
Abstract
Keywords
Introduction
Petrous temporal bone cholesteatoma (PBC) is a rare disease developing in the petrous portion of the temporal bone with an incidence ranging from 4 to 9% of all petrous pyramid lesions. 1 Since it has a slow and silent growth, it may produce severe functional damage, reducing patients’ quality of life.
Radical surgery of PBCs is performed by means of different techniques based on the location and extension of the lesion, respecting the facial nerve and inner ear. 2 The main complications of PBC surgery are facial nerve palsy and severe hearing loss, depending on their proximity to the disease. 3 Since PBC involves the otic capsule, it comes into contact with the membranous labyrinth structures: cochlea (anterior labyrinth) and the vestibular system (posterior labyrinth). 4
Over the last years, advances in neuroradiology and modern surgical techniques have made it possible to remove PBCs more safely, with minimal recurrence, and perioperative morbidity.
Sanna et al classified PBCs into 5 subtypes (supralabyrinthine, infralabyrinthine, infralabyrinthine-apical, apical, and massive) depending on their localization and defined possible surgical approaches. 5
According to many authors, otic capsule and hearing preservation are impossible to achieve in most supralabyrinthine or infralabyrinthine PBCs, due to the high risk of recurrence.6,7
In cases of supralabyrinthine PBCs, 5 the middle cranial fossa approach is preferred to the transotic one in order to maintain the otic capsule and the preoperative level of serviceable hearing, even though this implies a higher incidence of recurrence.
Infralabyrinthine PBCs are usually treated by translabyrinthine and transotic approaches with resulting anacusia. Hence, Fish proposed the infratemporal fossa approach as a hearing preservation technique. 8
In the recent literature, few studies have reported good hearing preservation outcomes after PBC surgery.9–13 On the contrary, good hearing outcomes have been reported after vestibular Schwannoma surgery performed using modified translabyrinthine techniques.14,15
Adoption of intraoperative endoscopic procedures is generally accepted, but their use in PBC surgery is mentioned in only a few papers.
The aims of this study were to evaluate the efficacy of modified translabyrinthine techniques in preserving hearing function and the use of adjuvant endoscopic techniques in a group of patients affected by PBCs. The outcomes and the possible disadvantages of these methods are discussed.
Patients and methods
This retrospective study described a series of 16 patients with petrous bone cholesteatoma who were referred to our Department for surgery between 2008 and 2020. This research was performed in accordance with the principle of the Declaration of Helsinki and approved by the local Ethics Committee of the University “Sapienza,” Rome.
Patients’ characteristics
The database was analyzed for presenting signs and symptoms, surgical details, and post-operative complications. A cohort of 23 consecutive patients, surgically treated for PBCs, was reported in the database. The inclusion criterion was related to hearing status that was assessed with pure tone audiometry (PTA) and speech discrimination. The degrees of hearing preservation and loss were defined according to the Gardner–Robertson classification system. 16 Sixteen patients belonging to Class I–III of this classification (serviceable in class I and II and with a potential improvement with hearing aid in class III) were enrolled.
Facial function was based on the House Brackman (HB) classification. 17
Preoperative Computed Tomography (CT) showed the extension of the disease. Topographically, the lesions were grouped using Sanna’s classification.2,5
When a PBC was observed, a temporal bone magnetic resonance was performed to differentiate it from other lesions such as cholesterol granuloma, mucocele and temporal bone tumors.
Surgical management
The choice of surgical technique was based on the database and the preoperative conditions of each patient; all definitive surgical procedures were performed by the senior author (GM).
Comparison between hearing preservation techniques for PBCs.
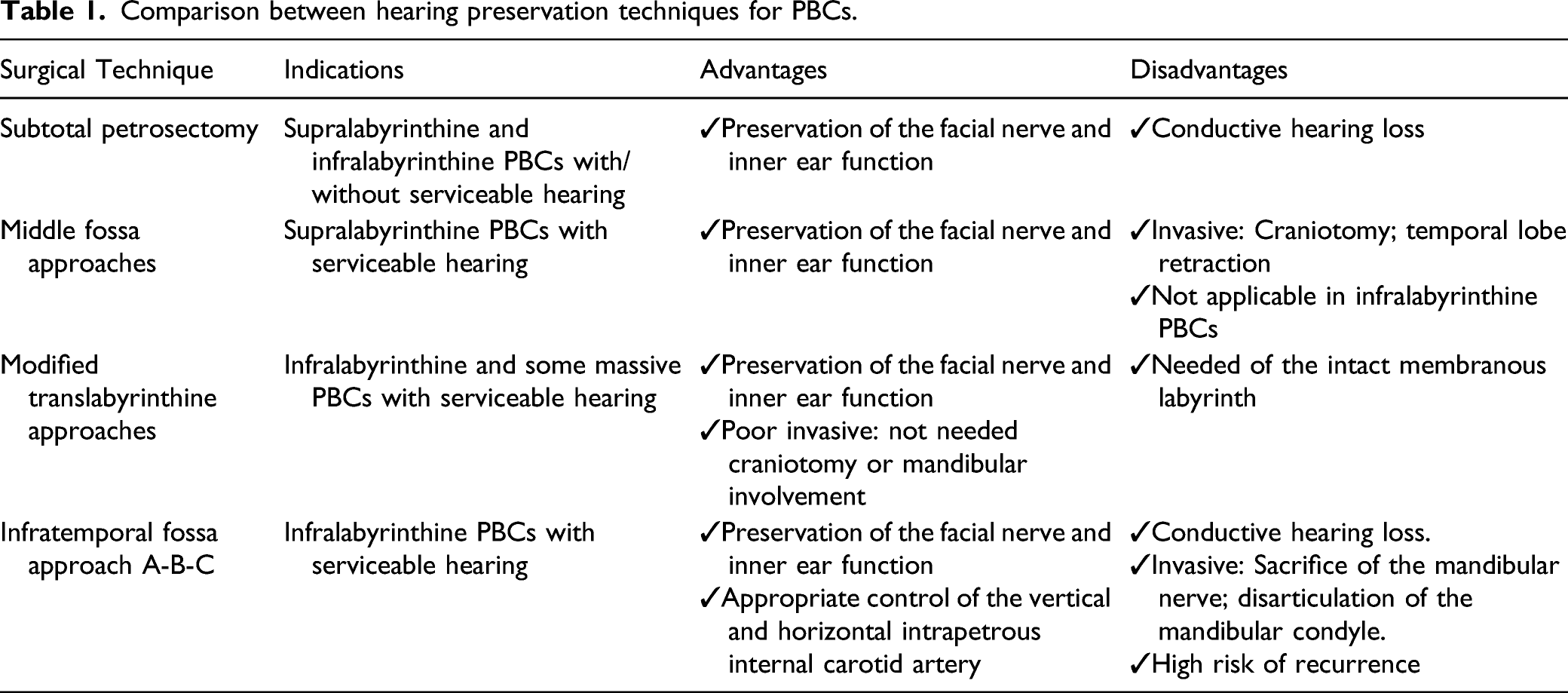
In cases of infralabyrinthine cholesteatoma with serviceable hearing, a modified translabyrinthine approach was chosen, while in other cases subtotal petrosectomy with blind closure of EAC was performed (Table 1).
Modified trabnslabyrinthine approach
The modified translabyrinthine technique consisted of a cutaneous incision similar to that used in the traditional one. 15 After drawing the periosteal flap back and exposing the cortical mastoid, total mastoidectomy was performed. All of the mastoid cells were removed, exposing the medial cranial fossa tegmen, the sinodural angle, and the dura of the posterior cranial fossa at the front and back of the sigmoid sinus, which was skeletonized with exposure of the jugular bulb. The three semicircular canals were identified from the horizontal canal as the starting point. The bone covering of the semicircular canal is removed using a diamond burr. This passage is performed keeping the dissection area as wet as possible and avoiding suction of the fluid around the labyrinth, which may violate the membranous labyrinth. When the posterior bony labyrinth has been completely removed, the area of the posterior, horizontal, and upper semicircular canals is occluded with bone wax.
Particular care must be taken to close off completely the access to the vestibule of the semicircular canals. Maintaining the vestibule anatomically intact and isolating it completely is fundamental for successful preservation of hearing function. If the cholesteatoma reaches the internal auditory channel, the bone around the vestibule must be scrupulously removed until the “blue line” of the internal auditory canal can be identified. The bone between the jugular bulb and the resected semicircular canals must be removed.
In the event of a semicircular canal fistula being identified, the cholesteatoma matrix was isolated and gently raised, exposing the membranous labyrinth. Firstly, the membranous labyrinth with the matrix was excised using a sickle knife and then the opening in the labyrinth was rapidly closed with bone wax. For the time it remained open, the membranous labyrinth was kept wet with Ringer’s solution and no suction was applied close to the openings of the semicircular canals to protect the anatomy and function of the membranous labyrinth of the vestibule. Using a cottonoid, the closure of the fistula was then reinforced with bone paste and temporalis fascia. This allowed preservation of the vestibule, sealing the openings of the semicircular canals. 18
Subtotal petrosectomy
Subtotal petrosectomy is defined as a complete exenteration of all pneumatic cell tracts of the temporal bone with closure of the isthmus of the Eustachian tube. The first step is retroarticular temporal incision followed by a blind sac closure of the EAC. The skin of the auditory canal is totally removed from the lateral bony canal. Mastoidectomy is performed exposing the medial cranial fossa tegmen, the sinodural angle and the dura of the posterior cranial fossa at the front and back of the sigmoid sinus, which was skeletonized with exposure of the jugular bulb. The facial nerve is identified and preserved, removing the posterior canal wall and following the passage of the Fallopian canal from the oval window to the stylomastoid foramen.
Then temporal pneumatic cells are removed (retrosigmoid, retrofacial retrolabyrinthine, supralabyrinthine, infralabyrinthine, pericarotid, and supratubal). Finally, the middle ear is obliterated with abdominal flat and fibrin glue.
Endoscopic adjuvant approach
For endoscopic adjuvant surgery, a rigid endoscope with an angulation of 45°, a length of 14-cm, and an outer diameter of 3 mm and 4 mm (Storz, Germany) was used. It was connected to a camera head (Storz, Germany) and a high-definition monitor positioned in front of the surgeon. It allows better visualization and removal of the matrix of the cholesteatoma from the dura of the middle and posterior cranial fossa and near the posterior labyrinth.
Follow-up
Post-operative follow-up ranged from 1 to 10 years (average of 3.9 years) and included CT and Magnetic Resonance Imaging (MRI) to estimate cholesteatoma recurrence. The Gardner–Robertson classification system and facial nerve function were evaluated at 3-6-12 months; after the first year of follow-up, they were repeated once a year.
Results
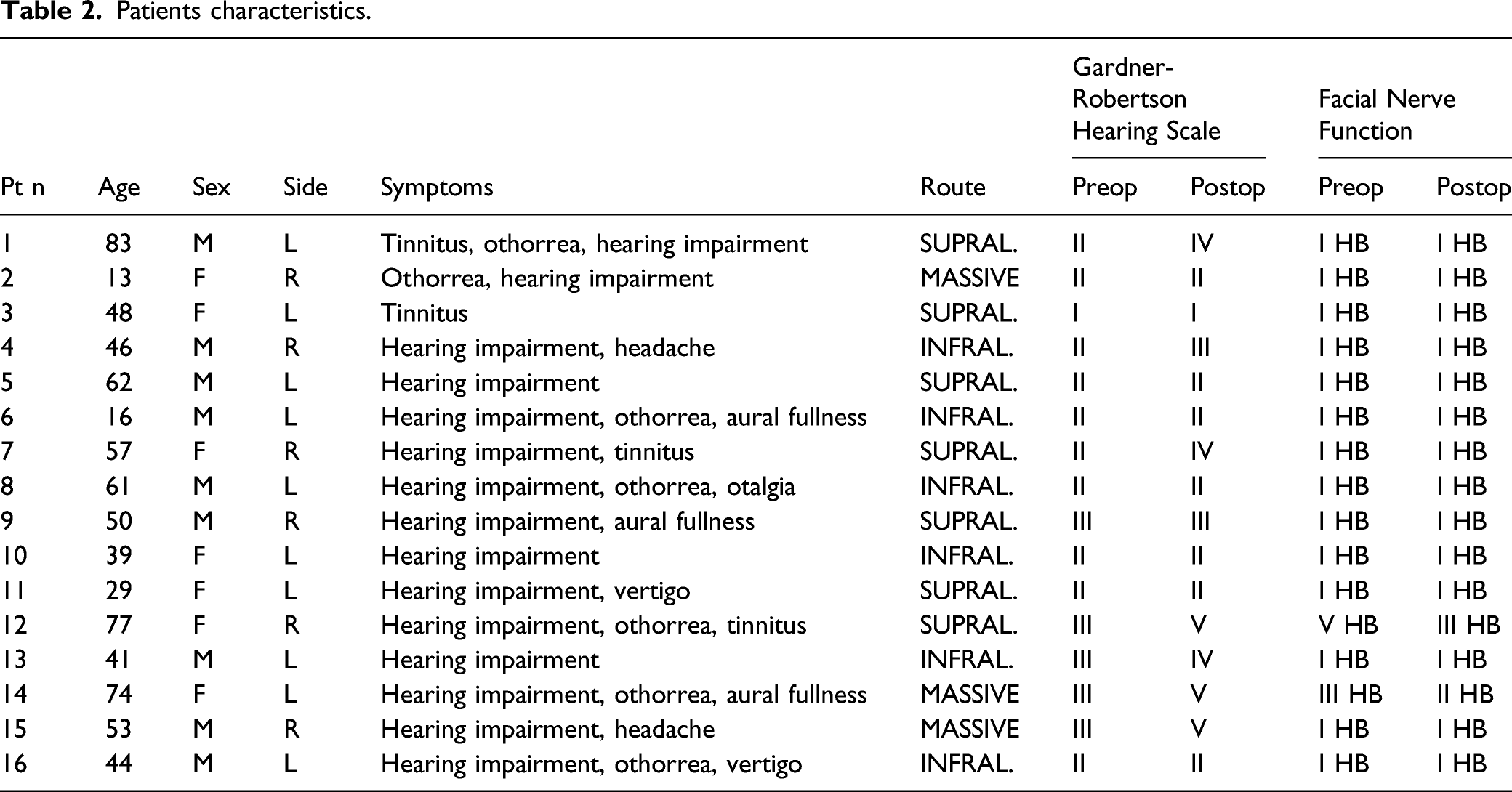
Patients characteristics.
All the cholesteatomas were acquired: 11 patients underwent primary surgery, while 5 had previously undergone otologic surgery in other structures.
Otomicroscopic exams revealed 5 epitympanic perforations, 4 subtotal or total perforations; 3 normal tympanic membranes associated with swelling in their inferior portion; 2 canal wall up tympanoplasty, 1 canal wall down tympanoplasty, and 1 radical tympanoplasty.
Hearing impairment was the most common symptom, present in 94% of patients (15/16) (Table 2). Preoperative Gardner–Robertson hearing evaluation evidenced 6.3% Class I (1/16); 62.5% Class II (10/16); and 31.25% Class III (5/16) (Table 2).
Facial palsy was present in 12.5% (2/16): one patient had a grade III HB for 4 months and the other had grade V HB for 7 months (Table 2).
PBCs were categorized according to Sanna’s classification: 6/16 (37.5%) were infralabyrinthine cholesteatomas; 7/16 (43.75%) were supralabyrinthine cholesteatomas, and 3/16 (18.75%) massive ones (Figure 1). (a) CT scan examination of massive petrous bone cholesteatoma in contiguity with the jugular bulb and involving the dura mater; and (b) CT scan examination of massive petrous bone cholesteatoma in contiguity with the jugular bulb and the dura mater.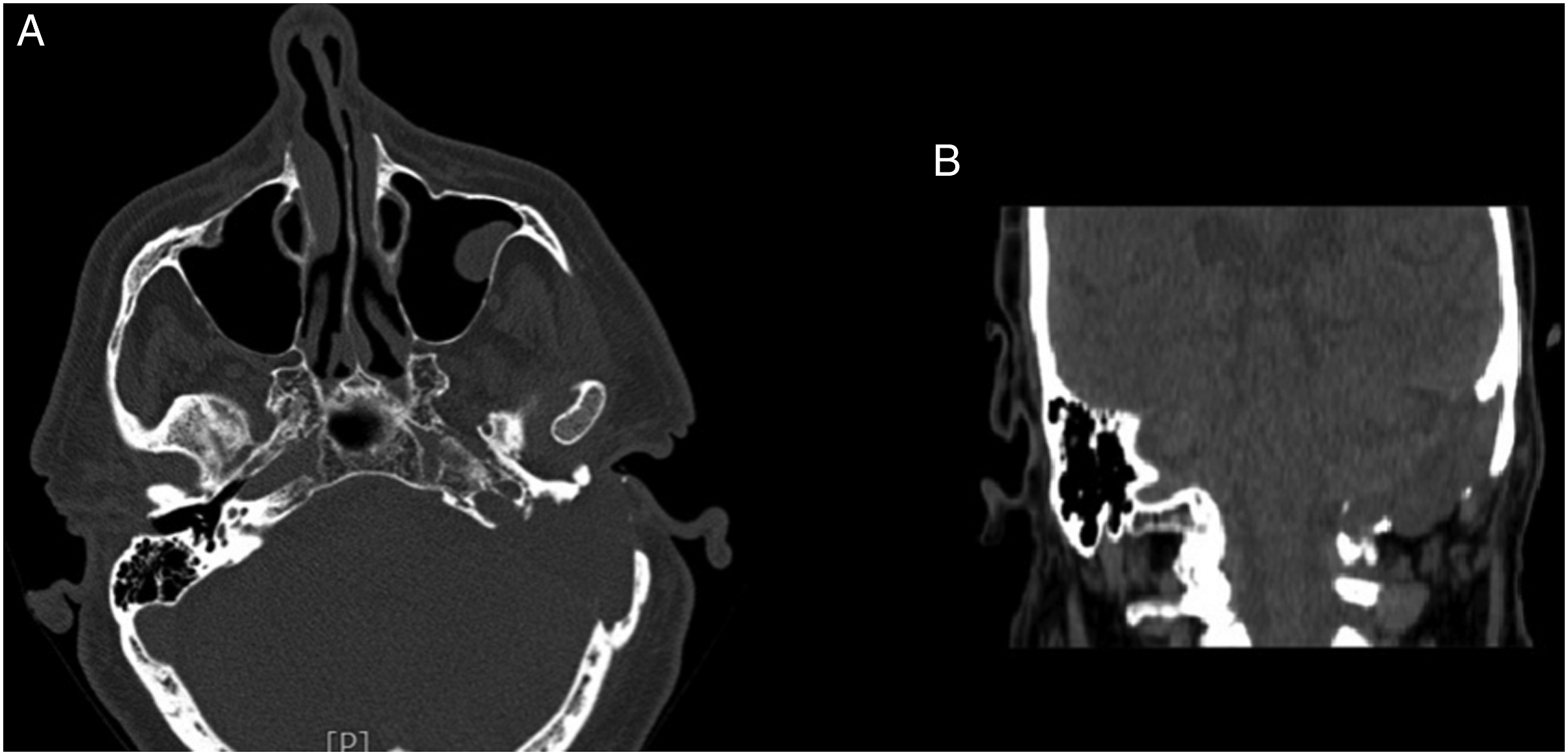
Preservation of the bone conduction threshold was possible in 62.5% of patients (10/16) (Table 2).
In our series of supralabyrinthine PBCs subtotal petrosetomy was performed in all cases and hearing preservation was possible in 4 patients (57%) (Table 2). The endoscopic adjuvant approach was performed in 3 cases (43%).
Infralabyrinthine PBCs are usually removed by subtotal petrosectomy with labyrinthectomy or translabyrinthine or transotic approaches, sacrificing hearing. In our series of patients, they were surgically treated with the modified translabyrinthine approach and showed preservation of bone conduction in 83% of patients (5/6). The adjuvant endoscopic adjuvant approach was adopted in 3 cases (50%).
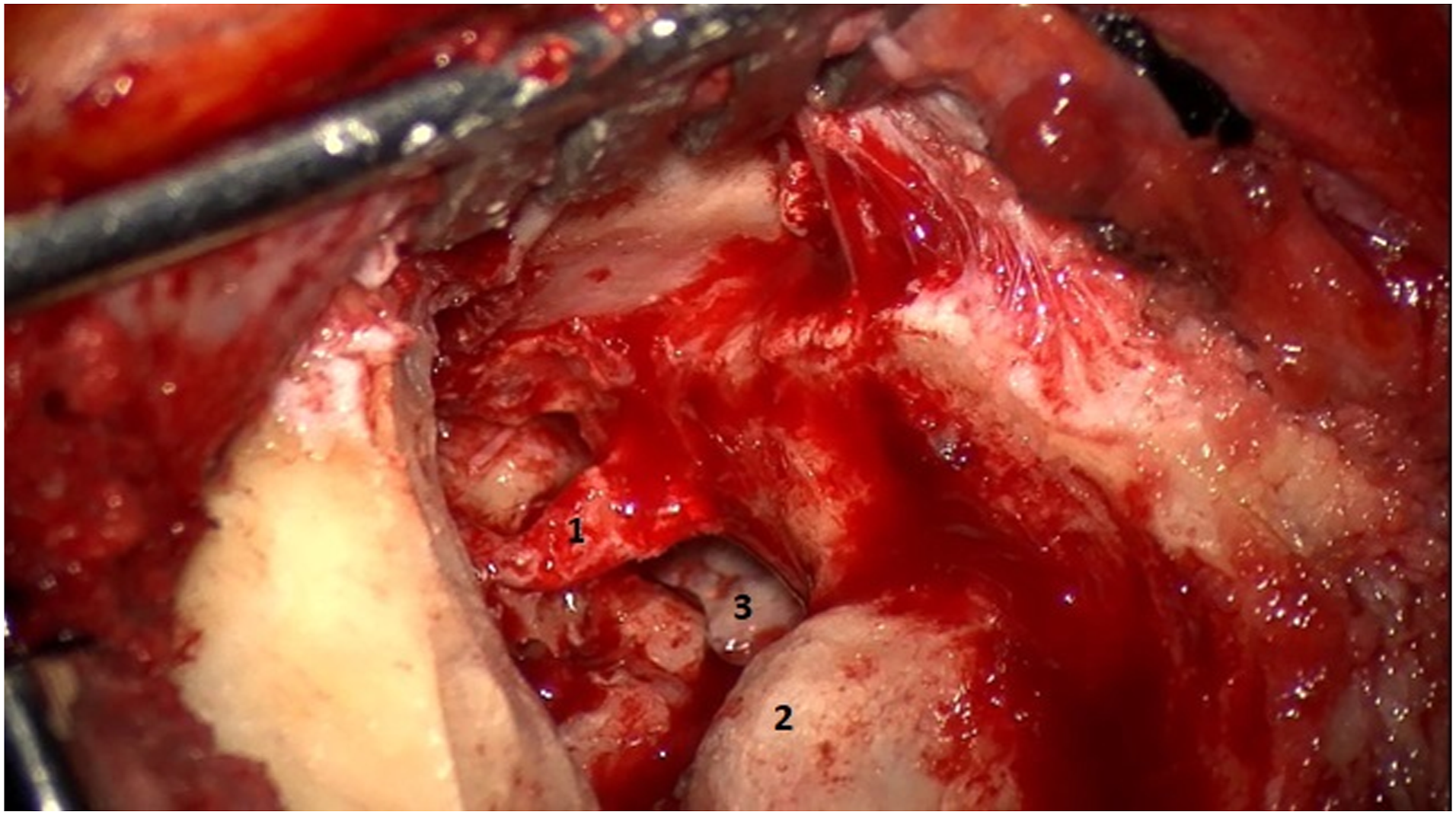
In massive PBCs hearing preservation is usually sacrificed to achieve radicality and to avoid recurrence. In our series, one patient presented a massive cholesteatoma that mainly involved the posterior labyrinth and the internal auditory canal: hence a modified translabyrinthine approach was chosen and a serviceable level of hearing was preserved (Figures 2 and 3). In all massive cases, an adjuvant endoscopic approach was performed. Massive petrous bone cholesteatoma: (1) jugular foramen nerves; (2) jugular bulb; and (3) removal of the cholesteatoma from the dura mate. Massive petrous bone cholesteatoma: (1) facial nerve; (2) sigmoid sinus; and (3) jugular bulb after removal of infralabyrinthine petrous bone cholesteatoma.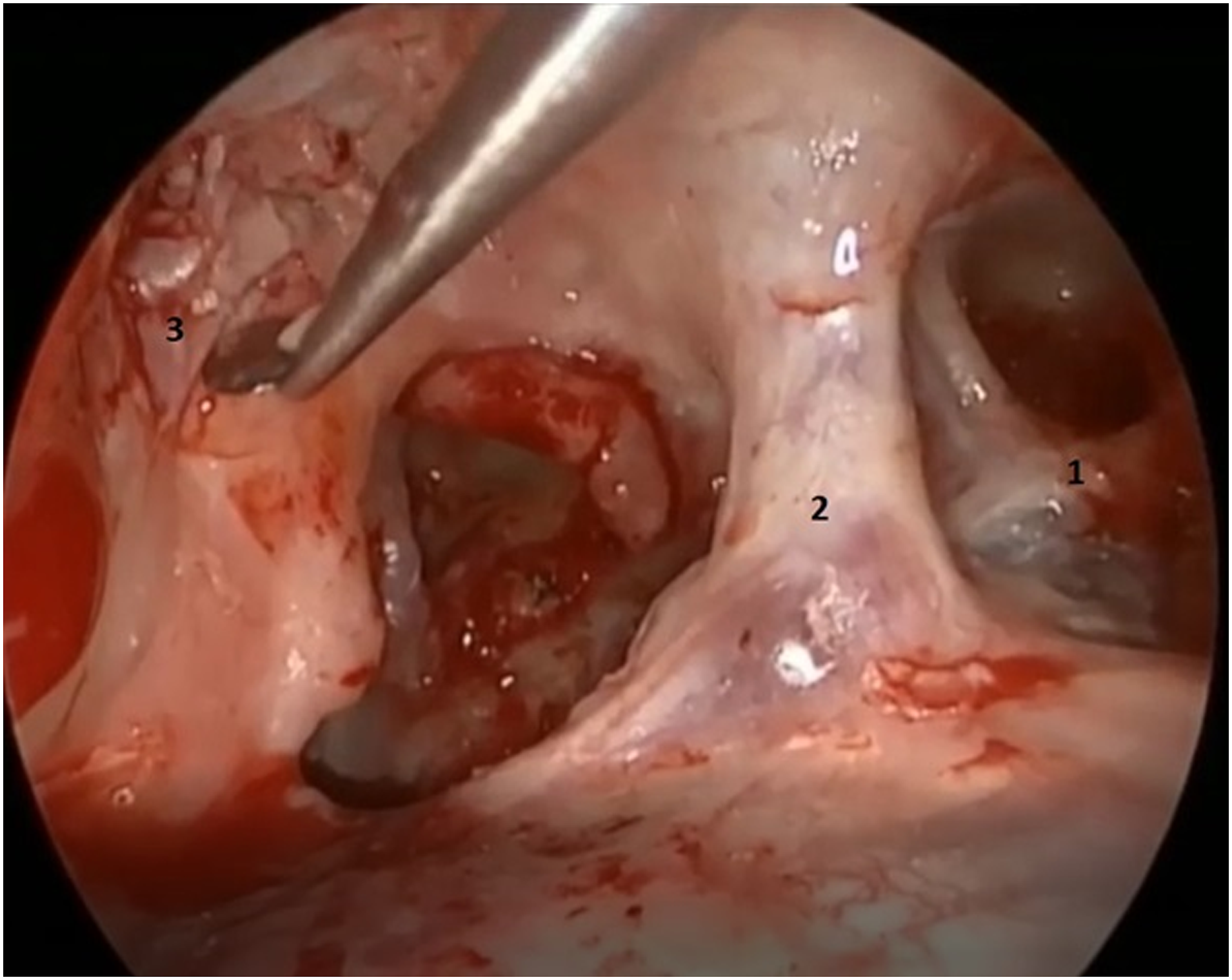
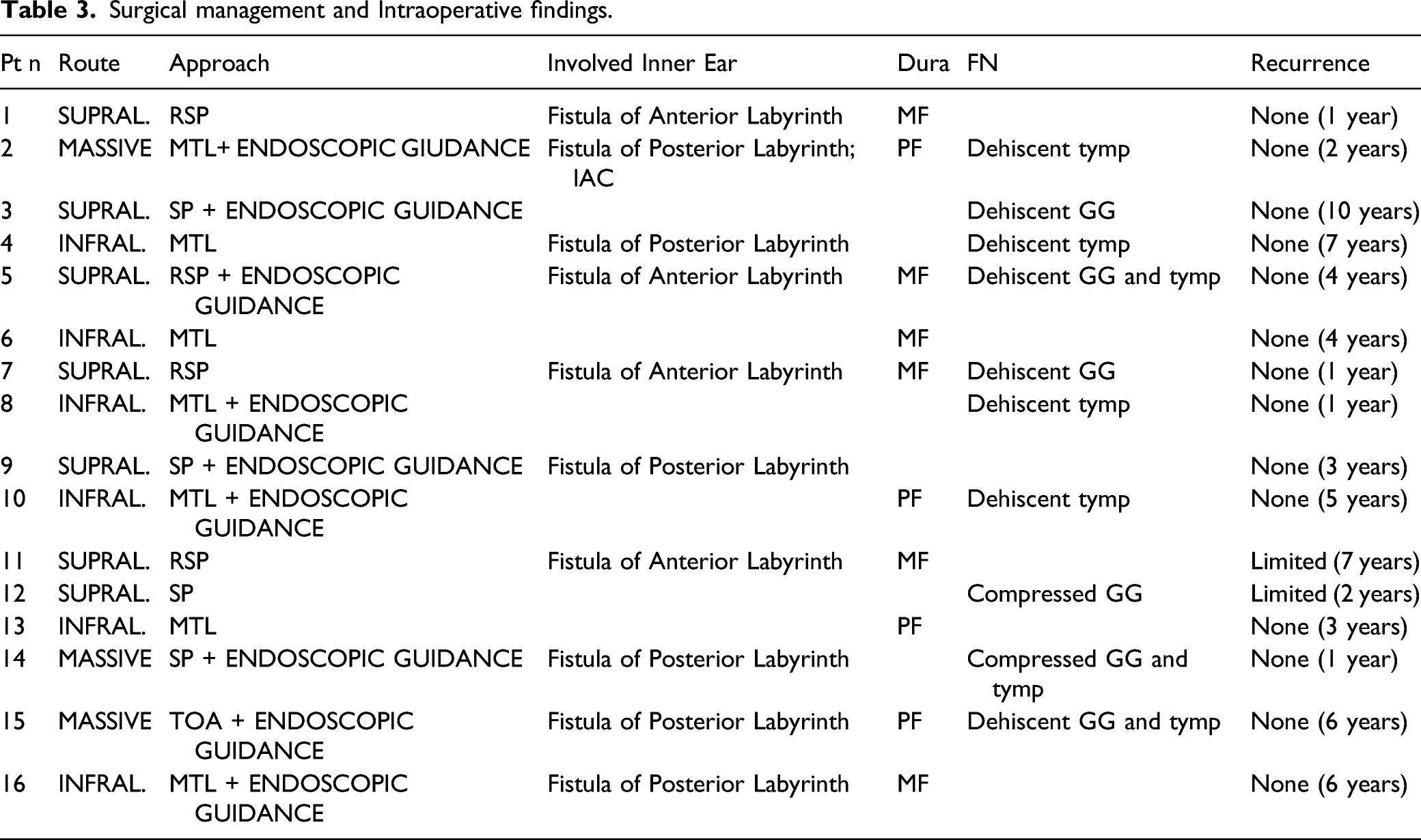
Surgical management and Intraoperative findings.
Partial erosion of the ossicular chain was observed in 3 patients, while 5 did not present any ossicular chain.
A fistula of the labyrinth was present in 62.5% of patients: in 19% (4/16) it was located in the anterior portion (cochlea), while in 37.5% (6/16) it was on the posterior side.
In one case of massive cholesteatoma, the lesion involved the internal auditory canal.
In the two cases with compression of the facial nerve, the cholesteatoma matrix was lifted off the nerve with a blunt dissector without requiring any graft.
Facial nerve function in two patients with preoperative palsy showed an improvement: 1 patient went to grade III HB from grade V HB; the other went to grade II HB from grade III HB (Table 2).
During surgery, no cochlear implant was positioned in anacusic patients. The same choice was made for bone conduction implants in patients with hearing preservation.
The follow-up period showed that 2 patients (12.5%) had a diagnosis of limited recurrence at CT imaging. Patients who constantly maintained their hearing presented a post-operative T2-weighted vestibule and cochlea signal (Figure 4). Two patients with hearing preservation underwent positioning of a Sophono device about two years later while three patients opted for a non-implanted bone conduction aid. None of the patients with anacusia opted for the cochlear implant. (a) CT scan examination of massive petrous bone cholesteatoma in contiguity with the dura mater; (b) CT scan evidenced the same massive PBC involving of internal auditory canal; (c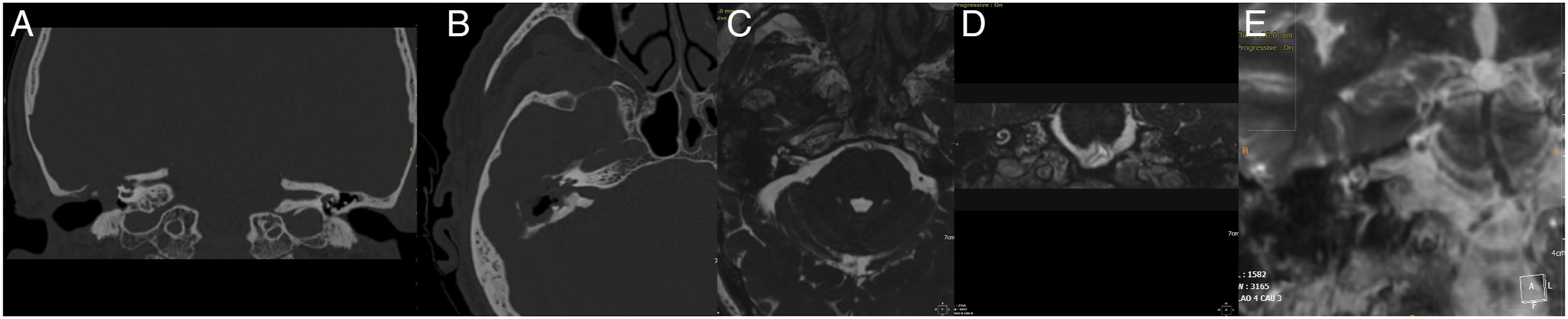
Discussion
Petrous bone cholesteatoma (PBC) is an epidermoid cyst of the petrous portion of the temporal bone with a congenital or acquired etiopathogenesis. Its growth is slow and asymptomatic in the deep portion of the temporal bone and it is commonly misdiagnosed for years. It has an erosive expansion that may involve several important structures (inner ear, facial nerve, internal carotid artery, and dura) even reaching as far as the cerebellopontine angle. 5
CT-scan imaging is the mainstay method since it displays isotropic sections and three-dimensional (3D) reconstructions of PBCs and their location in the temporal bone, thus providing fundamental information for surgical planning. 19
Magnetic resonance (MR) imaging provides preoperative information for differential diagnosis with cholesterol granuloma, mucocele, and tumors. It detects small lesions by DWI thinner sections imaging and is also essential for identifying signs of recurrence during follow-up. 19
Radical surgery of PBCs employs a variety of techniques whose target is to achieve removal of the entire cholesteatoma matrix with maximal preservation of nearby structures. 2 Surgical goals of all the procedures are radical excision of the disease; preservation of facial nerve function; prevention of CFS leakage; prevention of meningitis; preservation of hearing when feasible. 2
In our series, 87.5% of patients did not have any long-term recurrence. This incidence is in line with the literature, despite the different approaches performed. 6 Therefore, eradication of the disease may also be possible using less invasive techniques.
The facial nerve is a structure located in the temporal bone that may be involved by PBCs. Facial palsy is a common complication depending on compression and/or infiltration of the disease or may be a consequence of surgical removal procedures.
The incidence of preoperative facial palsy6,20,21 reported in the literature averages 51%. However, in our experience, its incidence is decreasing. In 2007, Magliulo 3 reported an incidence of 54% in patients with PBCs, treated at Sapienza University of Rome. From 2008 to 2020, in the same Department, preoperative facial palsy was observed in only 12.5% of PBC patients. This reduction may be ascribed to our protocol based on an early MRI diagnosis in patients with a suspect lesion.
Radical matrix removal is undoubtedly the aim of PBC surgery. Therefore, preservation of the otic capsule and hearing are secondary issues and depend on the extension of the disease and the possibility of preserving homeostasis of the anterior (cochlea) and posterior (vestibular) labyrinth (Table 1).
According to Sanna et al, 5 selected patients with supralabyrinthine PBC and serviceable hearing, but without any evidence of fistula, should be treated by combined middle fossa and trans-mastoid approach. However, this strategy is possible only in cases without any otic capsule involvement.
Prasad et al 6 evidenced post-surgical anacusia in 74.4% of supralabyrinthine PBCs treated with these surgical approaches. In our series, only Gardner–Robertson Class I–III patients were enrolled, namely those likely to maintain a serviceable level of hearing with/without aid after surgery. Supralabyrinthine PBCs were removed by subtotal petrosectomy, and in 43% this approach was combined with an adjuvant endoscopic approach. None of the patients were treated via the middle cranial fossa or transotic approach. Hearing outcomes showed preservation of the bone threshold in 68.75% of patients.
Surgical strategies for infralabyrinthine PBCs are subtotal petrosectomy with labyrinthectomy, translabyrinthine, and transotic approaches. Since they all sacrifice the otic capsule, in 1977 Fisch 8 proposed the infratemporal fossa approach as a hearing preservation technique. The translabyrinthine approach, and its related anacusia, is preferred for PBCs with labyrinthine fistula or internal auditory canal involvement.
Several surgical approaches for hearing preservation have been reported in the field of vestibular Schwannoma surgery.
In 1991, McElveen et al 14 proposed a modified translabyrinthine approach based on the destruction of all the semicircular canals and a concomitant sealing of the vestibule with bone wax. Sharma et al used this technique in 1 patient with PBC and reported a good long-term hearing outcome.
In 2004, Magliulo et al 15 described a modified translabyrinthine technique to preserve hearing during vestibular schwannoma surger, involving the internal auditory canal. It was a less invasive technique than McEleveen’s one because it spared the posterior labyrinth. In the recent literature, there are no reports of this technique being used for PBCs, although it was firstly performed to treat infralabyrinthine PBCs, associated with the endoscope in 50% of cases. Outcomes showed total hearing preservation in 5/6 patients (83%) including the case with internal auditory canal involvement. Several advantages of this approach emerged during follow-up: cholesteatoma was totally removed in all patients who underwent this method and none has shown signs of persistence or recurrence of the disease on radiological imaging.
The preservation of endolabyrinthic fluids in the vestibule is the basis of hearing preservation showed by a well-depicted post-operative T2-weighted labyrinthine signal (Figure 4). To date, no cases of recurrence have been reported.
Our data are in contrast with those reported by Moffat et al in 2008. 21 In their report, 43 patients were categorized according to the Moffat–Smith classification, showing a prevalence of massive (massive labyrinthine and massive labyrinthine apical), and supralabyrinthine types. Preservation of the otic capsule was performed in only 14% of patients, even though the series included patients with normal hearing and patients with serviceable hearing. The authors preferred to sacrifice hearing to gain better access for removing the cholesteatoma.
Similar findings were reported by Zaabi et al, 7 who described preservation of hearing after traditional PBC surgery in only 1 out of 6 patients. A limitation of their study was the lack of a PBC classification.
On the contrary, our results are in line with Senn et al, 22 who reported 82% of hearing preservation in patients treated with traditional approaches. However, the percentage of infralabyrinthine PBCs was low (10%), despite the supralabyrinthine ones (67%). Moreover, they reported hearing preservation techniques with a high rate of recurrence (19%), while in our cases none of the patients treated with a modified translabyrinthine approach presented evidence of recurrence during follow-up.
The endoscopic surgical technique is a recent source of debate due to its increased use in association with microsurgery. According to Orhan et al, 23 the association with an angled endoscope avoids invasive techniques (es: middle fossa) better visualizing the hidden area of the temporal bone and allowing a more radical removal of the cholesteatoma matrix, while reducing the incidence of disease recurrence.
Moreover, the improved view of anatomic recesses helps inner ear preservation and hearing function. The disadvantages of this technique are its two-dimensional vision and the need to perform one-handed surgery. 24
Gao et al, 25 using the combined microscopic and endoscopic technique, reported cochlea preservation in 76.9% of patients with supralabyrinthine PBC, followed by 66.7% of infralabyrinthine and 66.7% of infralabyrinthine-apical ones.
In our series, the endoscope was mainly used in revision surgery and in cases of more extensive PBCs, providing a better view of the potential dehiscence of the facial nerve, dura mater, and labyrinthine fistula.
The main limitation of this paper is the small sample reported, due to the rarity of the disease. Therefore, further multicenter studies with larger samples are under way to confirm these results.
Conclusions
PBC is a rare disease that requires surgical treatment. Its management is based on radical excision evaluating preoperative hearing function, facial function, and the risk of recurrence. Recently, the introduction of modified surgical approaches, able to preserve the anatomical-functional structures, have brought about an improvement in post-operative hearing outcomes.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Author Contributions
Giuseppe Magliulo made a substantial contribution to the concept and design of the work; Irene Claudia Visconti, Giannicola Iannella, and Daniela Messineo: acquisition, analysis, and interpretation; Annalisa Pace and Alessandro Milani: acquisition, analysis, interpretation of data, and draft the article; Antonino Maniaci and Valeria Rossetti revised it critically for important intellectual content and approved the version to be published; Salvatore Cocuzza and Giuseppe Magliulo approved the version to be published; All authors have participated sufficiently in the work and take public responsibility for appropriate portions of the content.