
Abstract
Hamartomas result from the growth of normal tissues which are endogenous to the site of the lesion. Typically, hamartoma tissues appear spatially disorganized and merge with normal surrounding tissues. 1 In the oral cavity, the involved tissues include smooth and skeletal muscle, fat, salivary tissues, as well as nerves and blood and lymphatic vessels.1-3 Hamartomas composed of closely packed and variably sized intertwined nerve bundles and blood vessels, ie, neurovascular hamartomas (NVH), are extremely rare in the oral cavity; it has been hypothesized that this may be due to unrecognition and under-reporting. 1
Herein we present the case of a 28-year-old Caucasian woman presenting to our University hospital in June 2021 with a 6-month history of multiple millimetric excrescences involving the ventral surface of the tongue and the adjacent mucosa of the floor of mouth, associated with burning sensation. She was otherwise healthy and denied trauma, history of tumors or previous local surgery. The overlying surface of the lesions was smooth; no cervical lymphadenopathies were clinically evident. The lesions were clinically interpreted as squamous cell papilloma and were subsequently excised under local anesthesia. No preoperative pictures of the lesions were taken.
At histology, the lesions showed a polypoid architecture. The lining squamous epithelium was unremarkable. The stromal axis was loose, virtually devoid of inflammatory cells and enriched in small nerve bundles that appeared in close proximity to small-size blood vessels (Figure 1 A-D Whole-mount histological view of the excised lesions are illustrated in panels A-C. The lesions share small nerve bundles (aterisks) closely associated with the wall of a small-size blood vessels (arrows) as detailed in panel D (boxed area of the lesion illustrated in (A). The vascular and neural components of the lesion are highlighted by the immunohistochemical stains for CD34 (marker of endothelial cells, (E), S100 (marker of Schwann cells, (F) and neurofilaments (major cytoskeletal element in nerve axons, (G). The intra-epithelial immunoreactivity for S100 highlights normal dendritic/Langerhans cells. (A-D): hematoxylin-eosin. Bars: 500 μm in A-C, 200 μm in D, 150 μm in E and 100 μm in F and G.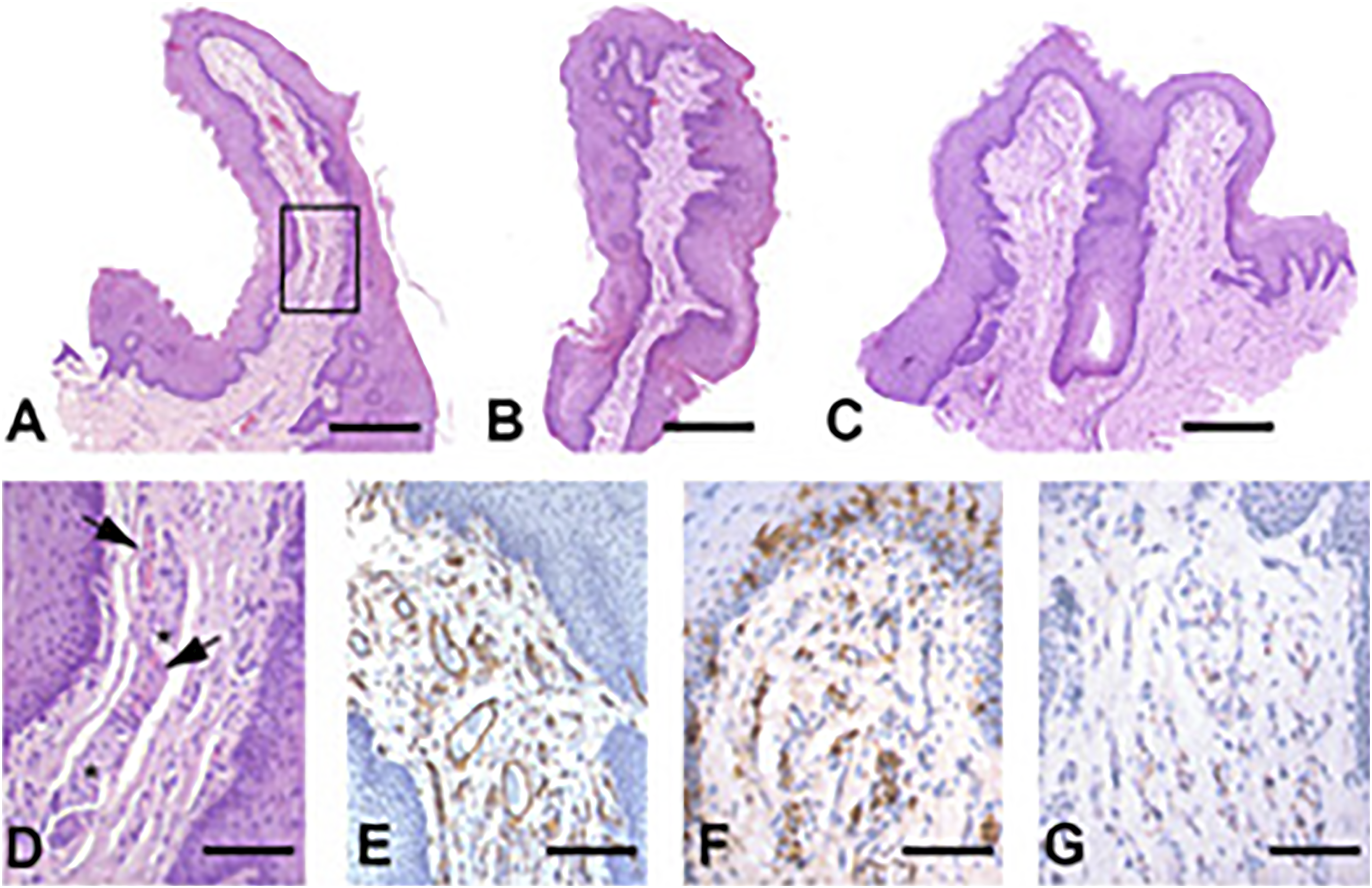
Even though some types of hamartomas have been reported in the context of syndromic conditions as PTEN hamartoma tumour, Cronkhite-Canada’s and Oro-facial digital syndromes and Sclerosis Tuberosa,1,10 oral NVHs have been always reported as sporadic entity,1-3 as in our case. However, compared to the previously reported cases,1-3 oral NVHs have been always reported as solitary “exophytic masses” 1 or “ulcerated lesion”. 2 In contrast, in our case the lesions were multiple and appeared as small millimetric excrescences over the mucosal surface.
Given the well-established non-specific clinical presentation of NVHs,1,2 histologic examination of the lesions is ultimately required to establish the diagnosis. Allon et al 1 were the first authors to describe the fine histological features of oral NVHs. In our case, the possibility of multiple traumatic neuromas was also considered, but was excluded for the absence of history of local trauma and surgery and, at histological level, for the close association of nerve and vessels and for the absence of inflammation and fibrosis. 1 A further potential entity for differential diagnosis could be benign mesenchymoma, a non-encapsulated lesion composed of at least two benign mesenchymal tissues, excluding the fibroblastic component and without predominance of a tissue type. 3 Unquestionably, as noted by Kreiger et al, 3 “benign mesenchymoma would fulfill the criteria for hamartoma as well”. However, we share the opinion of other authors according to which the distinction between benign mesenchymoma and NVH may represent “differences in terminology” 1 or “a nomenclative quandary”. 2
In conclusion we reported the clinical and pathologic findings of unusual multiple benign oral lesions that were clinically interpreted as squamous cell papilloma but were histologically consistent with NVH. Neurovascular hamartomas is rare in the oral cavity and, as far as we know, multiple NVHs have never been reported at this site.
Footnotes
Authors’ note
The data sets used and/or analyzed during the current study are available from the corresponding author on reasonable request, except for preoperative clinical picture that were not taken. All the clinic-pathologic investigations detailed in the manuscript have been conducted in accordance with the Declaration of Helsinki and its later amendments or comparable ethical standards. Written informed consent for publication of data and images was obtained from the patient.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.