
Abstract
Keywords
Introduction
Chronic suppurative otitis media (CSOM) refers to prolonged inflammation of the mucosae in the middle ear and mastoid cavity. 1 CSOM is characterized by recurrent discharge through a perforation in the tympanic membrane, often resulting in long-term, permanent alterations to the tympanic membrane, such as atelectasis, perforation, tympanosclerosis, the formation of retraction pockets, or the development of cholesteatoma. 2 The goal of tympanoplasty is to repair tympanic membrane perforation (TMP) through grafting and/or ossicular reconstruction, eliminate middle ear inflammation, and improve hearing. 3 Endoscopic tympanoplasty provides minimally-invasive transcanal access to the middle ear and improves visibility for the treatment of CSOM. 4 There are several factors influencing the success rate of tympanoplasty, encompassing patient age, perforation size, eustachian tube function, the duration of ear canal secretions, different types of graft materials employed, and the presence of infectious secretions during the surgical procedure. 5 Otomycosis is a superficial fungal infection of the external ear canal that is frequently seen in primary care and otolaryngology practices. 6 Aspergillus and Candida species are the most commonly-identified fungal pathogens. 7 The extensive use of topical antibiotic ear drops and steroids in patients with CSOM can lead to otomycosis. Otomycosis with TMP is difficult to treat in clinical practice. Due to the narrow ear canal, the patient may have difficulty applying the antifungal ointment to the outer ear canal by themselves. Antimycotic solutions are irritant to middle ear and may be ototoxic to the cochlea. 8 In such cases, myringoplasty may be required. However, otomycosis was considered an important factor affecting the success of myringoplasty. It remains controversial whether CSOM patients with otomycosis are good candidates for myringoplasty. In our previous study, we have found that the graft success rate and hearing improvement were not affected by otomycosis. However, the cases were only 25 patients. 9 Therefore, in the study, we increased the number of cases. Our aim was to observe the outcomes of tympanoplasty in patients with otomycosis on the ground of success of graft uptake and the hearing improvement.
Materials and Methods
Study Population
This retrospective study comprised a total of 431 patients clinically diagnosed with CSOM who underwent endoscopic type 1 tympanoplasty at the Affiliated Eye, Ear, Nose and Throat Hospital of Fudan University from January 2020 to October 2023. Patients meeting the following criteria were included: (1) age ≥12 and ≤70 years, (2) TMP caused by otitis media, (3) endoscopic myringoplasty (over-underlay technique) using cartilage with a single-sided perichondrium, (4) primary ear surgery, and (5) at least follow-up duration of 3 months. The exclusion criteria included the following: (1) missing data, (2) cholesteatoma, (3) ossicular chain abnormalities, and (4) uncontrolled diabetes and hypertension. Forty-four patients were excluded. The 387 patients with CSOM were divided into the control group (group 1, n = 203, without otomycosis) and the trial group (group 2, n = 184, with otomycosis). The patients’ demographics, clinical characteristics, and otologic history including age, sex, admission duration, time of onset, size of perforation, endoscopic images, and hearing outcomes were collected. The size of TMP was estimated as follows: (1) small (S) for perforation less than 1/3 of tympanic membrane surface (TMS), (2) medium (M) for perforation between 1/3 and 2/3 of the TMS, and (3) large (L) for perforation more than 2/3 of the TMS. 10
The study was approved by the Institutional Review Board of Eye & ENT Hospital, Fudan University, Shanghai, China (approval number 2020131) and registered in the Chinese Clinical Trial Registry (ChiCTR2100042154).
Surgery and Follow-Up
All surgeries were performed by 2 experienced otologists. After the general anesthesia and before the initiation of surgery, the ear canal debris and exudate were collected by using sterilized cotton swabs, which were sent to the microbiology laboratory for fungal and bacterial culture and drug sensitivity within 30 minutes. Then, the fungal crusts in the external auditory were cleared and disinfected with povidone-iodine for 3 times. All patients underwent endoscopic type 1 tympanoplasty with the graft of full-thickness tragus cartilage covered by one side of the perichondrium. The ear canal was filled with a gelatin sponge impregnated with fluconazole or voriconazole. All patients were followed up in our outpatient clinic at the 3rd week, 3rd month postoperatively. Subjects in both groups were followed up for a minimum period of 3 months. The external auditory canal and tympanic membrane were examined every time. Pure-tone audiometry (PTA) was assessed preoperatively and at the 3rd month postoperatively. PTA was calculated as the average of the 500, 1000, 2000, and 4000 Hz frequencies. The air-bone gap (ABG) was also analyzed for each patient pre- and postoperatively. The primary outcome was closure of the perforation. Secondary outcomes were audiometric results and persistent postoperative otomycosis.
Statistical Analysis
All statistical analyses were performed with SPSS ver. 26.0. The measurement data were expressed as mean ± standard deviation (x ± s), and when comparing between groups, Student’s t-test (normal distribution) or the Mann-Whitney U test (non-normal distribution) was used. A paired t-test was performed for audiological comparison. Chi-squared test or Fisher’s exact test was used to compare categorical variables between the 2 groups. A P-value <.05 was considered to indicate statistical significance.
Results
There were 79 male and 105 female patients in the trial group, with an average age of 45.88 ± 12.54 years old. There were 78 male and 125 female patients in the control group, with an average age of 43.80 ± 12.87 years old. There was no statistically-significant difference in patient age, gender, duration, and TMP size between the 2 groups (Table 1). We reviewed the records of 184 patients in the trial group. Eleven of these patients were not cultured, and fungi were not detected in 68 patients. One hundred five patients had culture-proven fungal otitis externa (11 Candida albicans, 87 Aspergillus and 7 filamentous fungi). Thirty-two of the 105 patients had mixed infection of fungi and bacteria, and the most common mixed infection of bacteria was Staphylococcus epidermidis (9/32).
General Features of Enrolled Patients.

Abbreviation: TMP, tympanic membrane perforation; S, small; M, medium; L, large.
The graft success rate in the trial group was 94.57% and the control group was 96.06% (P = .486) (Table 2). There was no significant difference in the 2 groups. Failed graft uptake was seen in 10 cases in the trial group, 5 cases of postoperative persistent fungal infection, 3 cases of marginal perforation due to cartilage collapse, and 2 cases of bacterial infection. In the control group, there were 8 cases of unhealed tympanic membrane, including 3 cases of postoperative infection and 5 cases of marginal perforation caused by cartilage collapse. No patient presented severe hearing loss or facial paralysis for 3 months after the surgery. Figure 1 shows a representative tympanic membrane preoperatively and at the 3rd month postoperatively.
Graft Uptake of 2 Groups.
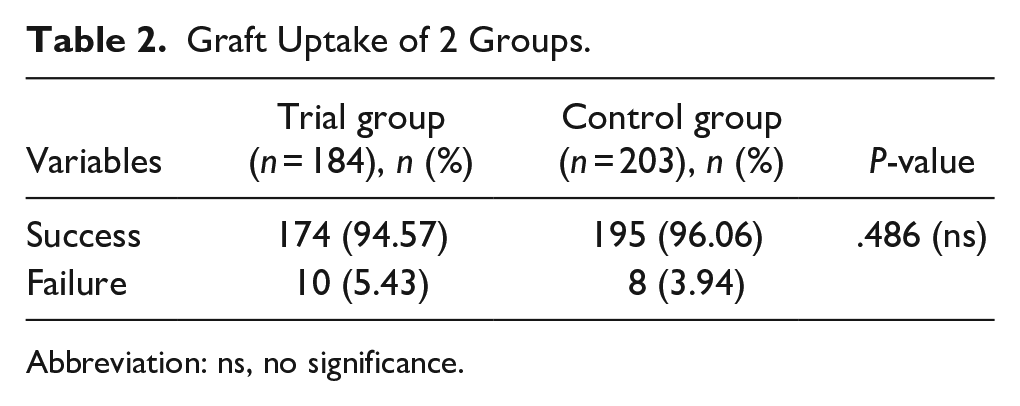
Abbreviation: ns, no significance.
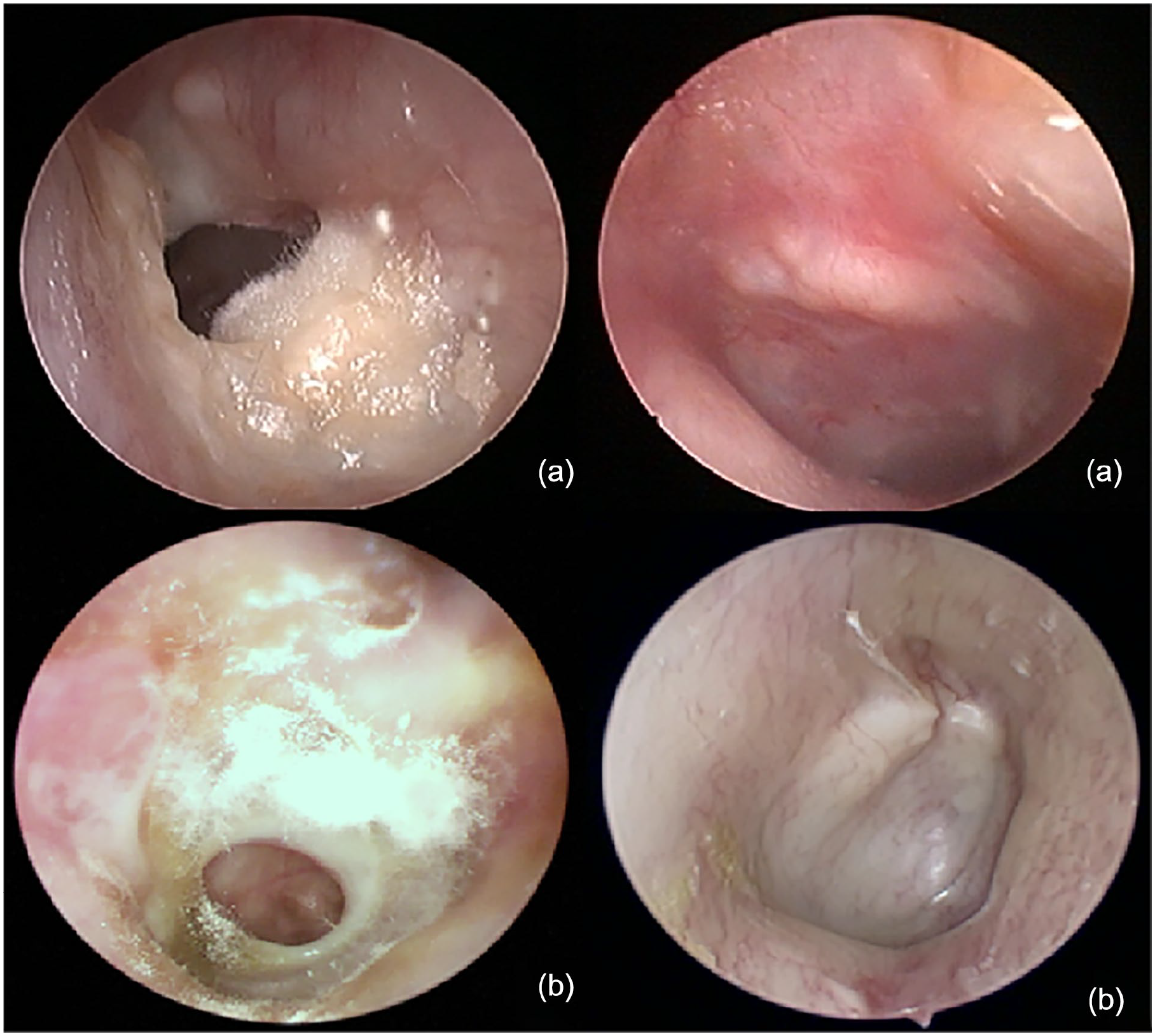
Two representative tympanic membranes preoperatively (a) and at the 3rd month postoperatively (b).
Preoperative and postoperative ABG and AC were compared by the Mann-Whitney U test, and their power values (1 − β) were all close to 1. The postoperative mean ABG and AC in both groups were significantly lower than that before the operation (P < .001), while no significant difference was observed in the preoperative AC (P = .992) and ABG (P = .151) of the 2 groups (Table 3). The 2 groups did not exhibit any significant differences in pre- or postoperative hearing results (including AC and ABGs) at any single frequency (125, 250, 500, 1000, 2000, 4000, and 8000 Hz). The comparison in AC and ABGs changes between the 2 groups did not show any significant difference at all frequencies (Figures 2 and 3). Postoperatively, the improvements in the postoperative AC levels were 8.82 ± 10.44 dB in the trial group and 9.67 ± 9.07 in the control group (P = .649). The change in mean ABG was 3.34 ± 7.96 dB in the trial group and 3.96 ± 7.20 dB in the control group, showing no significant difference (P = .420) (Table 3).
Hearing Conditions of 2 Groups Before and After Operation (Mean ± SD, dBHL).
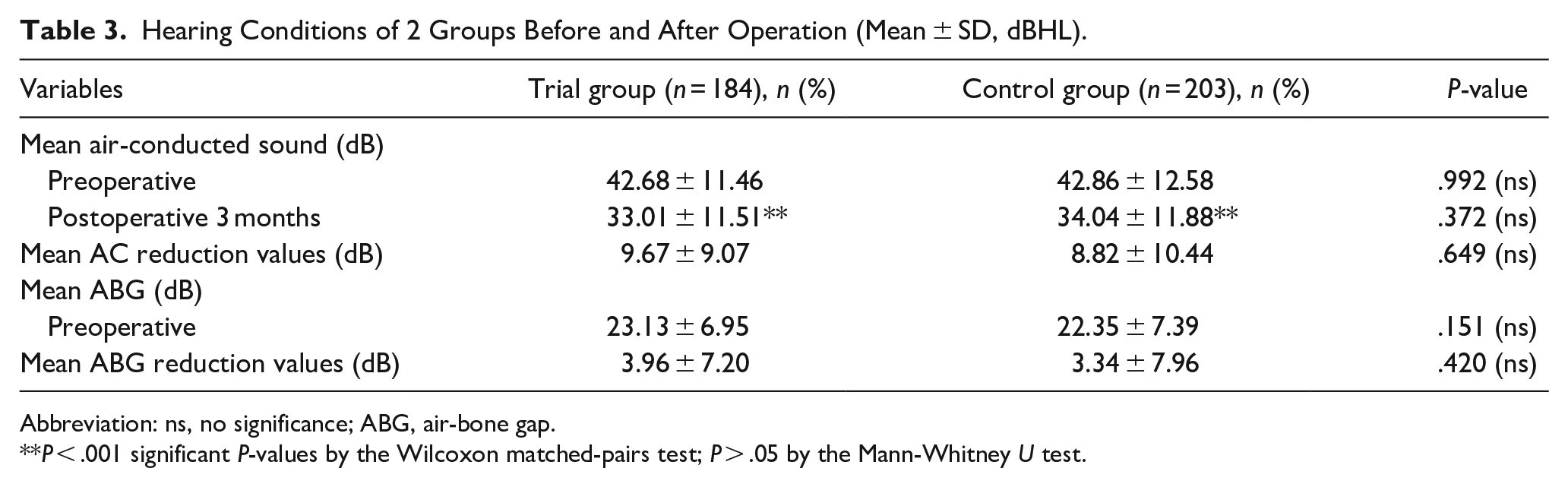
Abbreviation: ns, no significance; ABG, air-bone gap.
P < .001 significant P-values by the Wilcoxon matched-pairs test; P > .05 by the Mann-Whitney U test.
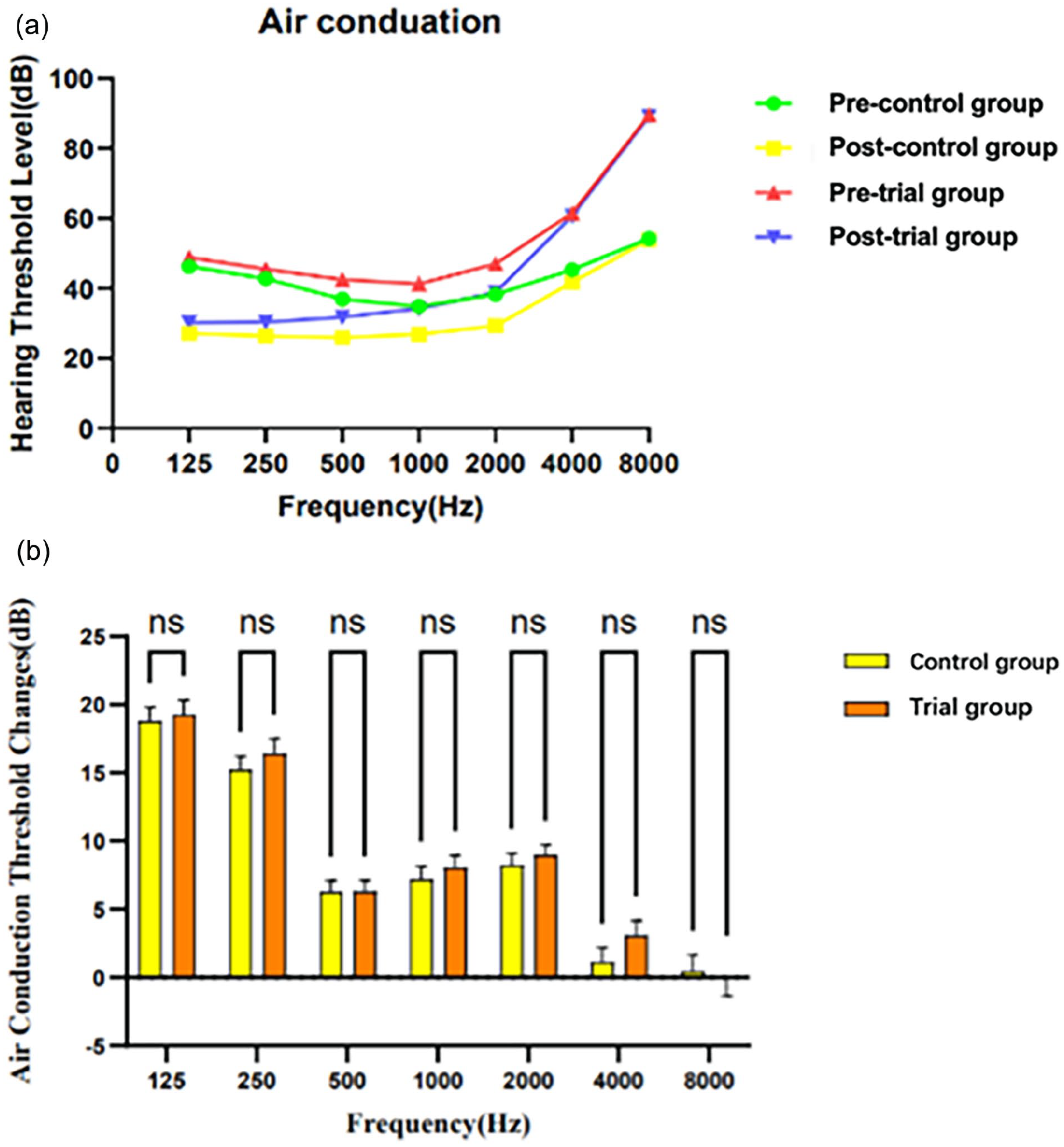
Comparison between frequency-specific hearing results in air conduction. (a) Pre- and postoperative average air conduction between the trail group and the control group at each frequency. (b) Air-conduction change at each frequency. A positive value indicates improvement. Data are shown as mean with SEM. ns, no significance, P > .05 by the Mann-Whitney U test. SEM, standard error of mean value.
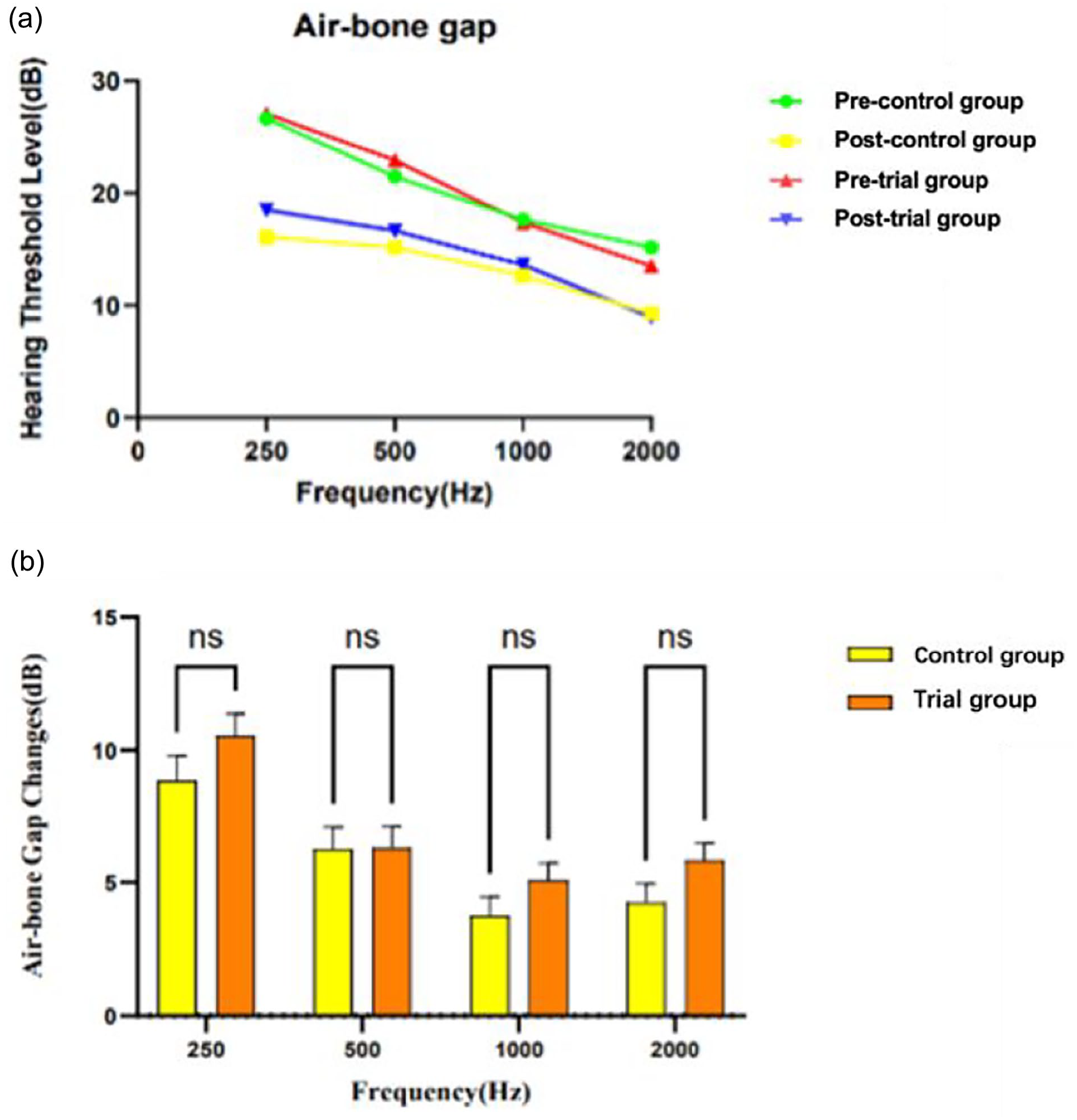
Comparison between frequency-specific results in air-bone gap. (a) Pre- and postoperative levels in air-bone gap. (b) Frequency-specific reduction values in air-bone gap. A positive value indicates improvement. Data are shown as mean with SEM. ns, no significance, P > .05 by the Mann-Whitney U test.
According to Fisher’s exact test, in the trial group, no significant differences in graft uptake among variables such as age, duration, TMP size, fungal type was found (P = .848, .389, .189, and .491, respectively). In the trial group, 127 patients had no postoperative fungal infections, among whom 5 had unhealed tympanic membrane. Additionally, there were 57 patients with fungal infection, including 5 cases of failed graft uptake and the difference was not statistically significant (Table 4). For patients found to have persistent fungal infections at the 3rd week postoperative follow-up, fluconazole or voriconazole ear drops were administered.
Differences in Graft Uptake Among Variables in the Trial Group.
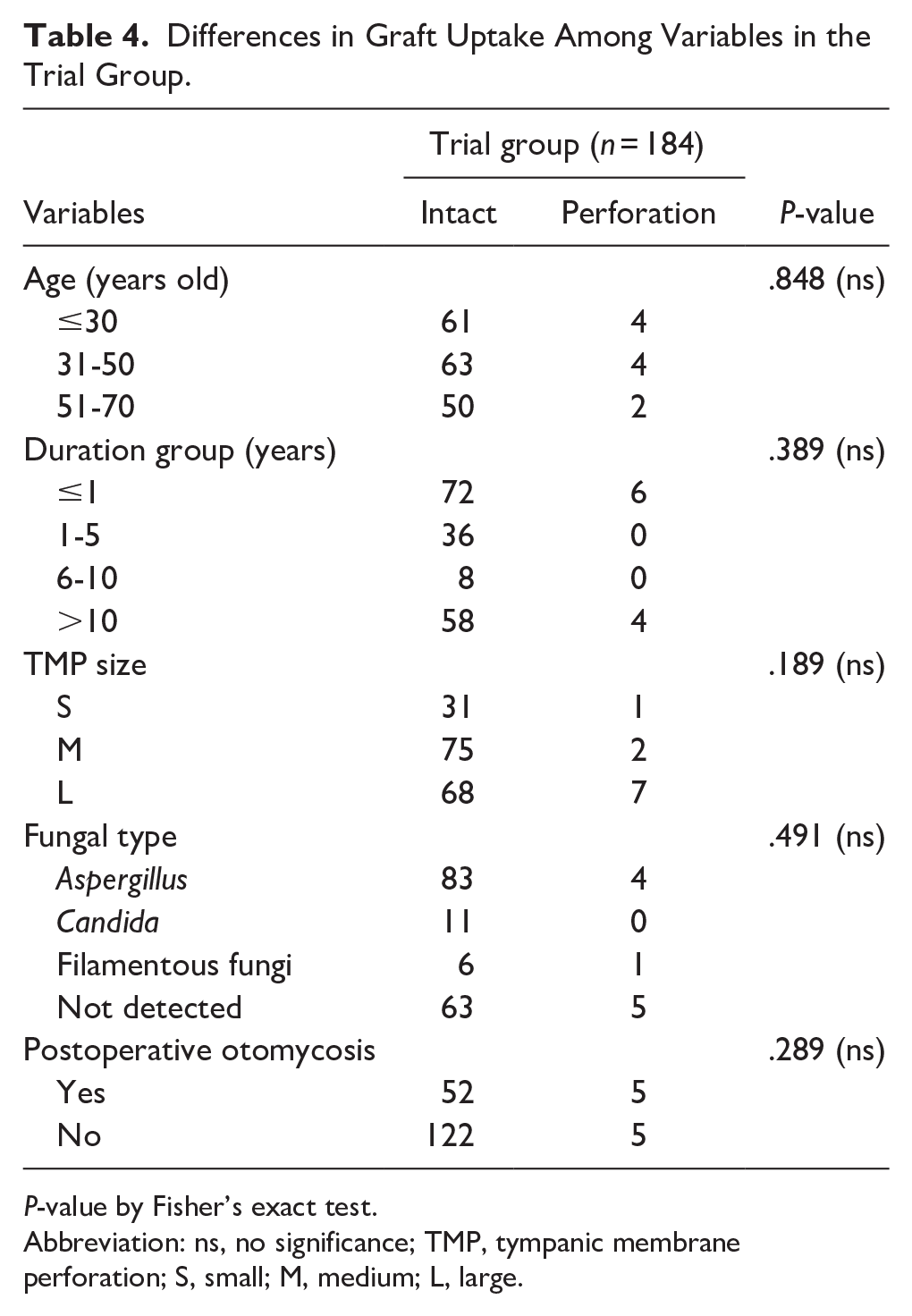
P-value by Fisher’s exact test.
Abbreviation: ns, no significance; TMP, tympanic membrane perforation; S, small; M, medium; L, large.
Discussion
Endoscopic type 1 tympanoplasty results in treatment outcomes comparable to those of microscopic myringoplasty with respect to graft success rate and ABG. However, endoscopic approach was significantly associated with shorter operative time, more self-rated excellent cosmetic results, and lower pain VAS. 11 Furthermore, a previous study showed that endoscopic transcanal type 1 cartilage tympanoplasty achieved a high graft success rate, significant gap gain, and improved hearing results, regardless of the perforations’ location and size. 12 In our study, all patients underwent endoscopic type 1 tympanoplasty using tragal cartilage with a single-sided perichondrium and achieved distinct improvements in hearing. The results showed that the graft success rate was 94.57% in the trial group and 96.06% in the control group.
Whether surgery can be performed for CSOM with otomycosis has been controversial. There were no statistically-significant differences in postoperative mean hearing gain and graft uptake between active and inactive otitis media patients undergoing tympanoplasty. Hence, tympanoplasty procedures should not be postponed solely because of patients’ preoperative ear discharge status. 13 Yang et al. 14 reported that mucoid ear discharge has no adverse effect on the outcome of the operation as regard to graft uptake and hearing gain. However, the repairing of the TMP with otomycosis is an intractable issue and a technical challenge. 15 The overmuch cream is accumulated in the external auditory canal, which may further result in the wet environment and thereby worsen the otitis externa with otomycosis. 16 Although most cases of fungus caused TMP resolve with proper medical treatment, in a few patients a tympanoplasty may be required. 17 Lin et al. 18 found that 50% of patients with otomycosis had worse hearing after surgery compared with 17.7% of those without otomycosis; however, there was no statistical significance in this study, which may be due to the small sample size. These findings should be verified with a large series. It is sometimes difficult to distinguish between otomycosis developing secondarily to a perforation and a perforation with CSOM developing secondarily to otomycosis. 19 The most widely used treatment regimen for otomycosis is mechanical debridement of the ear canal along with antifungal medication. 20 According to the present study, currently available 5% povidone-iodine did not affect hearing and, therefore, can be comfortably used for preparation and disinfection in otologic surgeries. 21 When dealing with patients with middle ear effusion and fungal infections in the ENT outpatient department, we provide drug interventions. However, when the fungus of the external auditory canal was dry and the middle ear cavity was no infection, we typically proceed with cleanup alone, without medication. Occasionally, ear discharge in patients with CSOM is difficult to control with drug treatment alone and often recurs preoperatively. There is a certain waiting period between the outpatient appointment and the scheduled surgery. In some cases, patients may show no signs of fungal infection at the time of registration, yet upon admission to the hospital, fungi were detected in their ear canal. Unless there was active discharge, we usually did not suspend the operation, but thoroughly clean the fungal hyphae and crust during the operation, and perform 5% povidone-iodine soaking, as described in Materials and Method. Our previous research found that the graft success rate and hearing improvement were not affected by a wet middle ear and otomycosis, 9 like the results of this study.
Fungi are commonly present in chronically-discharging ears. The diagnosis of otomycosis is usually made on clinical grounds, as the characteristic appearance of the fungal fruiting bodies are easily recognizable through an otoendoscopy. Indeed, we sometimes did not confirm whether the residual fungal mycelia were completely eradicated. Notably, it is necessary to culture fungi and bacteria and to test drug sensitivity before and during operation. In our study, the fungal detection rate stood at 60.70%, with Aspergillus comprising the most significant proportion. Among the 105 patients with confirmed fungal infections, 32 exhibited concurrent bacterial infections. The healing rate of the tympanic membrane was unaffected by the specific fungal infection. However, Lou, Z reported that 9.5% of patients exhibited recurrent otomycosis after 4 weeks, even after the topical application of compound ketoconazole cream, resulting in reperforations. 19 Compared to our results, the reported ratio appears higher, which might be attributed to our relatively-shorter follow-up period. Although our data suggested that myringoplasty with fungal infection of the external auditory canal has no difference in graft uptake and hearing improvement compared with the control group, preoperative medication control is still imperative for patients exhibiting definitive signs of acute infection. We do not consider it a contraindication for patients with fungus confined to the external auditory canal for type 1 tympanoplasty. Nonetheless, our findings require further refinement, and an extended follow-up period is necessary.
Limitation
As a retrospective study, our research is inherently subject to selection bias and potential confounding factors that may not have been fully controlled for in the analysis. The use of gender and age-matched controls would strengthen the study. A prospective, randomized controlled trial is warranted to validate our findings with higher quality evidence. The outcomes of this study were limited to 3 months of follow-up. Additionally, due to the insufficient sample size, there was a possibility that actual differences were not detected. We would like to report the outcomes again in the future when we have more patients with a long-term follow-up.
Conclusion
Patients with chronic otitis media could obtain a high success rate of tympanic membrane repair regardless of otomycosis. Whether fungal infection or not, hearing improvement after endoscopic type 1 tympanoplasty has a significant effect. CSOM with otomycosis is not a contraindication for type 1 tympanoplasty under the oto-endoscope. Intraoperative repeated rinsing with povidone-iodine may reduce the occurrence of postoperative infection.
Footnotes
Acknowledgements
We collected the clinical data from the Department of Otorhinolaryngology, Eye & ENT Hospital, Fudan University, Shanghai, People’s Republic of China. We thank them for this support.
Author Contributions
Linglan Gu, MD: data acquisition, literature research, data interpretation, manuscript preparation, manuscript definition of intellectual content, and manuscript editing. Yuhui Deng, MD: literature research, data interpretation, manuscript preparation, and manuscript editing; Wuqing Wang, MD: manuscript defnition of intellectual content. Ying Zhou, MD: statistical analysis; Dongdong Ren, MD: guarantor of integrity of entire study and study concepts; Jianghong Xu, MD: study design, manuscript revision/review, and manuscript final version approval.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the National Natural Science Foundation of China (NSFC; Grant Nos. 82271166 and 81970880 to D.R.) and Natural Science Foundation of Shanghai (Grant No. 22ZR1410100 to D.R.).
Ethical Approval
This study was reviewed and approved by Institutional Review Board of Eye & ENT Hospital, Fudan University, Shanghai, China (approval number 2020131) and registered in the Chinese Clinical Trial Registry (ChiCTR2100042154) and conducted in compliance with the Declaration of Helsinki.