
Abstract
Objective
Hemangioma is a common benign tumor in the head and neck. The therapeutic effect by conventional treatment was not very satisfactory. The purpose of this study is to explore the surgical strategy of low-temperature plasma radiofrequency in the treatment of hemangioma located in the nasal cavity, pharynx, and larynx.
Methods
The clinical data of 29 cases with hemangioma in nasal cavity, pharynx, and larynx treated by low-temperature plasma radiofrequency ablation were retrospectively analyzed. The strategy of ablation before resection was performed for 16 cases of nasal capillary hemangioma. The other 13 cases of cavernous hemangioma in the pharynx and larynx were treated by the strategy of direct ablation.
Results
All 29 patients underwent a successful operation with minimal intraoperative bleeding and no postoperative bleeding complications. There was no nasal septum perforation, dyspnea, dysphagia, dysphonia, or other complications. The patients were followed up for more than 3 years without recurrence.
Conclusion
Low-temperature plasma radiofrequency is a practical, minimally invasive, and accurate method for treating hemangiomas in the nasal cavity, pharynx, and larynx. For capillary hemangiomas, the strategy of ablation before resection may be an effective way to reduce bleeding, and for cavernous hemangiomas, the strategy of direct ablation is a simple and efficient method.
Introduction
Hemangioma is one type of benign tumor originating from vascular tissue of the mucosa, skin, muscle, gland, or bone, which is common in the head and neck, 1 and it is reported that hemangioma is one of the most common benign tumors in the nasal cavity. 2 Generally, hemangiomas are divided into 2 types: capillary hemangiomas and cavernous hemangiomas. There are a variety of treatment methods for hemangiomas, such as radiotherapy, laser treatment, microwave, local injection of pingyangmycin, surgical excision, and so on. During the last 10 years, the application of low-temperature plasma radiofrequency technology in the treatment of hemangiomas in the head and neck has achieved good results, with the advantages of simplicity, minimal invasion, and less bleeding.3,4 However, there are no reports on low-temperature plasma radiofrequency ablation strategies for different types of hemangiomas in the head and neck. In this study, we retrospectively reviewed 29 cases of hemangiomas occurring in the nasal cavity, pharynx, and larynx, and discussed the surgical strategy of low-temperature plasma radiofrequency in the treatment of different types of hemangiomas.
Methods
Subject and Ethic Statement
The medical records of 29 consecutive cases of hemangioma in nasal cavity, pharynx, or larynx in our hospital were retrospectively reviewed from January 2013 to December 2017. Patients were eligible for inclusion in the study if they were over 18 years old; in good health; diagnosed with hemangioma by clinical history, nasal endoscopy, or electronic laryngoscope. None had previous surgery for hemangioma. All patients were treated by low-temperature plasma radiofrequency ablation.
Surgical Procedure
Each patient was in the supine position. All operations were under general anesthesia through orotracheal intubation and performed by the same physician (HTZ). Surgery under an endoscopic endonasal approach was adopted for hemangiomas in the nasal cavity. A Davis mouth-gag was essential to reveal hemangiomas in the pharynx. Hemangiomas in the larynx were removed under a self-retaining laryngoscope. The Coblator II low-temperature plasma radiofrequency system (ArthroCare Corporation, Austin, TX, USA) was used in the surgery, and the coblation plasma wands EIC8872#, 5874#, and 7070# were selected for the treatment of hemangiomas in nasal cavity, pharynx, and larynx, respectively.
We performed different surgery strategies for capillary hemangiomas and cavernous hemangiomas. The method of ablation followed by resection was used for capillary hemangiomas of the nasal cavity, the plasma wand with the ablation function was used on the tumor and then the dark red tumor became grey and reduced; the base of tumor appeared subsequently, the base of the tumor and surrounding mucosa were then removed, and hemostasis was performed by this plasma wand for coagulation function (typical case 1). For cavernous hemangiomas in the pharynx or larynx, a direct ablation method was used instead of a method to remove the tumor, the plasma wand ablation was carried out gradually from the outer portion of the tumor to the center, and the swelling tumor body was reduced quickly and finally became flattened (typical case 2 and 3).
Postoperative Treatment
Medical care after operations for nasal hemangiomas were similar to that of other endoscopic endonasal surgeries, including nasal saline rinsing and nasal hormone spray to promote mucosal repair. The main treatment for pharyngeal and laryngeal hemangiomas after surgery was nebulization with budesonide.
Outcome Measures
We mainly observed the following indicators during and after operation: (1) whether the bleeding during the operation was uncontrollable and so another surgical procedure was requisite; (2) whether a severe hemorrhage occurred after the operation, (3) whether a secondary surgery was needed; (4) whether there were some complications such as nasal septum perforation, dyspnea, dysphagia, or dysphonia; and (5) whether patients were found to have a recurrence during routine postoperative follow-up.
Results
Patients’ Basic Clinical Characteristics
In the 29 cases, including 7 male patients and 22 female patients, the median age was 51 years, ranging from 31 to 63 years old. There were 16 patients with a hemangioma in the nasal cavity, which were clinically diagnosed as capillary hemangiomas and confirmed by histological examination after surgery. These tumors were located in different parts of the nasal cavity: nasal septum (10 cases), inferior turbinate (4 cases), and middle nasal meatus (2 cases). The other 13 cases of hemangioma were in the larynx and pharynx, which were clinically diagnosed as cavernous hemangiomas. There were no histopathological specimens since the hemangioma was completely ablated. The bases of the tumors were also located in different parts of the laryngopharyngeal cavity: posterior separate pharyngeal wall (4 cases), separate lateral wall of pharynx (3 cases), trans-tonsil and lateral pharynx wall (2 cases), trans-lateral pharynx wall and tongue base (1 case), laryngeal surface of the epiglottis (2 cases), and the trans-laryngeal surface of the epiglottis and laryngeal ventricle (1 case).
Overall Outcome
Operations on all 16 cases of nasal hemangioma were performed using the method of ablation followed by resection. Bleeding occurred when the tumor base was removed, and the plasma wand was used to stop bleeding by coagulation, with a total blood loss of about 2-5ml. Operations on other 13 cases of laryngopharyngeal hemangioma were performed under the method of direct ablation, and there was almost no intraoperative bleeding. These 29 cases achieved success after a one-off operation, and there was no postoperative bleeding, nasal septum perforation, dyspnea, dysphagia, dysphonia, or other complications. The patients were followed up for more than 3 years without recurrence. The following are 3 typical cases of hemangioma in the nose, pharynx, and larynx.
Typical Cases
Case 1
A 31-year-old woman was admitted to the hospital for repeated left nasal cavity bleeding and progressive nasal congestion in June 2017 for one month after delivery. Nasal endoscopy showed a dark red, smooth neoplasm congesting the left nasal cavity (Figure 1A). The paranasal sinus computed tomography (CT) scan revealed a homogeneous neoplasm with distinctive boundaries on the anterior central part of the left nasal cavity and a left-deviated nasal septum (Figure 1B and C). The neoplasm was clinically diagnosed as a hemangioma, and the surgical strategy of ablation followed by resection was adopted. Under the endoscopic endonasal approach, the plasma wand was placed close to the tumor body for ablation and from the anterior, anterosuperior, and anteroinferior parts of the tumor body, the tumor was gradually reduced in size (Figure 1D). Then, the basal part was exposed on the nasal septum, and plasma radiofrequency resection of the tumor along the tumor base continued (Figure 1E). Bleeding on the base was stopped using a power setting of 4 with the coagulation system (Figure 1F). Four weeks after the operation, the white membrane on the nasal septum surface was exfoliated, and the mucosa was smooth (Figure 1G). The clinical data of case 1. A, Nasal endoscopy showed the neoplasm congesting the left nasal cavity. B and C, The axial, B, and coronal, C, CT scan revealed a homogeneous neoplasm in the left nasal cavity. D, The tumor was shrunk by using the ablation strategy of low-temperature plasma radiofrequency. E, The tumor was totally removed from the basal by using plasma radiofrequency resection strategy. F, The tumor base was located in the nasal septum, and hemostasis was performed by plasma after resection. G, Endoscopic examination of the left nasal cavity at 4 weeks after the operation.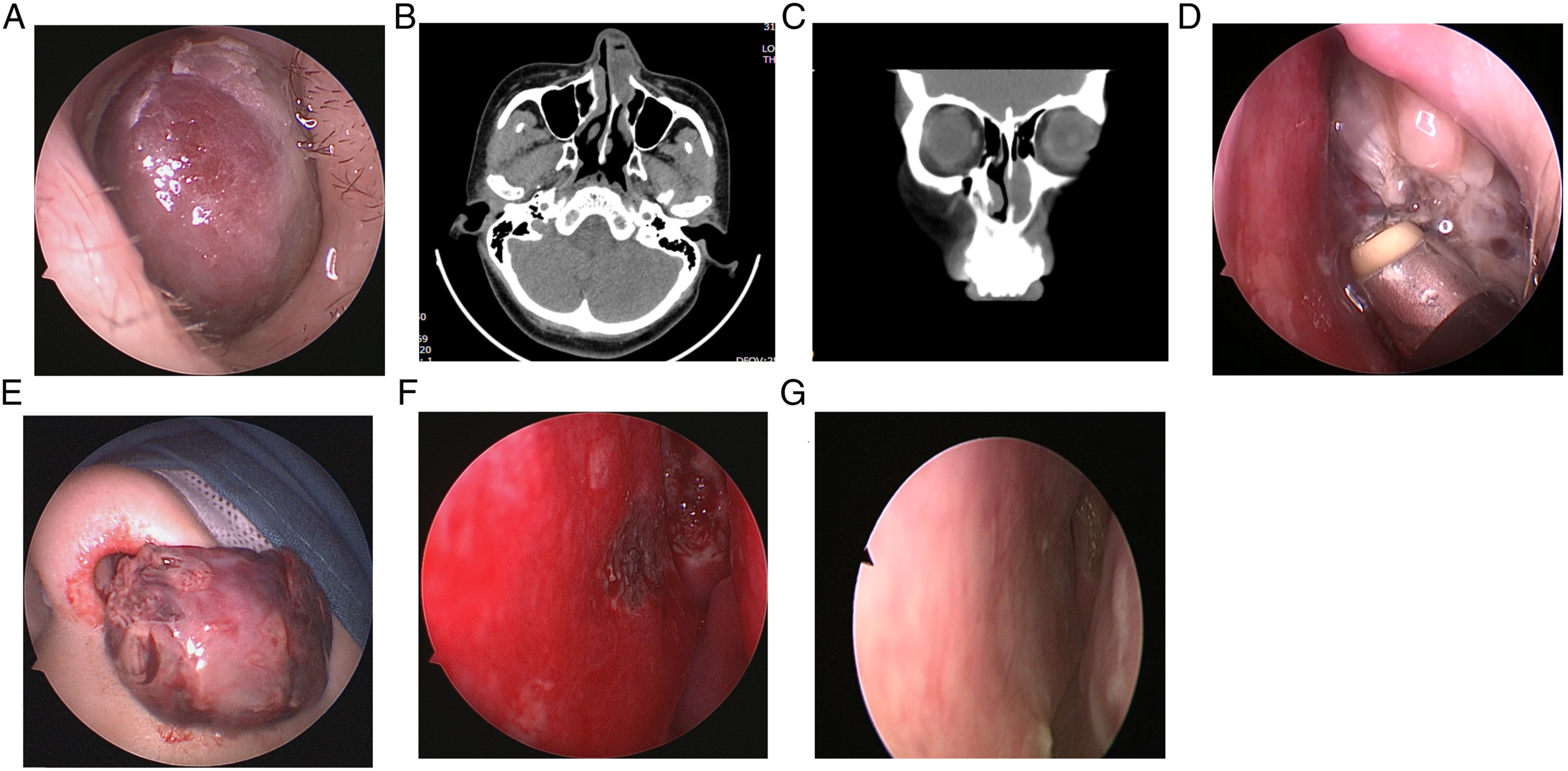
Case 2
A 43-year-old man was admitted to the hospital for the pharyngeal paraesthesia in February 2017. The electronic laryngoscope showed a light red projection (about 1.5 × 1.2 × 1.0 cm) on the left posterior pharyngeal wall and 3 cysts on the tongue side of the epiglottis (Figure 2A and B). During the operation, the tumor was exposed by a Davis mouth-gag. The plasma wand was placed close to the tumor body for ablation, gradually from the outer part toward the center part of the tumor (Figure 2C), then the tumor turned pale, and the protruding tumor body became atrophic and finally flat (Figure 2D). Subsequently, the epiglottic cysts were removed with plasma radiofrequency under a suspension laryngoscope. Six months later, there were few signs of surgery on the left posterior pharyngeal wall and the epiglottis (Figure 2E and F). The clinical data of case 2. A and B, The electronic laryngoscope showed a light red projection on the left posterior pharyngeal wall, A, and 3 cysts on the tongue side of the epiglottis, B. C, The tumor was ablated by plasma from the outer part towards the center part. D, The tumor became atrophic and finally flat by the direct ablation. E and F, The electronic laryngoscope showed the left posterior pharyngeal wall E, and the epiglottis F, at 6 months after the operation.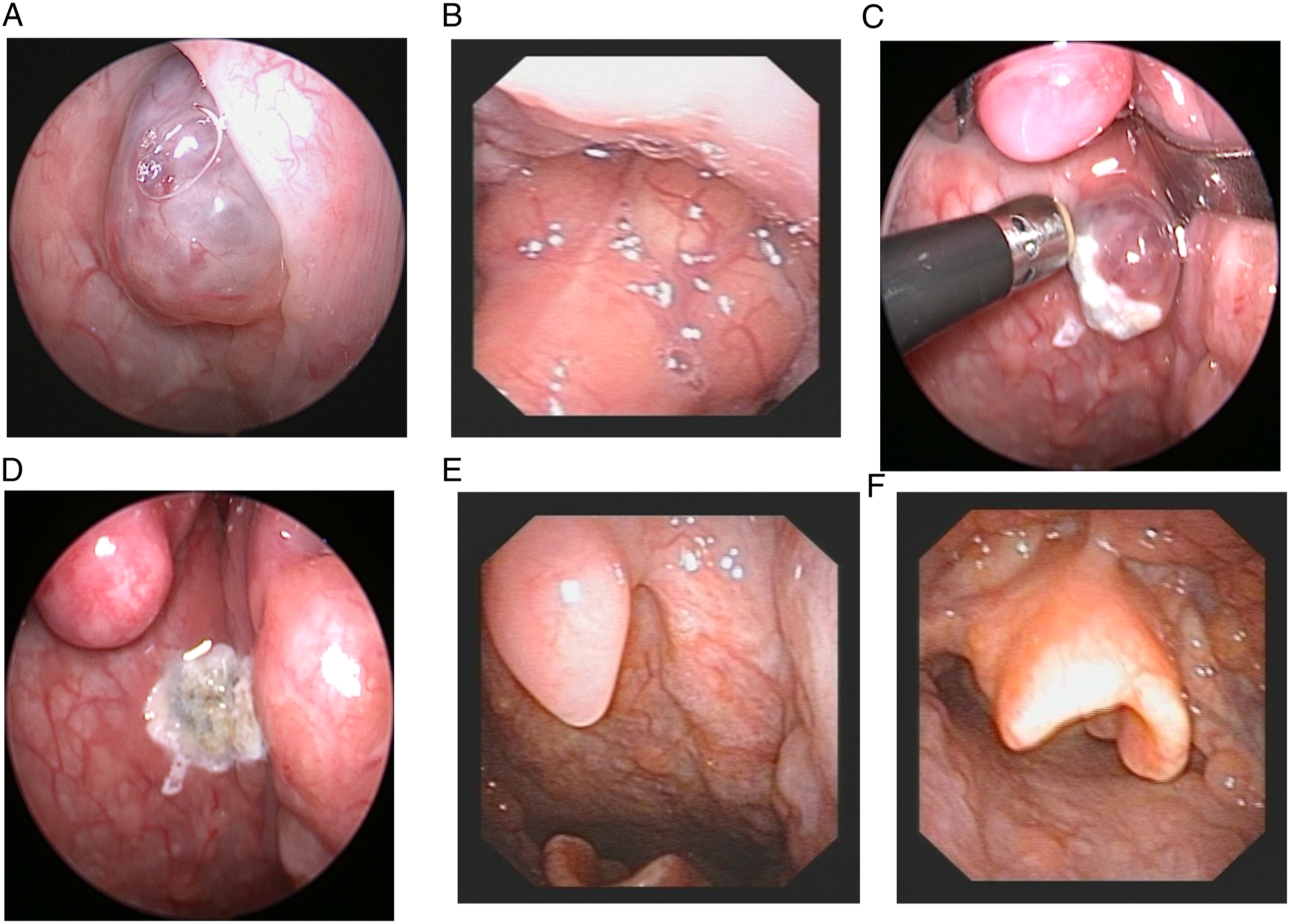
Case 3 A 63-year-old woman was admitted to the hospital for the pharyngeal paraesthesia in March 2017. The electronic laryngoscope showed a dark red, smooth neoplasm on the laryngeal side of the epiglottis, and the left ventricular band and interior wall of the left sinus piriformis (Figure 3A and B). A laryngopharyngeal magnetic resonance (MR) examination suggested a neoplasm on the left supraglottic region and the sinus piriformis (Figure 3C and D). The neoplasm was clinically diagnosed as a hemangioma, and the surgical strategy of direct ablation was adopted. Under a suspension laryngoscope, the plasma wand was placed close to the tumor body for ablation, then the tumor turned pale, and the protruding tumor body became atrophic and finally flat. One week after the operation, a white membrane was present on the wound (Figure 3E). One month later, a hyperplastic granulation tissue was found on the left ventricular band (Figure 3F), but there was no hemangioma. Inhalation of aerosol Pulmicort 1 mg plus saline 5 ml was continued for 10 days. Two months after the operation, the granulation tissue was disappeared, and the mucosa was smooth (Figure 3G).
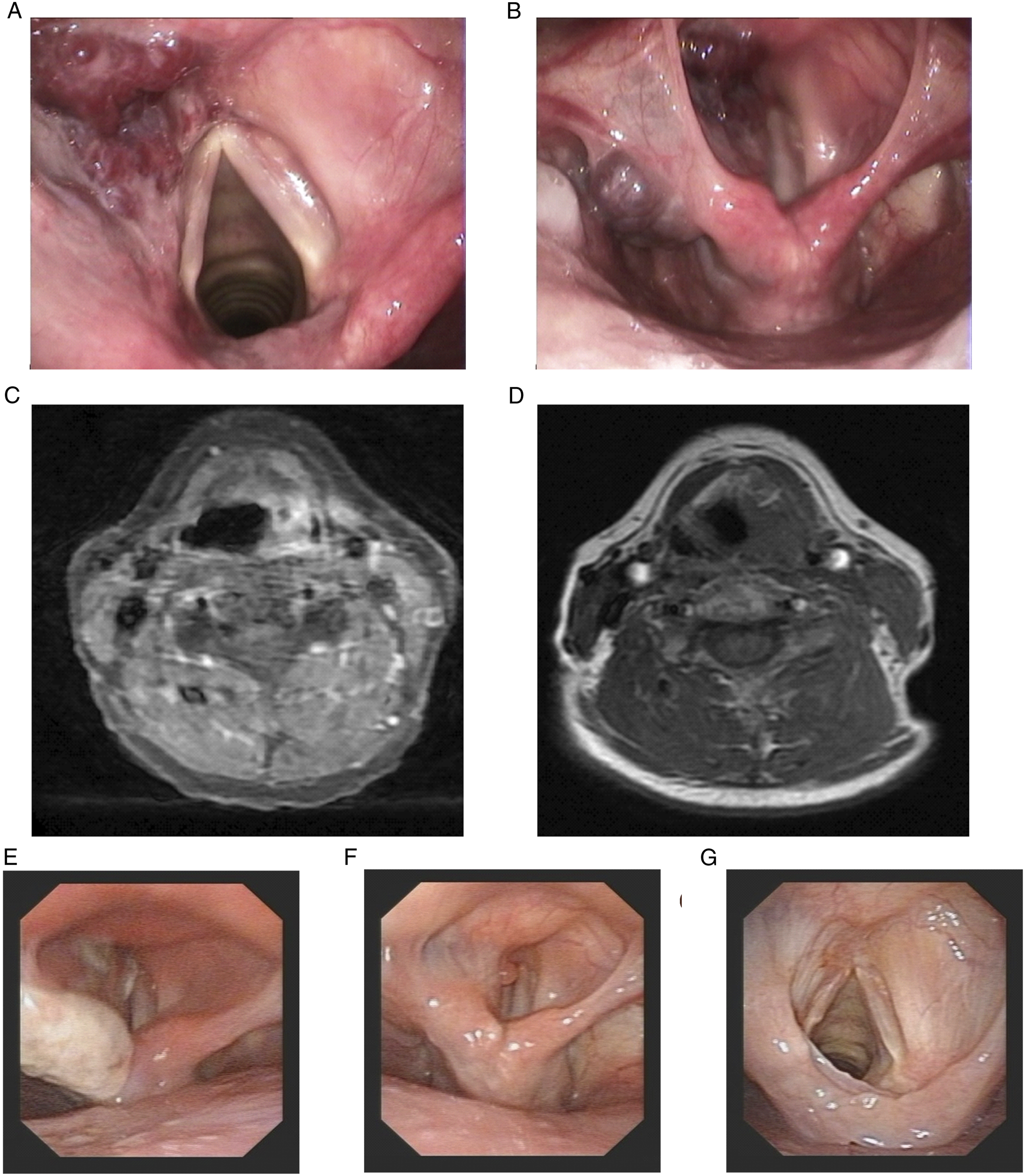
The clinical data of case 3. A and B, The electronic laryngoscope showed the neoplasm on the laryngeal side of the epiglottis, A, and the left ventricular band and interior wall of the left sinus piriformis, B. C and D, A laryngopharyngeal MR examination revealed a neoplasm on the left supraglottic region, C, and the sinus piriformis, D. E, The neoplasm was directly ablated and then became atrophic and finally flat. F, A hyperplastic granulation tissue was found on the left ventricular band at 1 month after the surgery. G, The granulation tissue was disappeared and the mucosa was smooth at 2 months after the surgery.
Discussion
Hemangioma is a type of common vascular disease in the head and neck, but it is uncommon in the nasal cavity and paranasal sinus. It was reported in a large sample study of 1479 patients with hemangiomas: nasal cavity or paranasal sinus hemangiomas accounted for 12.3% of head and neck cases and only 2.5% of total cases. 5 The incidence of a hemangioma during pregnancy was 2%-5%; it is generally believed that increased estrogen and progestin during pregnancy can stimulate the proliferation of endothelial cells in the mucosa. 6
Hemangiomas are pathologically categorized into capillary hemangiomas and cavernous hemangiomas. The former is composed of capillary-sized vessels lined with squamous endothelium and separated by a collagen matrix; the body of the tumor is generally small with a pedicle, red or dark-red colored, soft, and easy to bleed, while the latter is composed of large blood vessels; the tumor body is big and soft with a wide base and is easily compressible. Usually, no complete envelope can be found under a light microscope.7,8 Clinically, capillary hemangioma is the most common type of nasal hemangioma, which usually occurs on the nasal septum, while cavernous hemangiomas are located more commonly on the lateral wall of the nasal cavity, pharynx, and larynx. 8 The diagnosis of a hemangioma usually depends on pathological examination. However, preoperative biopsy is not recommended for this kind of hemorrhagic disease, and a clinical diagnosis is usually established by endoscopy and imaging examinations. It has been reported that CT and MR imaging, especially contrast-enhanced scan, can identify these 2 types of hemangiomas.7,9 During the operation, we first touched the hemangioma with the plasma wand, and a cavernous hemangioma was more easily compressed and significantly reduced after ablation, while capillary hemangioma was opposite; then, we continued to remove different types of hemangiomas using corresponding methods. In this study, 29 cases of hemangioma were reported, of which 16 cases of nasal capillary hemangiomas were confirmed by postoperative pathological examination, consistent with our intraoperative assessment, and 13 cases of cavernous hemangiomas were clinically diagnosed based on endoscopy and MR examination. It should be noted that all 13 cases of cavernous hemangiomas were clinically diagnosed and not pathologically confirmed, they should be closely followed up to prevent the possibility of other tumors.
In recent years, the application of low-temperature plasma radiofrequency in the treatment of hemangioma of head and neck has achieved good results, and the combination of low-temperature plasma radiofrequency technology and endoscopic technology is a key technique for minimally invasive and accurate treatment of hemangiomas of the nasal cavity, pharynx, and larynx. With the recent rapid development of low-temperature plasma radiofrequency, the aim of hemostasis can be achieved by blocking the blood vessels while abating the hemangioma, which is very suitable for the treatment of hemorrhagic diseases and even for the resection of vascular tumors.10–15 Compared to laser and electrocoagulation, plasma radiofrequency works at relatively low temperatures and causes less damage to surrounding tissues; furthermore, there are fewer postoperative scabs and scars. Several studies have reported the use of low-temperature plasma radiofrequency in the treatment of hereditary hemorrhagic telangiectasia with epistaxis and in the removal of nasopharyngeal fibroangiomas with or without embolization before surgery; these cases have achieved good results, with the advantages of less trauma, less bleeding, and quick recovery.11–14 In general, plasma radiofrequency can not only reduce the size of tumors, but also have the functions of resection, hemostasis, irrigation, and suction when removing tumors rich in blood vessels, making it a truly practical and minimally invasive technology.14,15
Although more and more hemangiomas in the head and neck are treated with low-temperature plasma radiofrequency, there have been no reports on the strategies for different types of hemangiomas. It was reported in a study that the application of low-temperature plasma radiofrequency in the treatment of nasal hemangioma had the advantages of small trauma, quick recovery, and no recurrence, but the blood loss was 1-150 ml, with an average blood loss of 15 ml. l4 Another study reported the use of low-temperature plasma radiofrequency to treat laryngopharynx hemangioma, and they analyzed 24 cases and followed up from 6 to 24 months; the results showed that all patients achieved good results, but there was 1 case of recurrence and 1 case of postoperative incomplete vocal cord paralysis because of wide range angeioma, and they concluded that coblation treatment for laryngopharynx hemangioma was an ideal way for less bleeding, less damage, and clearer field of vision. 3 A recent article reported the use of low-temperature plasma radiofrequency in the treatment of tongue hemangioma, and they concluded that this method might have advantages of simple operation, wide vision, fewer postoperative complications, and quick recovery. 16 However, none of these reports presented a detailed protocol for plasma use, nor did they consider the type of hemangioma. In our study, according to the principles of plasma ablation and the pathological features of hemangiomas, 2 different surgical strategies were performed for the treatment of capillary and cavernous hemangiomas. As the capillary hemangioma consists of blood vessels of capillary size, the strategy of ablation before resection was adopted. The plasma wand was placed close to the tumor body for ablation, and then the tumor body changed from dark red to pale and shrank. Gradually, the base of the tumor was exposed, and then the tumor body as well as the mucosa of the tumor base was resected together. The hemostasis on the tumor base was also performed with the plasma wand (typical case 1). For the cavernous hemangioma, since it is composed of large blood vessels, direct ablation was adopted for the surgery, which was different from the method of plasma resection for hemangiomas reported in the literature.3,4 The plasma wand was placed close to the tumor body for gradual ablation from the surrounding part toward the center part of the tumor. During the process of ablation, the tumor body became pale and atrophied gradually. Finally, the protruding part became flat (typical cases 2 and 3). All the 29 patients in this series underwent one-off operations and also achieved good results, with the same advantages of less trauma, quick recovery, no recurrence, no complications, and less bleeding. A total of sixteen patients with nasal capillary hemangiomas were roughly estimated to have 2-5ml of bleeding when the tumor base was removed, while the rest of the 13 patients with cavernous hemangiomas had nearly a bloodless field.
Conclusion
In conclusion, we have reported that low-temperature plasma radiofrequency is a practical, minimally invasive, and accurate method for treating hemangiomas in the nasal cavity, pharynx, and larynx. For capillary hemangiomas, the strategy of ablation before resection may be an obvious way to reduce bleeding. While for cavernous hemangiomas, the strategy of direct ablation is a simple and efficient method.
Footnotes
Author Contributions
All authors take responsibility for the integrity of this manuscript and give their final approval of the version to be published. HTZ had the original idea for the research, undertook collection of data, helped to interpret the data, performed the surgery, and revised the manuscript critically. XBL designed of the work, collected the data, helped to interpret the data, and drafted the manuscript. ZYL and YL helped to collect and interpret the data and revised the manuscript critically.
Conflict of Interest
The authors declare that they have no conflict of interest.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Natural Science Foundation of China (NSFC) grant 81400448 to Dr. Xiaobo Long, NSFC grant 81900913 to Dr. Zhiyong Li and Huazhong University of Science and Technology grant 2016082 to Dr. Hongtao Zhen.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. This study was approved by the Ethical Committee of the Tongji Medical College at Huazhong University of Science and Technology.