R) scores 0 points. A total score of all 5 items ≤5 indicates ETD. 16
Definition of Endoscopic Features
The endoscopic features refer to 3 items, including the size of the perforation, the location of the perforation, and the rating scale for mucosal inflammation of the Eustachian tube on the nasopharyngeal side.
The size of the perforation is defined as the ratio of the perforation area to the total area of the pars flaccida and tensa. The area is calculated as follows: 0% to 30%, 31% to 60%, 61% to 80%, 81% to 99%, and 100%.
The location of the perforation is classified into 5 types: posterior to the tensa, anterior to the tensa, in the middle of the tensa, pars flaccida, and subtotal to the tensa. In a perforation confined to the tensa of the tympanic membrane, the tensa is divided into anterior and posterior portions, with the malleus serving as the central axis. If more than 70% of the perforation area is in the posterior part of the tensa, it is considered to be in the posterior part of the tensa. If more than 70% of the perforation area is located in the anterior part of the tensa, it is considered to be located in the anterior part of the tensa. Otherwise, it is considered to be in the middle of the tensa. If the perforation area occupies 100% of the tensa, it means that the perforation is located in the subtotal of the tensa. If the perforation is confined in the pars flaccida, it is defined as being in the pars flaccida. If the perforation locates in both the pars flaccida and tensa, it is firstly considered to be in the pars flaccida unless it occupies 100% of the tensa simultaneously, in which case it can be considered to be in the subtotal of the tensa.
The grading scales for the mucosa inflammation of the ET in the nasopharynx proposed by Poe et al. are defined as follows: normal, mild edema or erythema, moderate inflammation with impaired dilatation, and severe inflammation with inability to open the lumen 26 (Supplemental Figure 1).
Diagnostic Criteria
Patients were clinically diagnosed with ETD if fitting both of the following conditions:
(1) At least 2 of the pressures’ results of tubomanometry indicated poor Eustachian tube function (R > 1 or R = 0) 27 .
(2) At least repeated 3 times that the Eustachian tube lumen partially dilated or failed to open more than 2 seconds28-30 after swallowing during nasal endoscope examination (Supplemental Figure 2).
Statistical Analysis
All results were analyzed using SPSS 28.0. (Chicago, IL, USA). Descriptive and frequentist statistics were calculated to describe patient demographics and characteristics. T test was used to compare means. Chi-square test was utilized to compare categorical variables. All significant variables were placed in a multiple logistic regression model with P < .05 being placed in a backward stepwise regression model. The nomogram was constructed by R software 4.3.2. The discrimination performance of the nomogram prediction model was evaluated using the area under the receiver-operating characteristic curve (AUC, ROC) and the consistency index (C-index). Calibration curves were created to evaluate the calibration of the nomogram prediction model. Decision curve analysis (DCA) was performed to determine the clinical utility of the nomogram. DCA curve showed the net benefits (y-axis) of the prediction model across various risk threshold probabilities (x-axis). The net benefit was calculated by taking the difference between the proportion of true positive patients and the proportion of false positive patients while considering the relative harm of forgoing interventions compared to the negative consequences of unnecessary interventions. The nomogram underwent bootstrapping validation with 1000 bootstrap resamples to calculate a relatively corrected C-index. 31 All reported statistical significance levels were 2-sided, and a threshold of P < .05 was considered statistically significant.
Results
Demographics and Characteristics
A total of 40 participants (40 ears) were recruited for the study. Patient demographics and characteristics were shown in Table 1. There was no statistically significant difference in age, gender ratio, onset time, smoking, drinking, PTA, and Air-Bone gap between COM with ETD group and COM without ETD group. Chronic rhinitis or rhinosinusitis (85.0% vs 25.0%, P < .001) were significantly more common in COM with ETD patients than in patients without ETD. R > 1 and R = 0 in each pressure of tubomanometry were found more often in patients with ETD than in those without ETD. Eustachian tube delaying open or no open (100% vs 5%, P < .001) was more common in patients with ETD compared with those without ETD.
Demographics and Characteristics.

Abbreviations: COM, chronic otitis media; ET, Eustachian tube; ETD, Eustachian tube dysfunction; PTA, pure tone audiogram; TMM, tubomanometry.
P < .05.
Univariate and Multivariate Binary Logistic Regression Analysis for Identification of ETD
Based on the information collected, we investigated the factors associated with ETD. Among the 10 variables collected, 3 potential factors including ETS-5 score (OR = 0.760, 95% CI 0.590-0.980, P = .035), ET mucosa inflammation of nasopharynx (OR = 9.074, 95% CI 2.269-36.288, P = .002) and SNOT-22 score (OR = 1.037, 95% CI 1.009-1.067, P = .010) were identified in the univariate analysis (Table 2). We then performed multivariate logistic regression analysis to examine these 3 factors. As shown in Table 2, the multivariate analysis finally indicated that the ETS-5 score (OR = 0.588, 95% CI 0.379-0.912, P = .018) and ET mucosa inflammation (OR = 28.128, 95% CI 3.268-242.103, P = .002) were independent predictors associated with ETD.
Univariate and Multivariate Logistic Regression for Diagnostic Factors of ETD in Patients with COM.
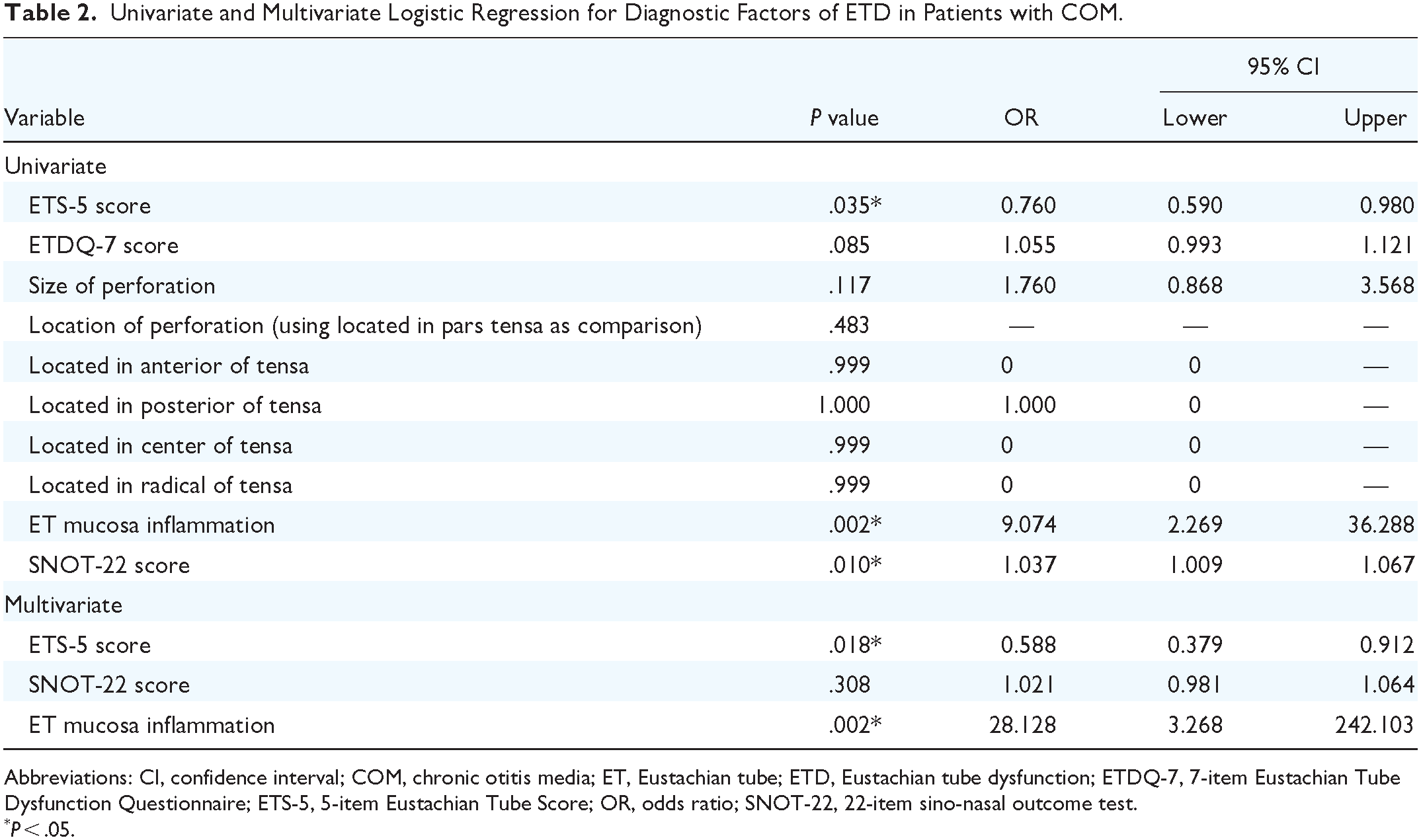
Abbreviations: CI, confidence interval; COM, chronic otitis media; ET, Eustachian tube; ETD, Eustachian tube dysfunction; ETDQ-7, 7-item Eustachian Tube Dysfunction Questionnaire; ETS-5, 5-item Eustachian Tube Score; OR, odds ratio; SNOT-22, 22-item sino-nasal outcome test.
P < .05.
Diagnostic Values of Different Diagnostic Methods in Patients with COM.

Abbreviations: AUC, area under the curve; COM, chronic otitis media; ET, Eustachian tube; ETS-5, 5-item Eustachian Tube Score.
P < .05.
Construction of Nomogram
The diagnostic equation built for the regression model was LogitP = −3.006 – 0.532 * ETS-5 score + 3.337 * ET mucosa inflammation, based on the multivariable logistic regression analysis, and the result was displayed as nomogram shown in Figure 1. In the nomogram, each factor was assigned a score (the numbers in brackets) based on its corresponding values or degrees (the numbers or classes on the axis). These scores were obtained by drawing a vertical line from each factor to the score axis. By calculating the total scores of the 2 variables, the likelihood of diagnosing a patient with ETD was visually demonstrated on the corresponding probability axis. For example, if a patient is evaluated with an ETS-5 score of 5 and moderate Eustachian tube mucosa inflammation, he or she will obtain a score of 27 for ETS-5 and 67 for mucosa inflammation. So, the total score of this patient is 94 on the axis yielding a probability of ETD over 0.98.

The nomogram diagnostic model to identify ETD in patients with tympanic membrane perforation. In the nomogram, each factor is assigned a score (the numbers in brackets) based on its corresponding values or degrees (the numbers or classes on the axis). These scores are obtained by drawing a vertical line from each factor to the score axis. By calculating the total scores of the 2 factors, the likelihood of diagnosing a patient with ETD is visually demonstrated on the corresponding probability axis. ETD, Eustachian tube dysfunction; ETS-5, 5-item Eustachian Tube Score; ET, Eustachian tube.
Diagnostic Value of Nomogram
The ROC curve of the nomogram prediction model was analyzed to evaluate the model’s diagnostic effect. The area under the curve (AUC) of the model was 0.901 (95% CI 0.801-1.000, P < .001), which was superior to 0.680 (95% CI 0.508-0.852, P = .051) in ETS-5 score, 0.831 (95% CI 0.697-0.965, P < .001) in ET mucosa inflammation, suggesting that the nomogram was superior to predict the probability of ETD (Figure 2). The sensitivity and specificity of the nomogram model were 80.0% and 90.0%, respectively, in identifying ETD, (Table 3) while comparing with a sensitivity and specificity of 60.0% and 65.0% in ETS-5 score and 85.0% and 80.0% in ET mucosa inflammation. The C-index for the diagnostic nomogram was 0.901 (95% CI 0.804-0.998), which suggested the model’s good discrimination. And the cutoff of the nomogram model was 0.657, suggesting that a patient with a nomogram’s probability over this cutoff could be diagnosed with ETD.
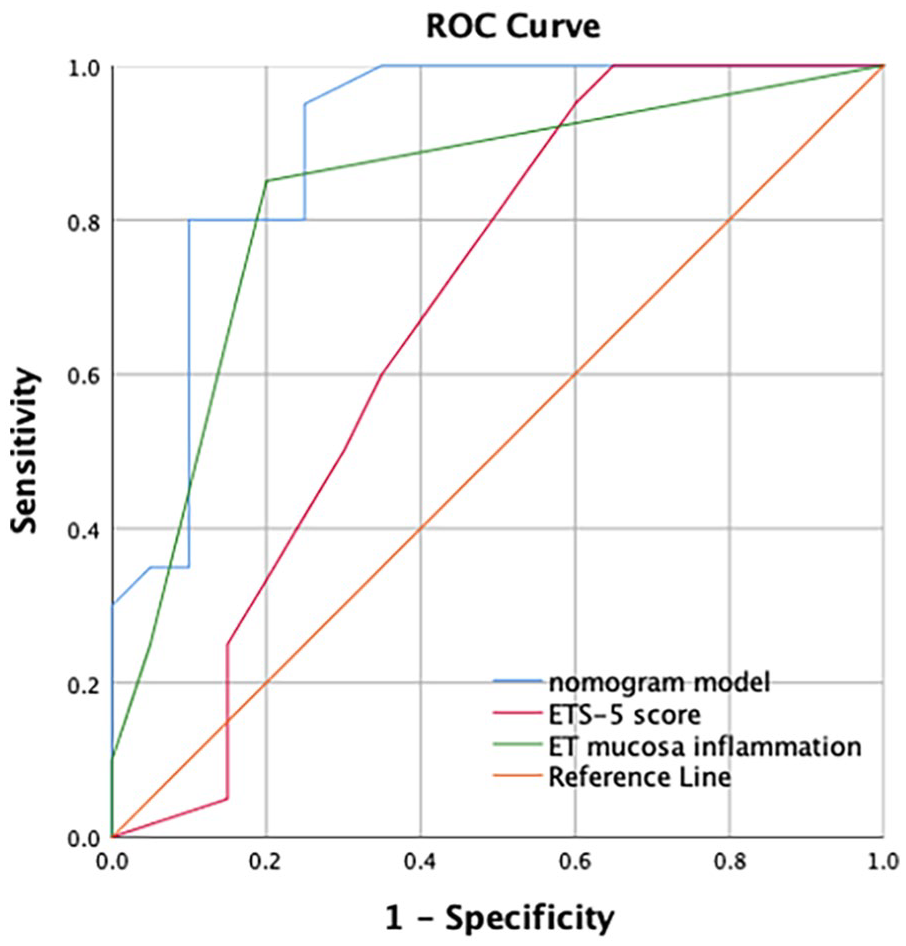
The ROC curve and the area under the curve of the nomogram model and independent diagnostic factors. ROC, receiver-operative characteristics; ETS-5, 5-item Eustachian Tube Score; ET, Eustachian tube.
Validation of Nomogram
After 1000 bootstrap resamples, the calibration curve was generated in this study. This curve showed that the predicted probability of nomogram was consistent with the actual probability and was close to the ideal line, indicating a good consistency and a high degree of calibration (Figure 3). The finding also showed that the nomogram model constructed with the above 2 factors had an accurate diagnostic value for identification of ETD.

The calibration belt for the nomogram. The curve shows that the predicted probability is consistent with the actual probability and is close to the ideal line, indicating good consistency and a high degree of calibration for the nomogram model. ETD, Eustachian tube dysfunction.
Clinical Use of Nomogram
DCA was performed to determine the clinical utility of the nomogram (Figure 4). To use this model for treatment decisions of ETD, a risk threshold was specified which we would treat if the probability of ETD calculated by the model was over this specific risk threshold. In our study, treatments referred to medical or surgical interventions for ETD in patients with CSOM and cholesteatoma. In this analysis, the nomogram model provided a higher net benefit than other models, including single ETS-5 model and single Eustachian tube mucosa inflammation model in almost all domains of threshold probability, suggesting that the nomogram model had better clinical practice.

The decision curve analysis for the nomogram. The y-axis represents the standardized net benefit, calculated by taking the difference between the proportion of true positive patients and the proportion of false positive patients. A risk threshold on x-axis is specified, which we would undertake treatment if the probability of ETD calculated by the nomogram model is over this specific risk threshold. The thick colorful lines represent the nomogram model, ETS-5 model, and ET mucosa inflammation model, respectively. The black solid line represents the assumption that no one is treated. The gray solid line represents the assumption that all patients are treated regardless of the diagnostic results. All models have superior net benefits than both treating no one and treating all patients in all domains of threshold probability. The nomogram model provides a higher net benefit than other models. ETD, Eustachian tube dysfunction; ETS-5, 5-item Eustachian Tube Score; ET, Eustachian tube.
Discussion
We believe this is the first time a disease-specific scoring system has been developed for ETD in patients with tympanic membrane perforation. This nomogram model provides subjective Valsalva and swallowing sensations, objective tubomanometry results, and endoscopic findings comprehensively and with good diagnostic ability. The instrument can contribute to identify ETD in patients with CSOM and cholesteatoma, making it possible to guide an early or concurrent intervention on ETD such as medical treatment and balloon Eustachian tuboplasty. 32
As we know, there are several objective measurements to diagnose ETD in patients with tympanic membrane perforation, such as inflation-deflation test, 10 methylene blue test, saccharine test, 11 temporal bone Valsalva computed tomography (CT), 33 video endoscopy, 30 and tubomanometry. But none of them can build a diagnostic gold standard. Clinicians often need to make a judgment by comprehensive evaluations. 11 For example, methylene blue test, saccharine test, Valsalva CT, and endoscopy can be used to evaluate the anatomical patency of ET, and pressure equalization tests and tubomanometry can be used to assess the middle ear pressure-regulation functions. However, methylene blue test, saccharine test, and inflation-deflation test were limited in measuring ET active opening ability, unlike tubomanometry could produce a mixed active and passive ET opening. 5 And there was still a lack of a specific reference range for CT in the assessment of ET stenosis. 34 Therefore, we finally selected endoscopic results combined with tubomanometry as the diagnostic method for ETD.
In our study, the original diagnostic criteria for ETD were determined by tubomanometry and endoscopic findings. It seemed to partially overlap with the factors of the nomogram model, leading to an overestimation of the capabilities of the new tool. For the original definition of ETD, the poor middle ear ventilation was defined by at least 2 of the pressures’ results of tubomanometry indicating poor Eustachian tube function. The mechanical obstruction of ET was assessed by the ET lumen dilation state, either delayed opening or not opening. For the parameters in multivariate analysis, we used quantitative scoring systems, including ETS-5 and Eustachian tube mucosal inflammatory grading scale, both being the developments of the original definition of ETD, more comprehensively and easier to record. Thereby, in this view, we tried to develop and validate a superior diagnostic method but not to generate a totally new technique for ETD identification.
Our study included patients with CSOM and cholesteatoma. All of them were with tympanic membrane perforation to explore the association between ETD and the characteristics of perforation. We found there was no statistical association between ETD and perforation features, which indicated that we could try to explore the applying scope of the model in patients with intact tympanic membranes. Regarding nasal endoscopy, we suggested that patients with CSOM and cholesteatoma should undergo the examination unless the patient refused to do so. It should be noted that this endoscopic finding depends on the judgment of the operator and the evaluator. Therefore, it is recommended that the assessment is performed by at least 2 clinicians.
In this study, we also recorded the symptoms assessments to identify ETD in patients with tympanic membrane perforation. Since 2012, the ETDQ-7, a validated symptomatic measure of ETD developed by McCoul et al, has been used in several countries as a screening tool as well as an outcome measure in both clinical and research settings.14,24 A systematic review by Andresen et al showed that the ETDQ-7 had a sensitivity of 91% to 100% and a specificity of 67% to 100% with an AUC of 0.94 to 1.00 in patients who had already undergone tympanometry. From previous studies, the ETDQ-7 score was excellent at distinguishing patients with ETD from healthy controls in patients with intact tympanic membranes. The reason could be that the symptoms of ETD were attenuated by the perforation, so that the score for ETD was not relevant in patients with tympanic membrane perforation. In contrast, tubomanometry has a wider scope. The concept of tubomanometry is the controlled delivery of defined pressures of 30, 40, and 50 mbar into the nasopharynx through a nasal applicator. 16 Tubomanometry is feasible even in the presence of tympanic membrane perforation and provides specific information about the dynamics of the Eustachian tube. 35 ETS-5 as an extension of tubomanometry serves as a reliable and effective objective assessment of Eustachian tube function. 5 In previous studies, analysis of the ETS-5 score alone yielded an AUC of 0.67 to 0.73 with a sensitivity of 48% to 72% and a specificity of 53% to 90% when the positive cutoff value was 4.5 to 5.0.16,18 However, in the current study, the ETS-5 performed better when used as part of the nomogram rather than as the sole ETS-5 in patients with tympanic membrane perforation. This may be due to the increased sensitivity of the tubomanometry to the middle ear pressure in patients with tympanic membrane perforation, which will overestimate the ET function in delayed opening so that affect the sensitivity of sole ETS-5.
Most importantly, this nomogram model can assess ETD in patients with chronic rhinosinusitis. Meanwhile, several previous studies have demonstrated the association between chronic rhinosinusitis and ETD.36,37 Chronic rhinosinusitis and allergic rhinitis have been shown to be 2 important factors leading to ETD.19,38 Functional endoscopic sinus surgery has been proved to be associated with the improvement of ETD symptoms. 24 Therefore, it is beneficial to have testing devices that are suitable for people with nasal conditions. Consistent with our study, Vandersteen et al. have shown that tubomanometry was a promising new tool for the assessment of ETD and could be incorporated into the clinical evaluation of patients with chronic rhinosinusitis. 39 Our new measurement incorporates tubomanometry and is applied to patients with or without chronic rhinosinusitis.
Several limitations should be noted with this study. First, this is a prospective study with a relatively small number of patients. The development and validation of the new instruments was limited to preoperative data. Therefore, the interpretation and value of our study are limited. Further prospective multicenter studies are needed to validate this new tool. Second, the partial overlap between the original definition of ETD and the factors in multivariate analysis made the nomogram model lack comparisons with other objective methods, which was unavoidable to overemphasize the capability of the new tool. Finally, in the context of the current data, we could not demonstrate that it is possible to measure short- and long-term outcomes with this new tool.
Conclusions
The nomogram diagnostic model is effective and reliable in identifying ETD in patients with tympanic membrane perforation. Further prospective and long-term studies are needed to demonstrate its clinical and scientific value.
Supplemental Material
sj-png-1-ohn-10.1177_19160216241293068 – Supplemental material for A Nomogram Diagnostic Model for Eustachian Tube Dysfunction in Patients with Tympanic Membrane Perforation
Supplemental material, sj-png-1-ohn-10.1177_19160216241293068 for A Nomogram Diagnostic Model for Eustachian Tube Dysfunction in Patients with Tympanic Membrane Perforation by Xiaoxin Chen, Michael C. F. Tong and Wai Tsz Chang in Journal of Otolaryngology - Head & Neck Surgery
Supplemental Material
sj-png-2-ohn-10.1177_19160216241293068 – Supplemental material for A Nomogram Diagnostic Model for Eustachian Tube Dysfunction in Patients with Tympanic Membrane Perforation
Supplemental material, sj-png-2-ohn-10.1177_19160216241293068 for A Nomogram Diagnostic Model for Eustachian Tube Dysfunction in Patients with Tympanic Membrane Perforation by Xiaoxin Chen, Michael C. F. Tong and Wai Tsz Chang in Journal of Otolaryngology - Head & Neck Surgery
Footnotes
Acknowledgements
We thank for the technical support of the audiologists from The Chinese University of Hong Kong.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Additional supporting information is available in the online version of the article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.