
Abstract
Non-iatrogenic traumatic facial paralysis is most common in intratemporal facial nerve injury caused by temporal bone fracture, followed by intraparotid facial nerve branch injury. Facial paralysis caused by injury to the extratemporal trunk of the facial nerve is extremely rare. We present a case of a 60-year-old man suffering from immediate complete left peripheral facial paralysis due to blunt transection of extratemporal trunk of facial nerve by stabbing with a car key. There was a facial nerve defect about 1 cm in length. The great auricular nerve was grafted to repair the facial nerve. Over 12 months, his facial nerve function improved to a House–Brackmann III/VI.
Introduction
Non-iatrogenic traumatic facial paralysis is most common in intratemporal facial nerve injury caused by temporal bone fracture, followed by intraparotid facial nerve branch injury. Facial paralysis caused by injury of extratemporal trunk of facial nerve is extremely rare. This work presents what may be the first case report of facial paralysis as the result of blunt transection of the extratemporal trunk of the facial nerve by stabbing with a car key at the stylomastoid foramen.
Case Study
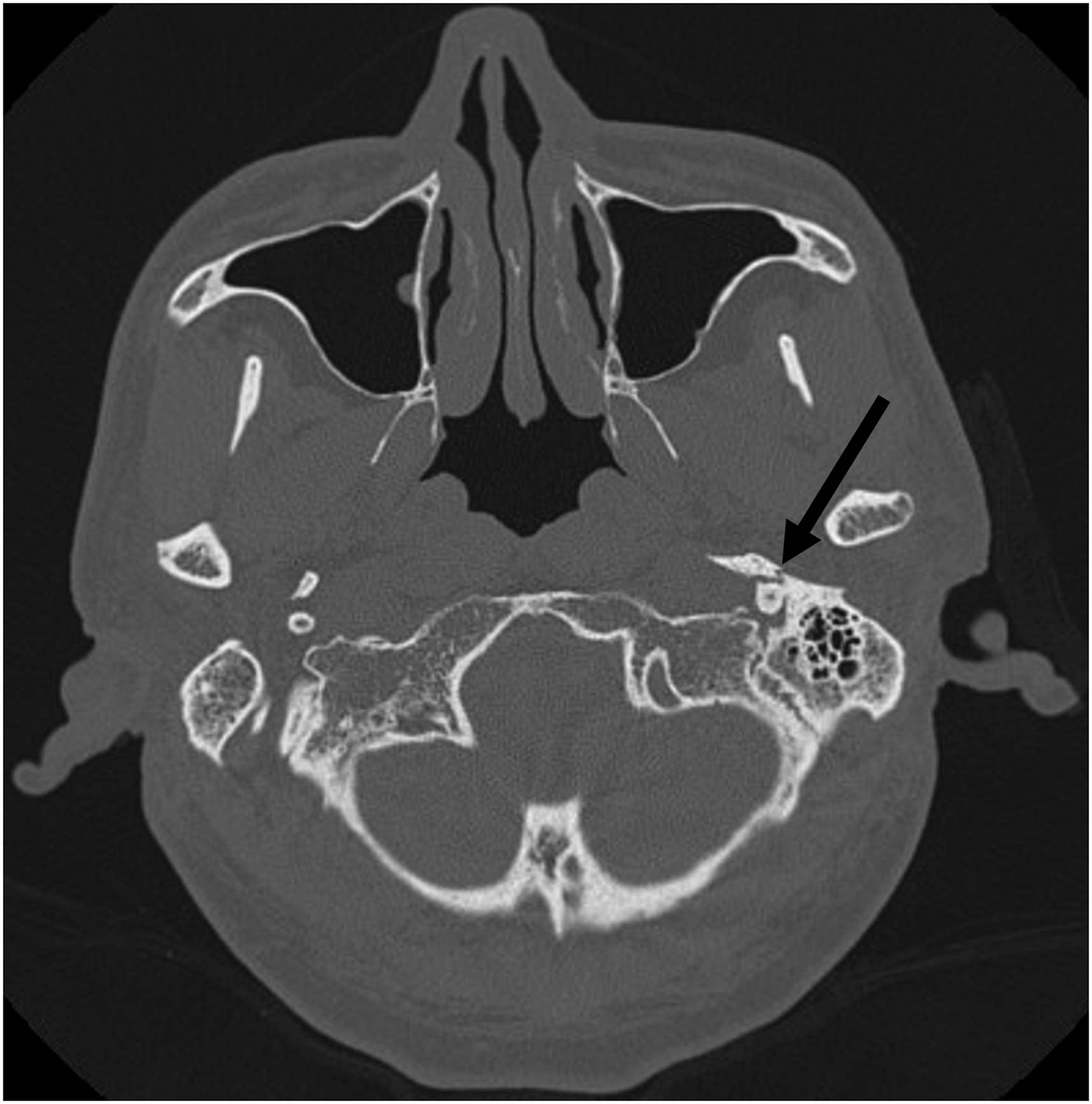
A 60-year-old man suffered from posttraumatic complete left peripheral facial paralysis immediately after a stabbing with a car key. He was referred to our department with a 5-mm stab wound inferior to the left tragus and another 5-mm stab wound anterior to the angle of mandible (Figure 1). He cited no hearing loss or bloody otorrhea. No abnormality was observed in the left external auditory meatus or tympanic membrane. High-resolution CT of the temporal bone showed fracture line in the vaginal process (Figure 2) and gas accumulated in the soft tissue beneath the left external auditory meatus. Stab wounds. Arrow: wound inferior to the left tragus; arrowhead: wound anterior to the angle of mandible. High-resolution CT of the temporal bone showed fracture line in the vaginal process (Arrow).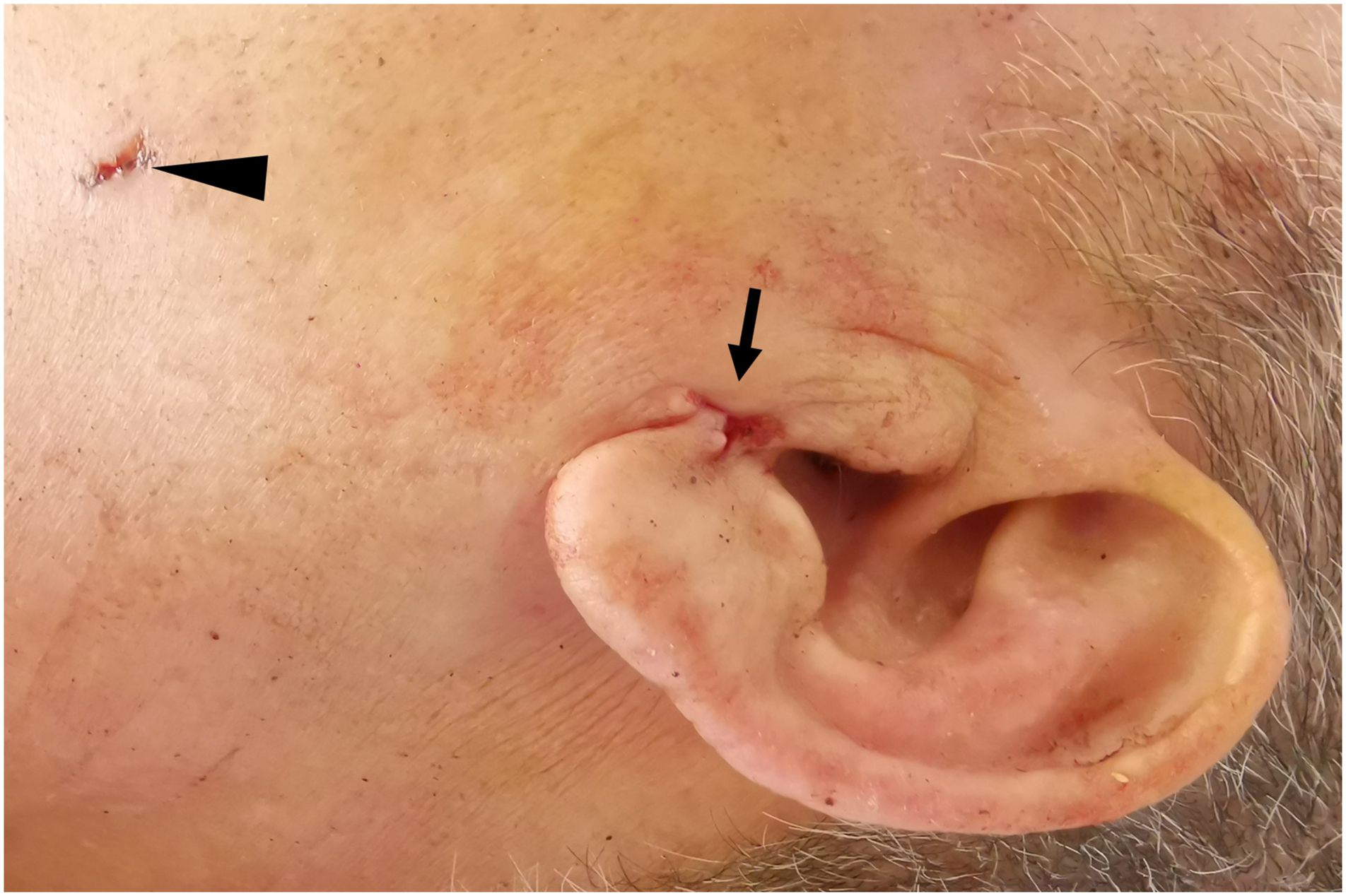
A recommendation was made for surgical exploration because injury to the left facial nerve extratemporal trunk was considerable, and injury to the marginal mandibular nerve could not be excluded. Surgical exploration was conducted with the assistance of a facial nerve monitor, and there was no injury to the marginal mandibular nerve. Following the marginal mandibular nerve back to the bifurcation, the extratemporal trunk was found to be bluntly severed, and there was a defect of about 1 cm with shrinkage of the proximal trunk to the stylomatic foramen. Then, canal wall up mastoidectomy with excision of mastoid tip was performed, and the mastoid segment of the facial nerve was dissected to the stylomatic foramen to fully expose the severed ends of the facial nerve. Because the facial nerve defect was about 1 cm in length, it could not be directly anastomosed end-to-end, so the great auricular nerve was grafted to repair the facial nerve (Figure 3). The patient recovered well after surgery without hearing loss or parotid gland leakage. Over 12 months’ rehabilitation, his facial nerve function improved to a House–Brackmann III/VI (Figure 4). Graft of great auricular nerve. GAN: great auricular nerve; *: bifurcation; arrow: proximal trunk of facial nerve; arrowhead: distal trunk of facial nerve. (A) House–Brackmann grade before and (B) 1 year after surgery.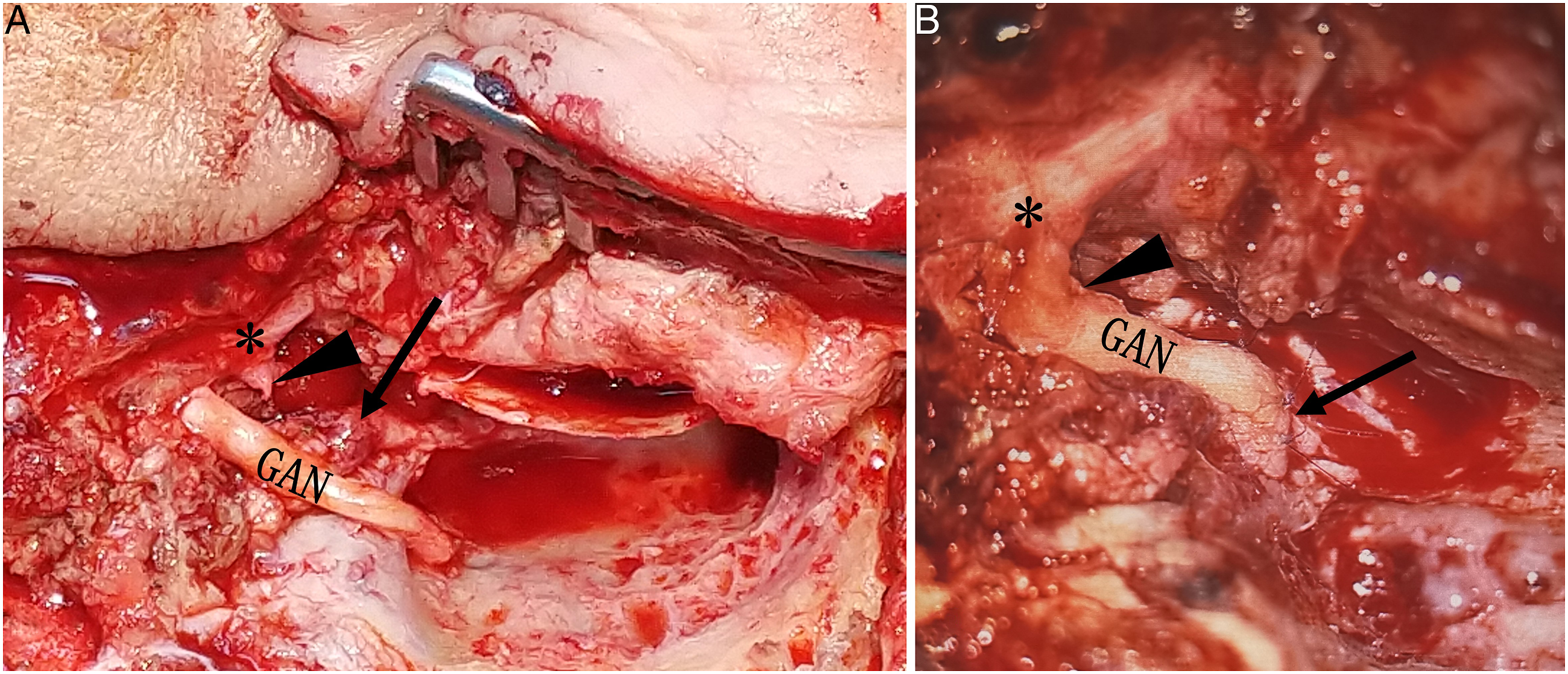

Discussion
There are a wide variety of etiologies for traumatic facial paralysis, such as temporal bone fracture, stab wound, gunshot injuries, and forceps delivery. 1 Although temporal bone fracture is the most common cause of traumatic facial paralysis, stab wounds to the extratemporal trunk are extremely rare. To our knowledge, this is the first report of a facial paralysis as the result of blunt transection of extratemporal trunk of facial nerve by stabbing with a car key.
Moss reported a case of total facial paralysis caused by the stabbing of the trunk of the facial nerve during a core needle biopsy of a deep lobe parotid tumor. The patient’s facial nerve function improved to a House–Brackmann III/VI 4 months after injury, although there was no discontinuity of the facial nerve. 2
If the facial nerve is severed, the repair should be performed as promptly as possible. That is because within the first 72 h after transverse injury to the facial nerve, the distal nerve can still be stimulated by a facial nerve monitor. This makes it easy to find the distal nerve. Tension-free end-to-end repair is the best choice, and the best recovery of facial nerve function can be obtained using this method. If the defect cannot be anastomosed end-to-end without tension, nerve graft should be considered. The greater auricular nerve and sural nerve are the most common donors.3,4
Graves reported a complete facial paralysis caused by a transection of extratemporal trunk of the facial nerve with a stab wound very close to the wound location in our case. According to his report, the nerve trunk was found to be severed, creating a gap about 0.5 cm in length, and the facial nerve was anastomosed end-to-end. Twenty months later, the patient had good facial symmetry but some mass action with voluntary movements. 5 As for our case, owing to the blunt stab wound caused by a car key, the defect of facial nerve was longer, about 1 cm, and end-to-end suture without tension was impossible. Instead, we decided to repair the facial nerve defect with the great auricular nerve; because the great auricular nerve is located near the surgical area, it is easy to harvest without additional incision, and its diameter is similar to that of the facial nerve. 4 Over 12 months, the facial nerve function of this patient improved to a House–Brackmann III/VI. This is consistent with the best results reported in the literature.
Conclusion
Stab wound to the extratemporal trunk of the facial nerve is extremely rare. This is the first report of a facial paralysis as the result of blunt transection of extratemporal trunk of the facial nerve by stabbing with a car key. Grafting of the great auricular nerve can achieve good improvement of facial function.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.