
Abstract
Facial nerve meningioma is exceedingly rare and tends to affect the geniculate ganglion. We present a case of facial nerve meningioma located in the internal auditory canal with a “labyrinthine tail,” mimicking facial nerve schwannoma. The clinical and radiological features, growth patterns, and surgical management were reviewed. Progressive facial paralysis was the main syndrome, similar to other facial nerve tumors. When facial nerve function is worse than House-Brackmann grade III, surgical resection should be performed with facial nerve reconstruction.
Introduction
Meningioma is a common intracranial neoplasm that arises from the arachnoid cells of the meninges. 1 Although a large meningioma centered in the temporal bone or cerebellopontine angle can in some instances secondarily involve the facial nerve,2,3 primary facial nerve meningiomas are rare. We report a case of meningioma intrinsic to the facial nerve from the porus acusticus internus to the geniculate ganglion that was initially suspected to be a facial nerve schwannoma.
A previously healthy 53-year-old female was referred to our department because of the discovery of a right internal auditory canal (IAC) tumor. The main complaints were hearing loss and right-side facial paralysis lasting for 3 years and 6 months, respectively. Her hearing loss was first considered sudden hearing loss, with no magnetic resonance imaging (MRI) or computed tomography (CT) scan results at that time. Due to progressively worsening facial paralysis for 6 months, an IAC MRI was performed in a local hospital, which revealed a tumor involving the IAC, the labyrinthine portion, and the geniculate ganglion of the facial nerve. On physical examination, her facial nerve function was House-Brackmann (HB) grade VI. Pure-tone audiometry showed profound sensorineural hearing loss. High-resolution computed tomography (HRCT) demonstrated expansion of the IAC and the geniculate ganglion region, especially the posterior wall of the IAC (Figure 1). On MRI, T1-weighted images revealed a homogenous isointense mass that was intensely enhanced after administration of gadolinium contrast, but only subtle hyperintensity was observed on T2-weighted images (Figure 2).
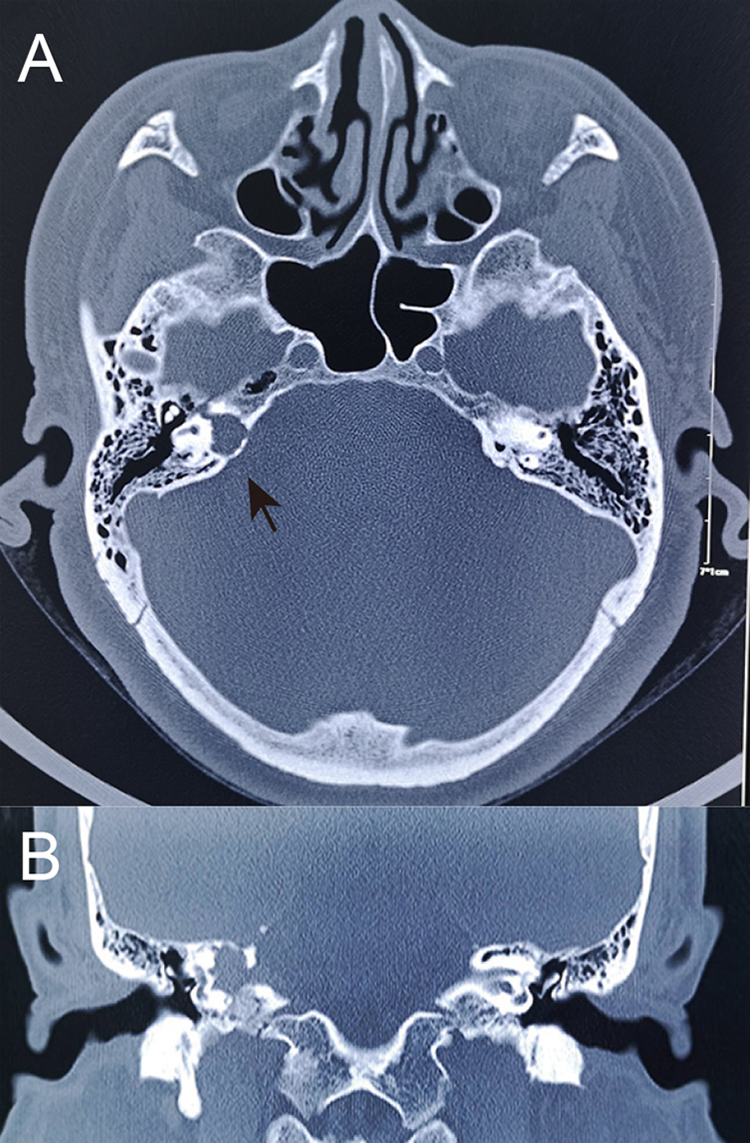
High-resolution computed tomography (HRCT; 1 mm section, bone algorithm). A, Axial HRCT scan shows erosion of the posterior wall of the IAC (black arrow) and enlargement of the labyrinthine segment and geniculate ganglion. B, Coronal HRCT image of the “globular” growth pattern.
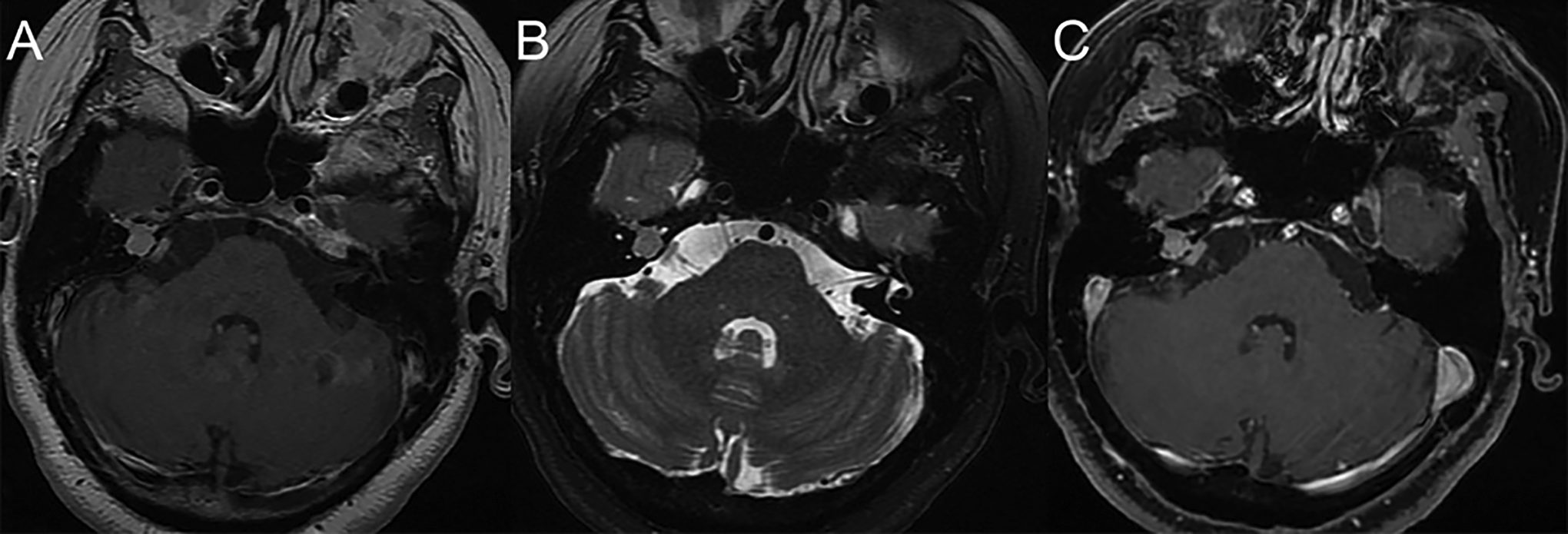
A, Axial T1-weighted magnetic resonance imaging. The mass located in the IAC and geniculate ganglion region shows a homogeneous isointense signal. There is subtle hyperintensity on axial T2-weighted magnetic resonance imaging (B) and intense enhancement after administration of gadolinium contrast (C). IAC indicates internal auditory canal.
A right translabyrinthine approach showed that the tumor had infiltrated the IAC contents and elongated to the proximal tympanic segment of the facial nerve. The remaining tympanic segment and mastoid segment of the facial nerve appeared to be normal, and negative margins were confirmed by stump frozen section. The patient underwent total tumor removal with a great auricular nerve cable graft.
The pathologic diagnosis of meningioma was meningothelial meningioma (World Health Organization grade I) characterized by lobules of epithelioid tumor cells delimited by collagenous septa. Moreover, the tumor cell clusters were positive for epithelial membrane antigen, supporting the diagnosis of meningioma (Figure 3).
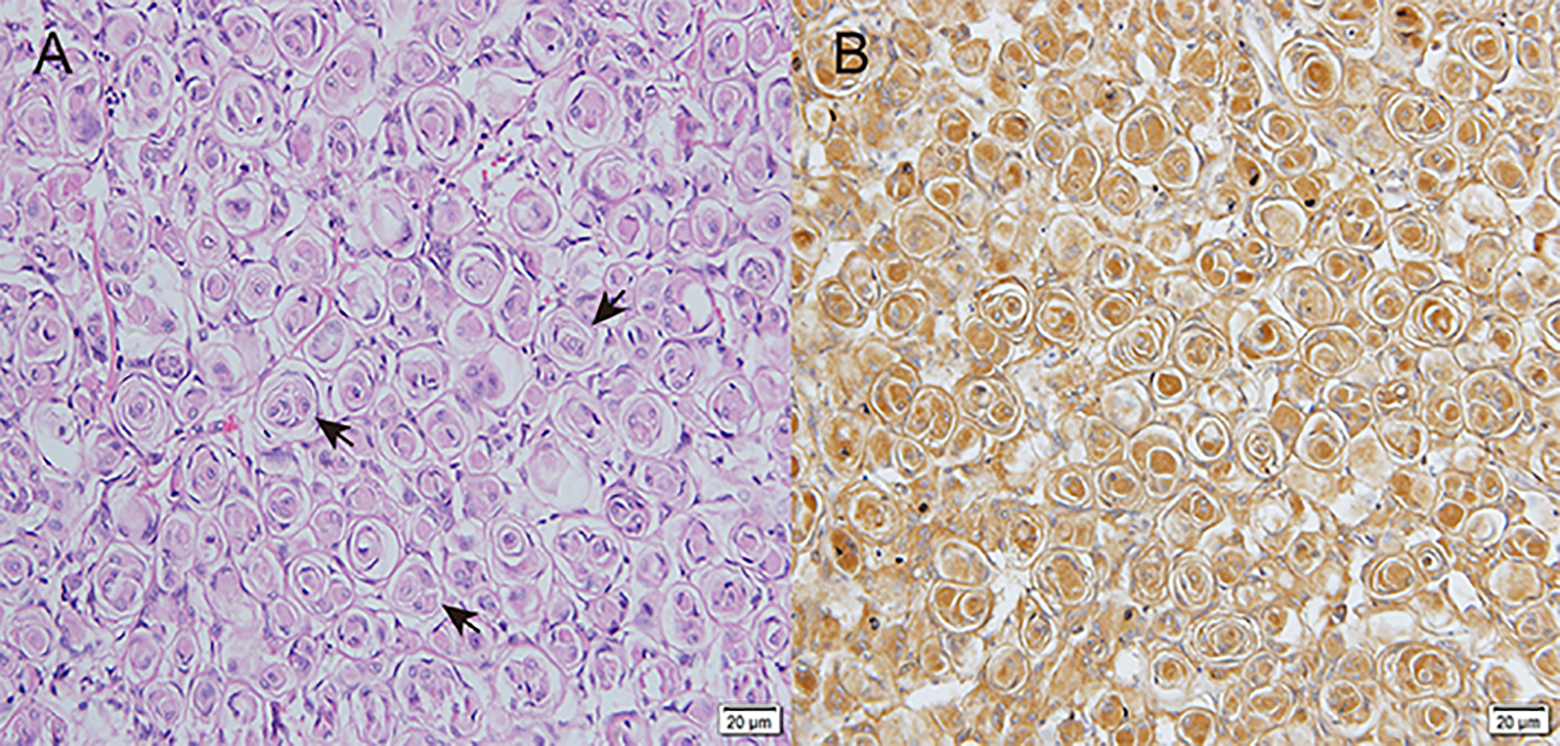
Histopathological features of the tumor. A, The tumor cell lobules (short black arrow) were delimited by collagenous septa. Hematoxylin and eosin stain, ×20 magnification. B, The tumor cells were positive for epithelial membrane antigen (EMA) by immunohistochemistry (x20 magnification.).
At the 1-year follow-up, her facial nerve function had recovered to HB grade III, and there was no evidence of residual tumor by radiological evaluation.
Discussion
Intrinsic facial meningiomas in the temporal bone are rare. To our knowledge, no more than 20 cases, mainly involving in the geniculate ganglion, have been reported to date.4-6 Overall, meningiomas are thought to originate from arachnoid cells, especially on those villus protruded into the walls of dural veins and sinus. 7 However, it is not surprising that meningiomas may also arise from the facial nerve. Nager 8 first described arachnoids cells displaced along the facial nerve during embryogenesis. At approximately 5 to 6 weeks gestation, the facial nerve exits the neural tube with a sheath of arachnoid cells and the dura. 9 The dura terminates within the IAC, but the arachnoid cells may continue toward the geniculate ganglion or beyond and ultimately fuse with the endoneurium and perineurium of the facial nerve. 8 These ectopic arachnoid cells within the facial nerve sheath might explain the origin of intrinsic facial nerve meningioma.
In general, it is difficult to distinguish intrinsic facial nerve meningiomas from facial nerve schwannomas. 10 Moreover, a tumor was confined to the IAC may even be confused with vestibular schwannoma. 3 Indeed, their radiographical features are not distinguishing. Magnetic resonance imaging finding for both facial nerve meningioma and schwannomas are often described in the literature as isointense or hypointense on T1-weighted imaging and hyperintense on T2 sequences, showing enhancement with contrast.2,5 On HRCT, bony erosion and asymmetrically enlarged IAC are common for these 2 different tumors. Although intracranial meningiomas can have a broad-based “tail” and intratumoral calcifications, intrinsic facial nerve meningiomas do not usually present with these features but have an appearance nearly identical to schwannomas.2,5 The preoperative radiographic diagnosis for our patient was facial nerve schwannoma, particularly due to the “labyrinthine tail” sign. However, a few slight differences in HRCT were discovered during retrospective analysis after surgery, whereby the expansile IAC appeared to be globally and not a typical trumpet shape, the latter of which is common in schwannoma. In addition, the posterior wall of the IAC was eroded with irregular margins. Combined with the 2 growth patterns of intracranial meningioma, we considered that the IAC-portion meningioma in our patient conformed with a “globular” growth pattern,10,11 and the growth pattern of the fallopian canal portion was “en-plaque.” The 2 growth patterns might be concurrent in a single case, as in our patient.
Regardless of whether a facial nerve lesion represents a schwannoma or meningioma, surgery is the mainstay of treatment. 12 An individualized approach is taken according to the preoperative hearing level and facial nerve function. Isolation via the middle cranial fossa approach or with a transmastoid approach is commonly applied for hearing preservation, and the translabyrinthine approach is used when a patient has total hearing loss.5,12 As it is impossible to find a cleavage for stripping out meningioma from the facial nerve, 5 the infiltrated facial nerve must be removed and reconstructed by grafting or anastomosis. The best postoperative facial function of HB grade III can be achieved,5,10,12 consistent with our case, and it is our policy to perform surgical intervention only when the paralysis is severe, at HB grade III and higher. Furthermore, meningioma shows a higher tendency for recurrence than schwannoma,9,10 and drilling more of the temporal bone is needed, especially around the IAC and geniculate ganglion.
In conclusion, both “globular” and “en-plaque” growth patterns coexisted in this case. Resection with facial nerve reconstruction was necessary to achieve complete disease control, with relatively good facial function.
Footnotes
Authors’ Note
The patient’s permission was obtained.
Declaration of Conflicting Interests
The author(s) declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.