
Abstract
Significance Statement: We present the rare case of a nasal lobular capillary hemangioma with bony erosion atypically localized to the left piriform aperture. This fast-growing lesion caused both physical and emotional distress due to recurrent epistaxis and prominent esthetic deformity evidenced by a large nasal growth. While the final diagnosis was benign, the clinical and radiological findings caused concern. This case serves as a reminder that prompt referral, work-up, and diagnosis are essential to optimize patient care.
Significance Statement:
We present the rare case of a nasal lobular capillary hemangioma with bony erosion atypically localized to the left piriform aperture. This fast-growing lesion caused both physical and emotional distress due to recurrent epistaxis and prominent aesthetic deformity evidenced by a large nasal growth. While the final diagnosis was benign, the clinical and radiological findings caused concern. This case serves as a reminder that prompt referral, work-up, and diagnosis are essential to optimize patient care.
Case presentation
An 18-year-old female presented to the Otolaryngology clinic with a 2-month history of a rapidly expanding left-sided nasal mass extending beyond the nasal cavity. The mass caused unilateral nasal obstruction and recurrent ipsilateral epistaxis. The patient was not pregnant and had no past medical history. She denied facial or nasal trauma and previous epistaxis or nasal packing.
Upon examination, a large mass was protruding outwardly from the left nasal cavity completely obstructing the vestibule (Figure 1). There was no deformation of the external nasal or facial anatomy. No additional skin lesions were noted. The remainder of the head and neck examination, including contralateral nasolaryngoscopy, was unremarkable. Left nasal cavity mass in an 18-year-old female. (A) Pre-operative mass occupying the entire left nasal cavity and protruding externally. (B) Post-operative specimen excised from the left nasal cavity measuring approximately 3.5 cm in length.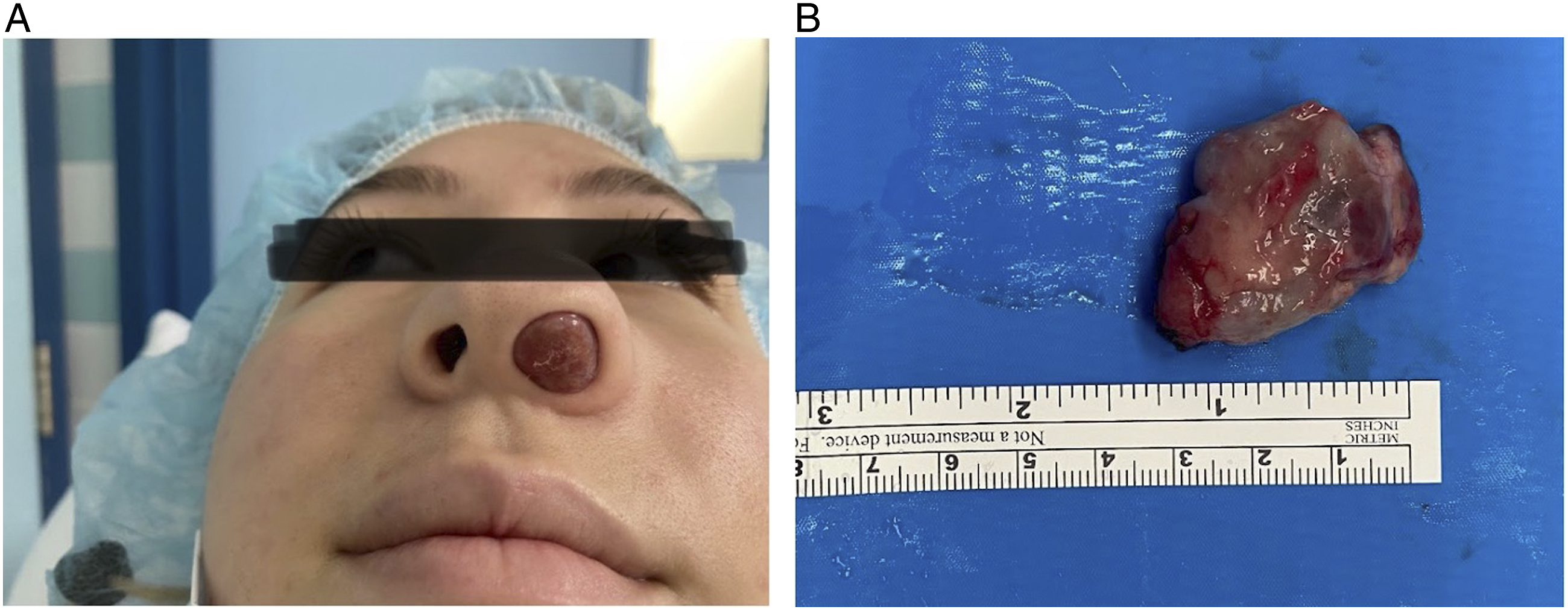
A computed tomography (CT) scan of the sinuses was performed (Figure 2), revealing a large mass measuring 34 x 21 x 30 mm located in the anterior nasal fossa and demonstrating bony erosion at the attachment to the piriform aperture, inseparable from the lesion. As a result, magnetic resonance imaging (MRI) was requested and demonstrated the enhancing well-circumscribed mass within the left nasal vestibule with several internal serpiginous vascular structures. The lesion was adjacent to the septum with no evidence of bony or septal invasion. CT sinus of left-sided LCH demonstrating a large mass (34 x 21 x 30 mm) in the anterior nasal fossa with bony erosion at the pyriform aperture. (A) Coronal plane. (B) Axial cut. Green arrows (A, B) demonstrating site of bony erosion.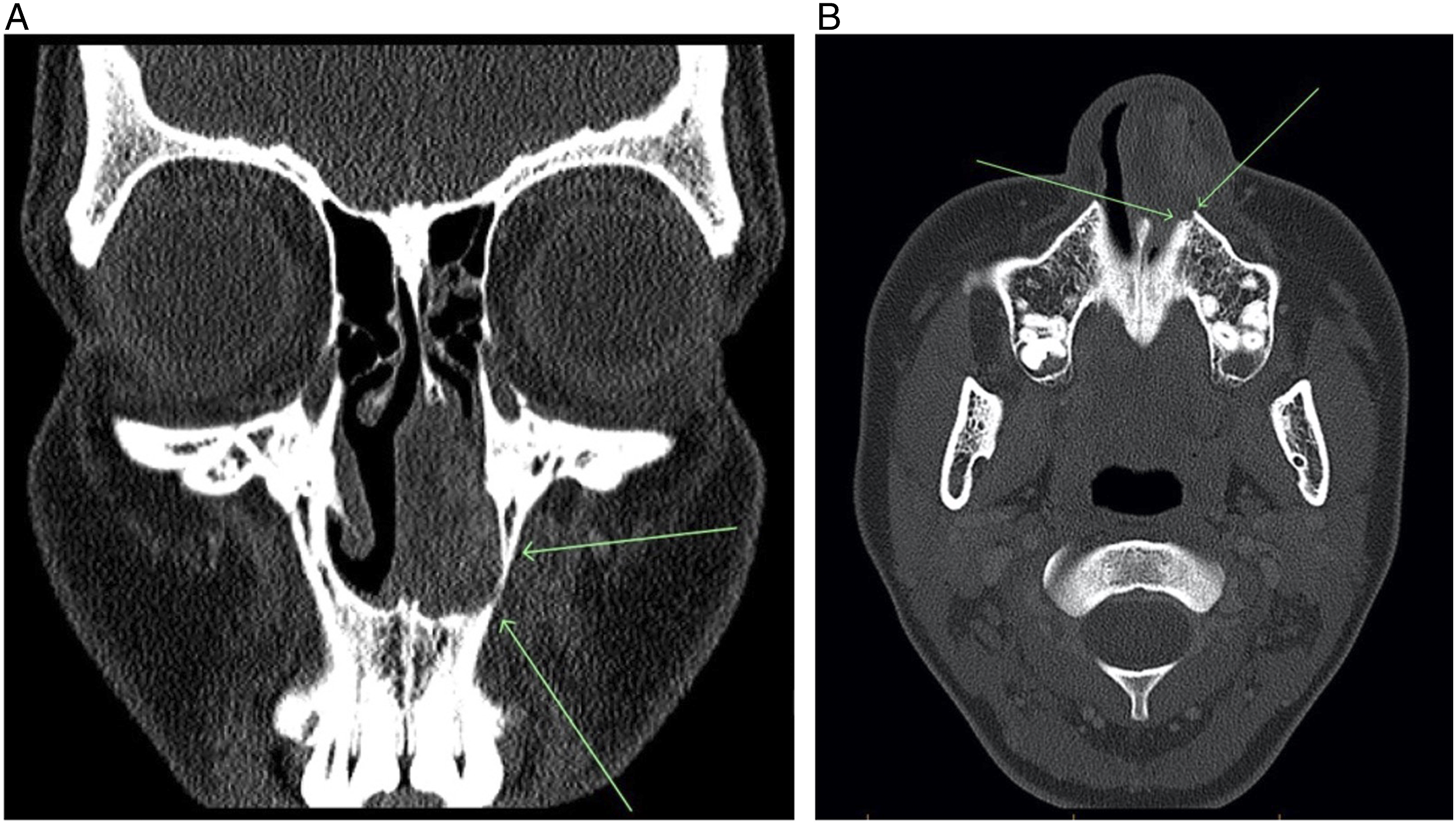
Moreover, the patient was brought to the operating room for an excisional biopsy. The examination revealed a pedunculated mass centered on the piriform aperture completely obstructing the left nasal cavity. The mass and an adjacent margin of soft tissue were excised by endoscopic endonasal intervention, and no perioperative complications ensued. On histological analysis, lobular arrangement of proliferated capillaries was noted, and lobular capillary hemangioma was diagnosed.
Discussion
Lobular capillary hemangiomas (LCHs), previously and inaccurately referred to as pyogenic granulomas (PGs), are benign hyperplastic vascular lesions commonly presenting on the skin or mucous membranes. 1 Etiology and pathogenesis of LCHs are not well understood but these lesions have neither infectious nor granulomatous causes.1,2 Pregnancy, trauma, immunosuppression, and certain medications including systemic retinoids have been associated with these growths.2,3,4,5
LCHs are characterized by their rapid growth pattern, often present as solitary nodules and are concerning for cosmetic reasons, risk of ulceration, and recurrent bleeding episodes attributed to the friable nature of the affected tissue. 6 As such, surgical excision is often performed to resolve bleeding. 7
In a large retrospective study of 408 adult and pediatric cases, LCH developed most frequently in the head and neck area followed by the trunk and upper extremities. 7 Cutaneous lesions are more prevalent than mucosal ones. 8 Of mucosal LCHs, the majority arise in the head and neck region predominantly in the oral cavity. 8 More uncommonly, the nasal cavity is involved, with the anterior nasal septum and tip of the turbinate as prevalent locations. 9 One of the largest retrospective studies exclusively examining nasal LCHs reported no lesions localized to the piriform aperture. 10 Nasal LCHs usually present clinically with recurrent unilateral epistaxis and nasal obstruction. 10
Bony erosion, as identified in this case, has been recognized in the literature yet remains a rare feature of nasal LCHs. 11 One report identified bony erosion in five of seventeen (29.4%) cases of nasal hemangiomas, while another found that bony erosion was present in three of six (50%) patients diagnosed with nasal cavity LCHs.12,13 The erosion was identified at the inferior turbinate, middle turbinate, nasal septum, and the medial wall of the maxillary sinus, none involving the pyriform aperture. Despite these two papers, the current understanding within the Otolaryngology community is that nasal LCHs are soft-tissue masses without bony destruction or invasion. Therefore, this review serves as a reminder to keep LCH in the differential diagnosis when bony erosion is identified.
To our knowledge, this is the first case report of an LCH originating from the nasal pyriform aperture. While the final histopathological report confirmed the presence of a benign mass, prompt management of such lesions is paramount as they can cause severe distress. Additionally, certain features such as fast growth rate and bony erosion can be worrisome mimickers of malignancy further emphasizing the urgency required to manage these lesions.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.