
Abstract
Introduction
Pilomatrixomas are benign neoplasms derived from hair follicle matrix cells.
1
They occur most commonly in the head and neck skin and more than 60% of these tumors present within the first 2 decades of life.
2
This makes pilomatrixoma one of the most common soft tissue head and neck tumors of childhood.
3
A pilomatrixoma typically presents as a solitary, firm, slowly enlarging, mobile, well-circumscribed subcutaneous nodule (Figure 1). They are often eccentric in shape and are adherent to overlying skin at their hair follicle of origin. Pilomatrixomas consistently remain within the skin and subcutaneous fat and do not violate the superficial fascia of the face. Complete surgical excision is curative. A typical pilomatrixoma of facial skin. Note projection and skin discoloration.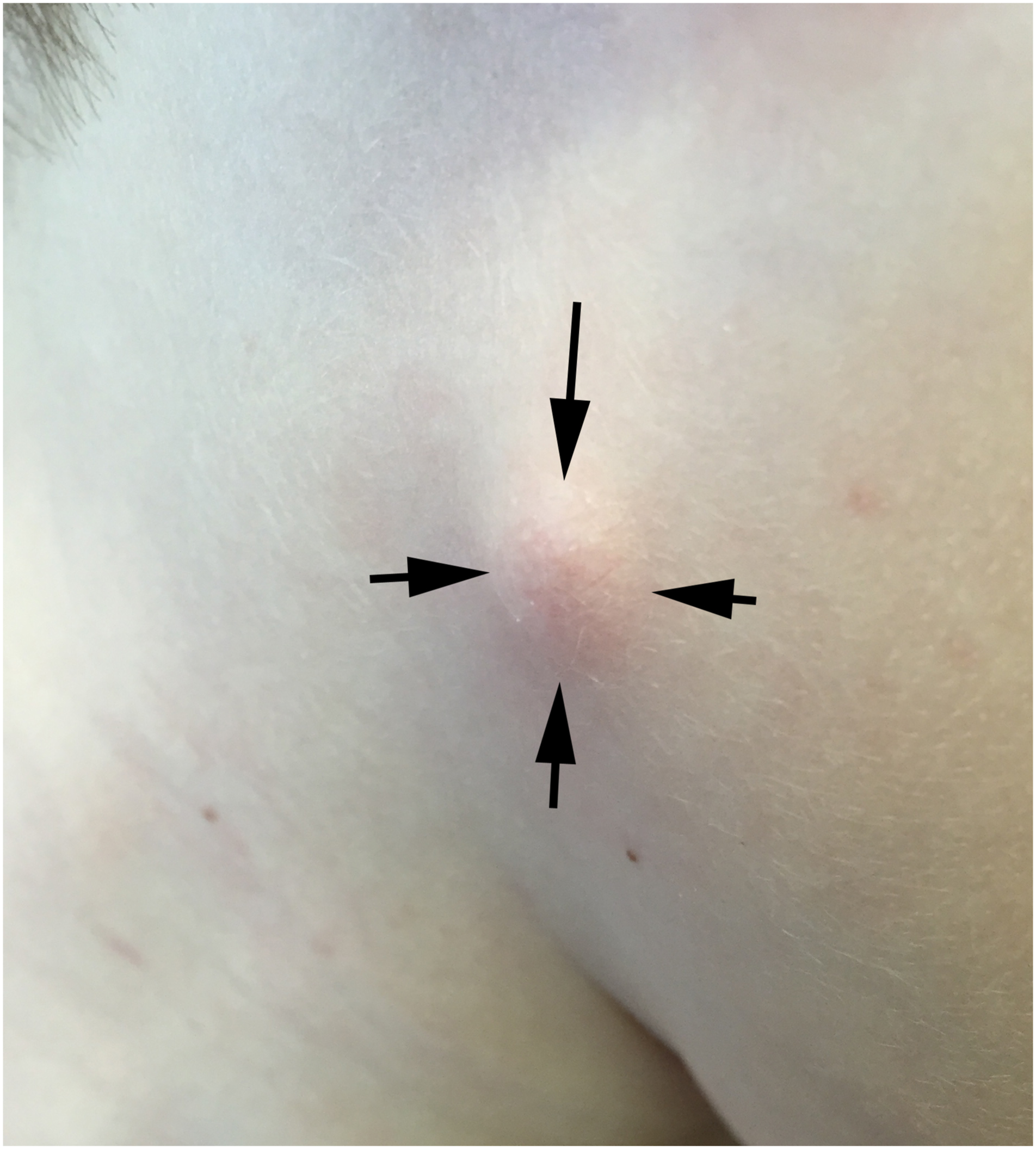
The clinical presentation of pilomatrixomas is so characteristic that many experienced surgeons will excise them without prior imaging. 1 This has been the practice of the senior author (GI) for the last 2 decades. We review the results of this approach to determine whether physical examination alone differentiates pilomatrixoma from other similar soft tissue tumors of the pediatric head and neck.
Methods
The study was exempted by the Temple University’s institutional review board (IRB protocol 24277). Using the “Find” feature of Microsoft Word™ we queried a 20-year computerized collection of office letters and operative reports using the search term “pilomatrixoma.” This identified any child who was thought to have a pilomatrixoma preoperatively or who was found to have a pilomatrixoma on pathologic examination. All office notes and operative letters for any identified child were then reviewed. Clinical presentation, diagnostic workup, treatment, and postoperative results as well as patient age, gender, past medical history, and location of the lesion were recorded.
Surgeries were performed by the senior author with the assistance of residents. In each case, an elliptical incision was made, preferably oriented along a line of relaxed skin tension, around the hair follicle of origin. The hair follicle was identified by dimpling the skin between finger and thumb (Figure 2). Dimpling on palpation (arrow). This lesion proved to be a giant molluscum contagiosum lesion rather than a pilomatrixoma.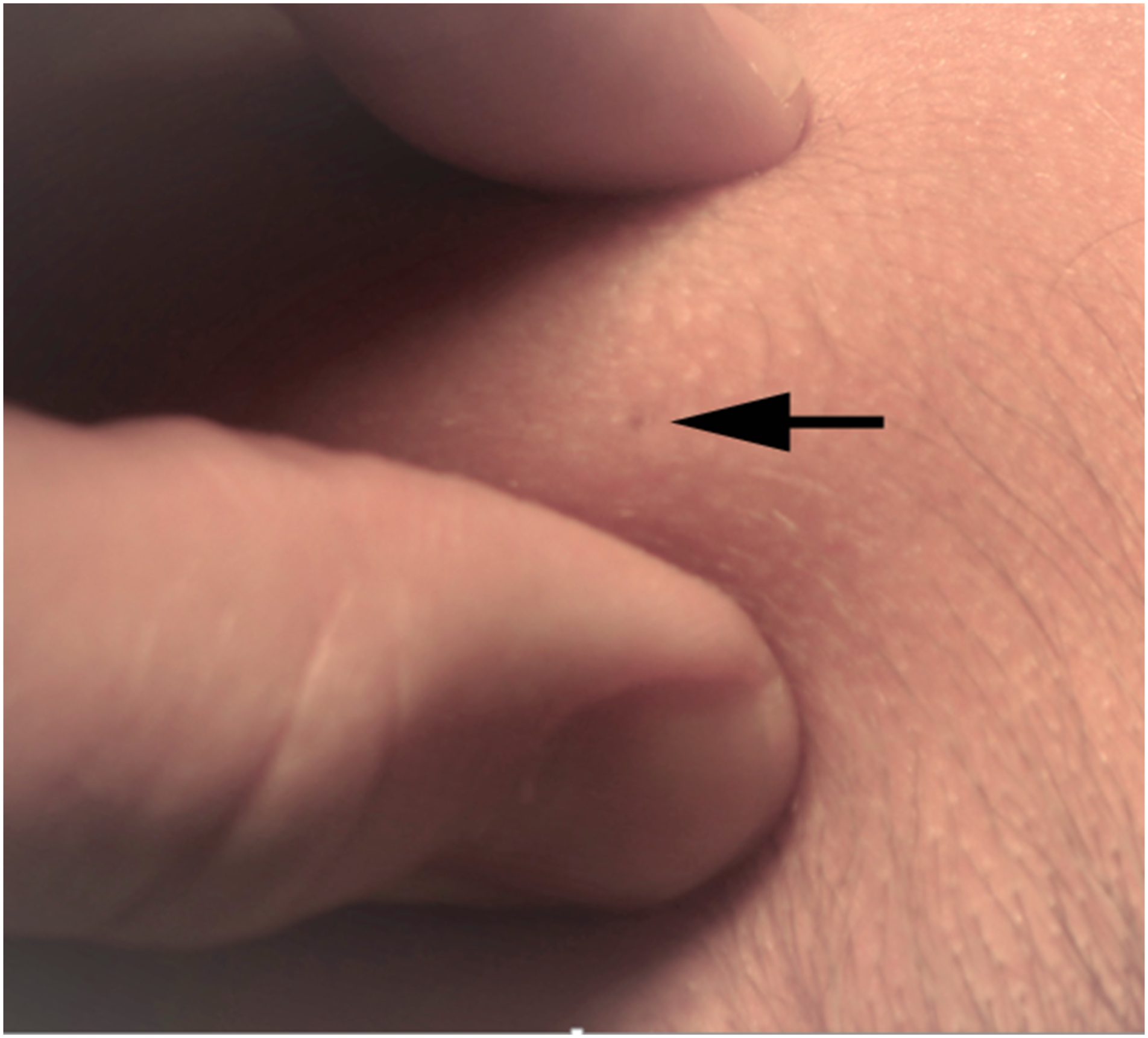
The tumors were excised under loupe magnification including the attached overlying skin ellipse. The pilomatrixoma was dissected free from the surrounding subcutaneous fat with care to include the entire lesion without violating its eccentric projections. The patients were seen a week later for suture removal and review of pathology. No additional follow-up was scheduled but family were asked to contact the office should there be signs of infection or recurrence.
Results
Eighteen patients presented to our pediatric otolaryngology practice between 2001 and 2021 with historical and physical findings consistent with pilomatrixoma. These were isolated, slow-growing masses that were firm, nontender, and mobile in the subcutaneous plane. Of the 18 patients, 7 were male and 11 were female. Ages ranged from 1.5 to 14 years, with a mean of 7.5 years. Most of the lesions (12) were located in the head and face, while the rest (6) were found in the neck. All patients presented with solitary masses. None of the lesions in this series was evaluated by preoperative ultrasonography. None of the children had a history of prior pilomatrixoma or associated syndromes (i.e,, Gardner and Turner syndromes). None was diagnosed with a second pilomatrixoma in the years following diagnosis. All patients were treated with complete surgical excision. One small lesion of the auricular helix was thought to be a dermoid cyst, but proved to be a pilomatrixoma on histologic examination (patient #19) (Figure 3). Pilomatrixoma of the auricle, initially thought to be a dermoid cyst.
Pathology confirmed pilomatrixoma in 15 of the 18 children thought to have a pilomatrixoma preoperatively (positive predictive value = .833). The other 3 patients were found to have an epidermal inclusion cyst, a ruptured trichilemmal cyst, and a giant molluscum contagiosum lesion, respectively. No recurrences were identified on short-term follow-up or on subsequent office visits.
Discussion
Clinical diagnosis of pilomatrixomas is usually based on classical features noted on physical exam. As a true benign neoplasm, pilomatrixomas lack the spherical symmetry of cutaneous cysts. Pilomatrixomas vary greatly in size with an average diameter of 1.2 cm in a large retrospective series. 4 Up to 90% of pilomatrixomas are calcified, so they are firm to the touch and can distend the overlying skin (Figure 1). The tumor is nontender and mobile in the subcutaneous fat but attached to the overlying skin. 5 2 signs clinicians should look for on physical exam to help diagnose a pilomatrixoma are the “tent sign,” in which the skin is stretched over the tumor’s calcifications to form a tent-like structure, 6 and the “teeter-totter sign,” where pressing on 1 edge of the mass causes the opposite edge to jut out from the skin.7,8 Some of these tumors have a reddish or bluish hue. 7 The majority of pilomatrixoma cases involve a solitary tumor, while multiple or recurrent tumors may be associated with certain conditions, including myotonic dystrophy, Gardner syndrome, and Turner syndrome.9,10
Unfortunately, not all pilomatrixomas have this typical appearance. There is evidence that pilomatrixomas change in appearance and histology over time. In their seminal article, Kaddu et al
11
describe 4 morphologic stages in the development of pilomatrixoma: Early lesions are cystic structures lined by squamoid and basaloid epithelium. Fully developed lesions are lined by basaloid epithelium at their periphery and have zones of cornified material containing shadow cells (Figure 4). Early regressive lesions have no visible epithelium and are composed of pink hair matrix material with shadow cells and multinucleated giant cells. Late regressive lesions have no epithelial component and are composed of confluent masses of faulty hair material, and calcified shadow cells with little or no inflammatory infiltrate. (A) Low power H&E photomicrograph of pilomatrixoma, (B) On histology, a fully developed pilomatrixoma consists of basaloid cells in the periphery and keratinized, enucleated ghost or shadow cells in the center. As the ghost cells are derived from the peripheral basaloid cells, an intermediate transitional zone can be seen. Multinucleated giant cells (bottom left) can be identified as well.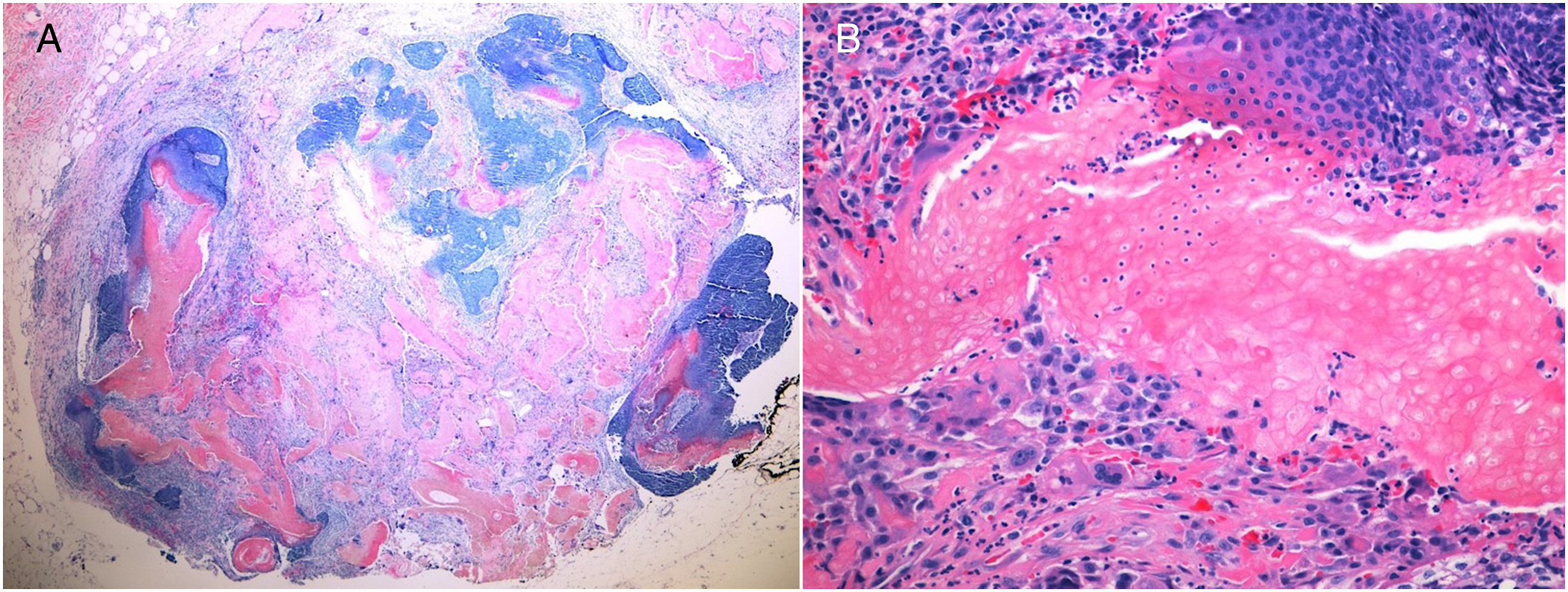
In these different life-cycle phases, pilomatrixomas vary in physical characteristics and in degree and type of calcification. 12 Early lesions have little or no calcification. Fully developed lesions have variable degrees of scattered calcification. Regressive lesions have clumped or arc-shaped calcium deposits, affecting their shape, texture, and ultrasound appearance. These variations may lead to misdiagnosis, especially of early lesions, on physical examination. This was the case with the lesion of the pinna (Figure 3) in our series.
Imitators
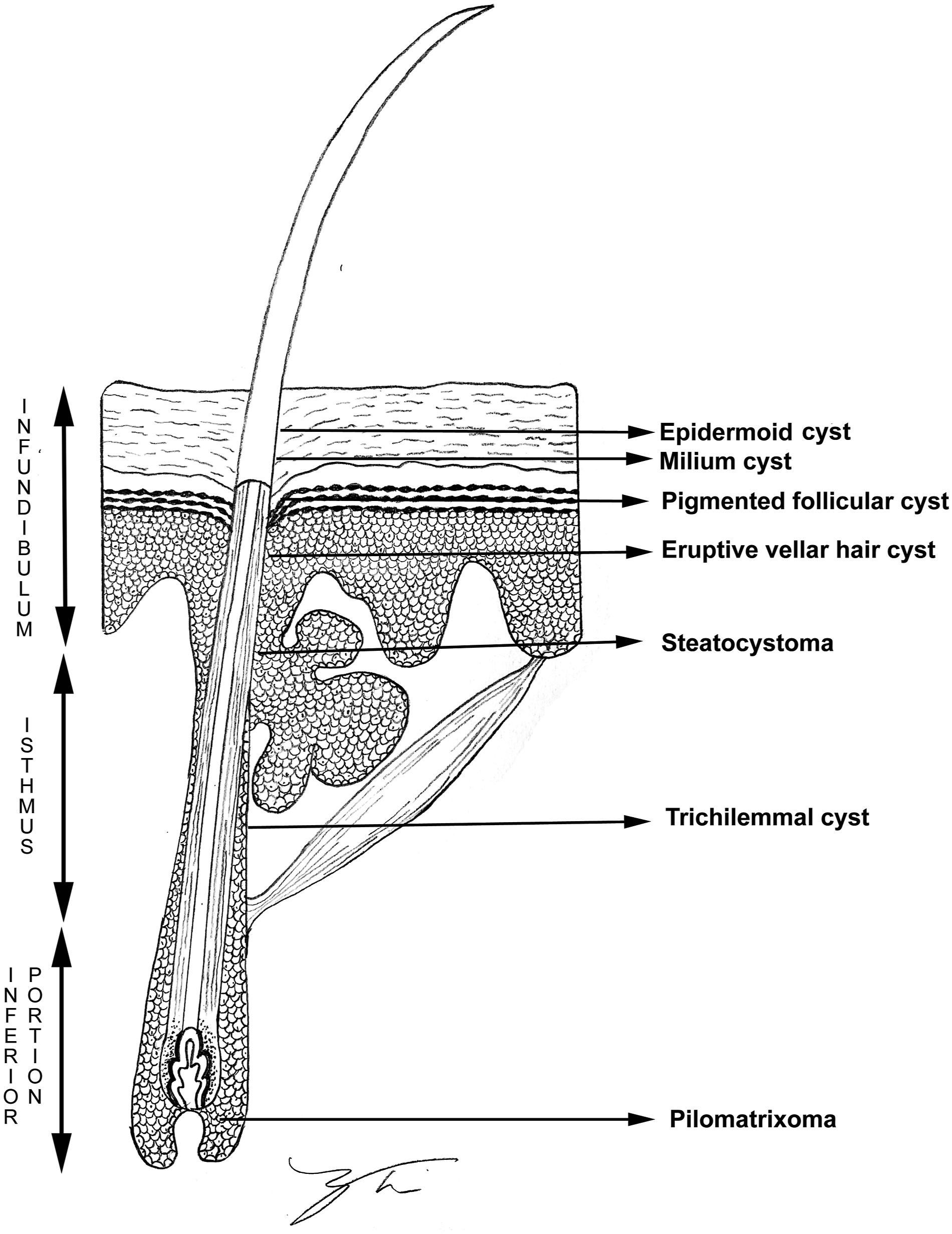
Further confounding accurate diagnosis are other cysts and tumors of pilosebaceous origin that may mimic a pilomatrixoma on clinical examination. These include epidermoid cysts and milium cysts, pigmented follicular cysts, eruptive vellus hair cysts arising from the superficial infundibulum; and steatocystoma, and trichilemmal cysts arising from the mid-portion (isthmus) of the hair shaft.
13
(Figure 5) Like pilomatrixomas, which arise from the deep inferior portion of the hair structure, follicular lesions can dimple the skin at their hair of origin and protrude into the dermis and subcutaneous fat. These lesions of pilosebaceous origin may be impossible to differentiate from pilomatrixomas clinically, especially if they are inflamed or partially calcified. Dermoid cysts, calcified lymph nodes, and regressed hemangiomas (which are also described as imitators) do not affect the overlying epidermis and can be differentiated on palpation. Drawing of hair follicle with proposed areas of origin for follicular lesions (Modified after Requena and Sanchez Yus
13
).
Out of the 18 patients presenting with masses consistent with pilomatrixoma on physical exam, we identified 3 imitating lesions: an epidermal inclusion cyst, a ruptured trichilemmal cyst, and a giant molluscum contagiosum lesion. We will discuss each in greater detail.
Epidermal Cyst
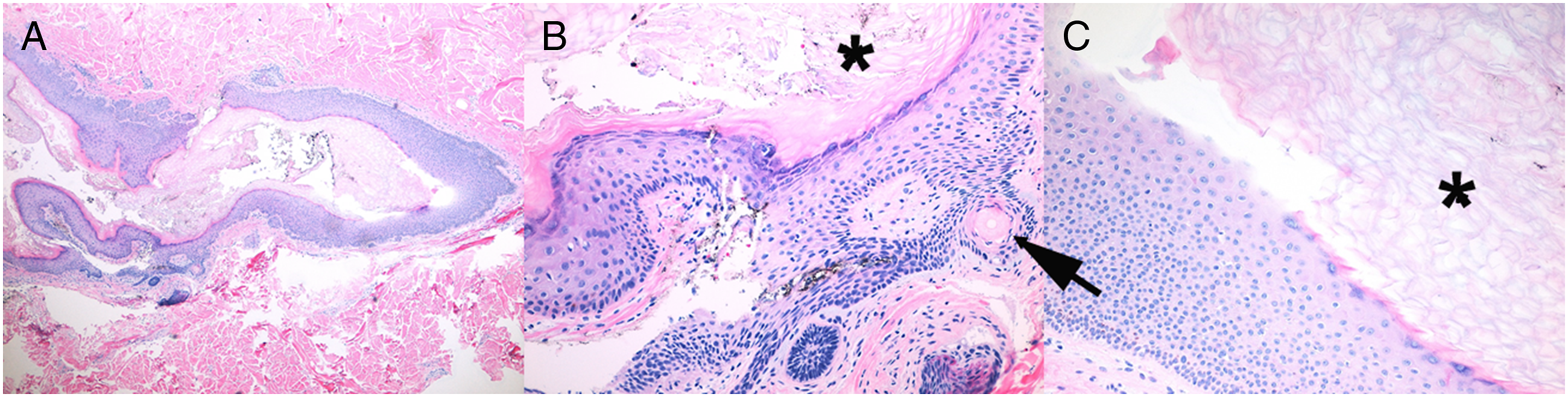
Epidermal cysts (epidermoid cysts or epidermal inclusion cysts) are common benign intradermal or subcutaneous cysts commonly presenting on the scalp, face, neck, trunk, and extremities.14,15 They are smooth, dome-shaped, spherical, unilocular swellings varying in size from a few millimeters to a few centimeters and usually present with a central punctum (Figure 6). Microscopically, these cysts are lined by an epidermis-like epithelium including a granular cell layer containing laminated keratin (Figure 7). Epidermal cysts are usually asymptomatic; however, if a cyst ruptures, its content are released into the dermis causing a foreign body reaction. Numerous multinucleated giant cells form keratin granulomas, causing pain and swelling.16,17 If multiple cysts are present, associated syndromes such as Gardner syndrome, pachyonychia congenita, and Lowe syndrome should be considered.
18
When partially calcified, these lesions may mimic pilomatrixoma on physical and ultrasound examination.
19
Symptomatic cysts are treated by surgical excision including the hair follicle of origin. (A) Teenage patient with inflamed cyst of hair follicle origin (black arrows outline subcutaneous cyst, large arrow indicates follicle of origin) (B). H&E section of epidermal cyst showing a connection to the skin surface (20x). (A) Low power view of epidermal cyst in the dermis (40x), (B–C) The cyst is lined by a stratified squamous epithelium with a granular layer, contains abundant keratin flakes (asterisk), and appears to be arising from a hair follicle (adjacent cross section of hair by arrow) (200x).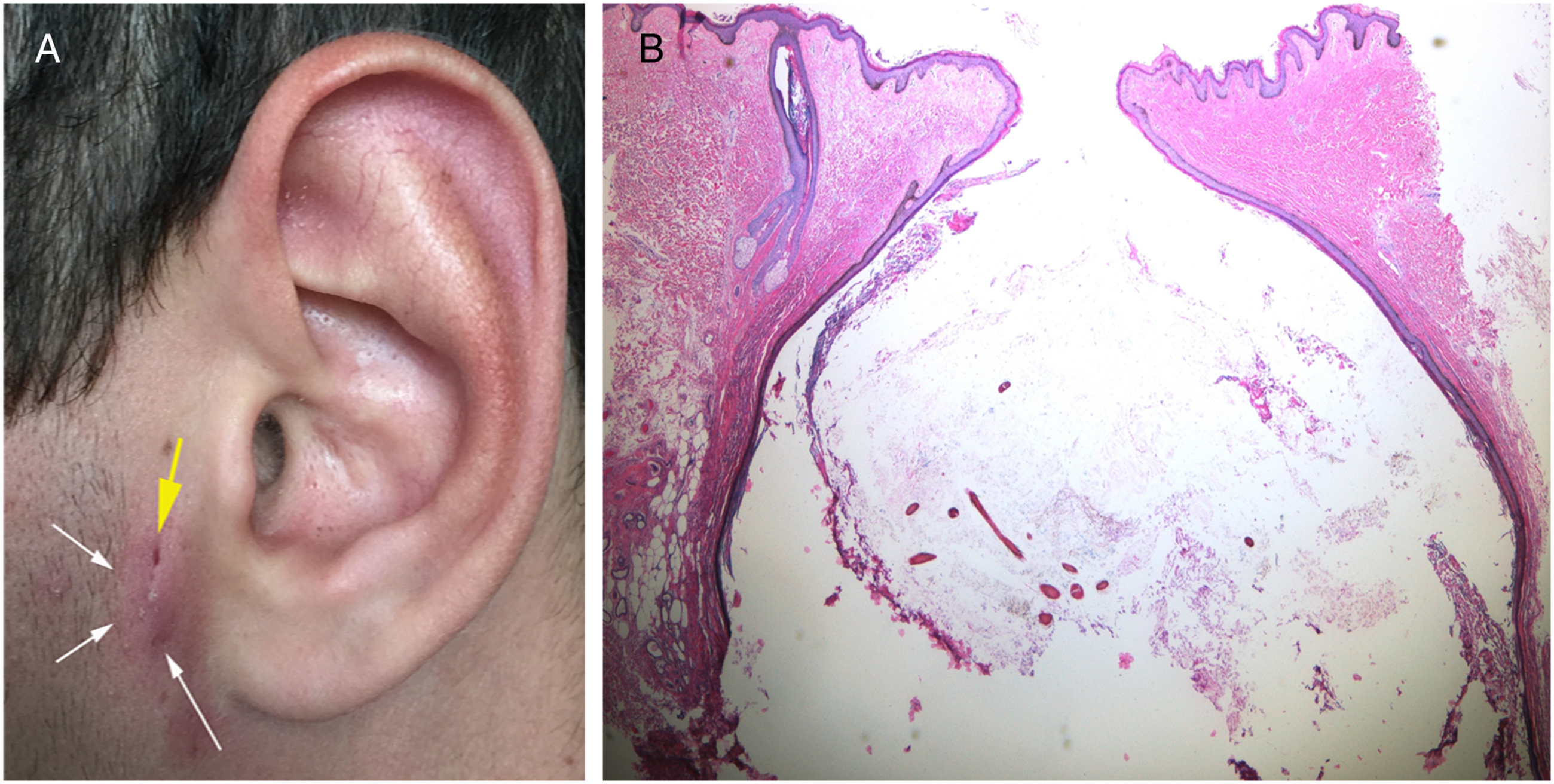
Trichilemmal Cysts
Trichilemmal cysts20,21 are nodular cystic lesions derived from the isthmus of the hair follicle. They can be solitary or multiple intradermal or subcutaneous lesions, mainly located on the scalp. They may be sporadic or follow autosomal dominant inheritance.
22
Their clinical presentation is similar to that of epidermal inclusion cysts and pilomatrixomas - firm, mobile, and nontender. The trichilemmal cysts are lined by stratified squamous epithelium, generally without a granular layer (Figure 8). Foci of calcification occur within the cyst lumen in about 25% of cases. When calcified, trichilemmal cysts may be difficult to differentiate from pilomatrixomas clinically or by ultrasonography.23,24 Complete surgical excision including the hair follicle of origin is the treatment of choice for symptomatic trichilemmal cysts. (A) Low power view of trichilemmal cyst, with stratified squamous epithelial lining at the periphery (bottom), central dense laminated eosinophilic keratin, and calcifications (arrow), (B) High power view of stratified squamous epithelial cyst lining showing an absent granular layer (asterisk) (200x).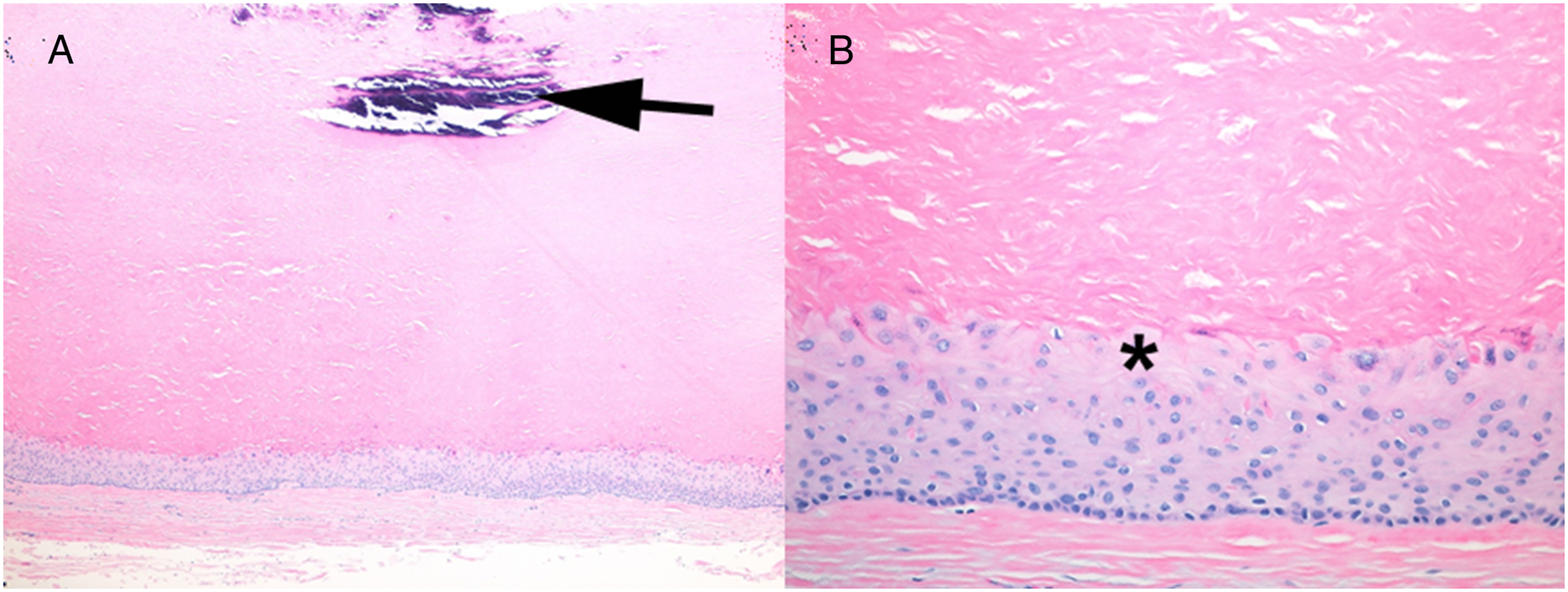
Molluscum Contagiosum
The molluscum contagiosum virus is a doubled stranded DNA poxvirus that infects the skin, resulting in the formation of molluscum lesions. 25 Molluscum contagiosum is most often seen in children and young adults, and incidence typically peaks between 1-4 years old. 26 On physical exam, these dome-shaped lesions are small, shiny, and flesh-colored. 27 Molluscum lesion are classically umbilicated with a white central core. They average is 1–5 mm in diameter. 28
Giant molluscum contagiosum is a rare nodular variant of molluscum contagiosum.29,30 As the lesions display central umbilication they may appear similar to pilomatrixomas, though they are softer and more symmetric (Figure 2). These lesions are rare in healthy children and more often are found in settings of altered immunity, such as atopic dermatitis, corticosteroid and immunosuppressive therapy, leukemias, and HIV infection.31,32 On light microscopy, giant molluscum lesions resemble epidermoid cysts with a lining of keratinizing stratified squamous epithelium. Typical molluscum bodies are found in the cyst wall.
33
(Figure 9). (A) Low power H&E photomicrograph of giant molluscum contagiosum lesion, (B) Arrow shows the nucleus of an epidermal cell, pushed to the periphery as molluscum bodies fill the cytoplasm. These molluscum bodies are present at the umbilicated core of the lesion.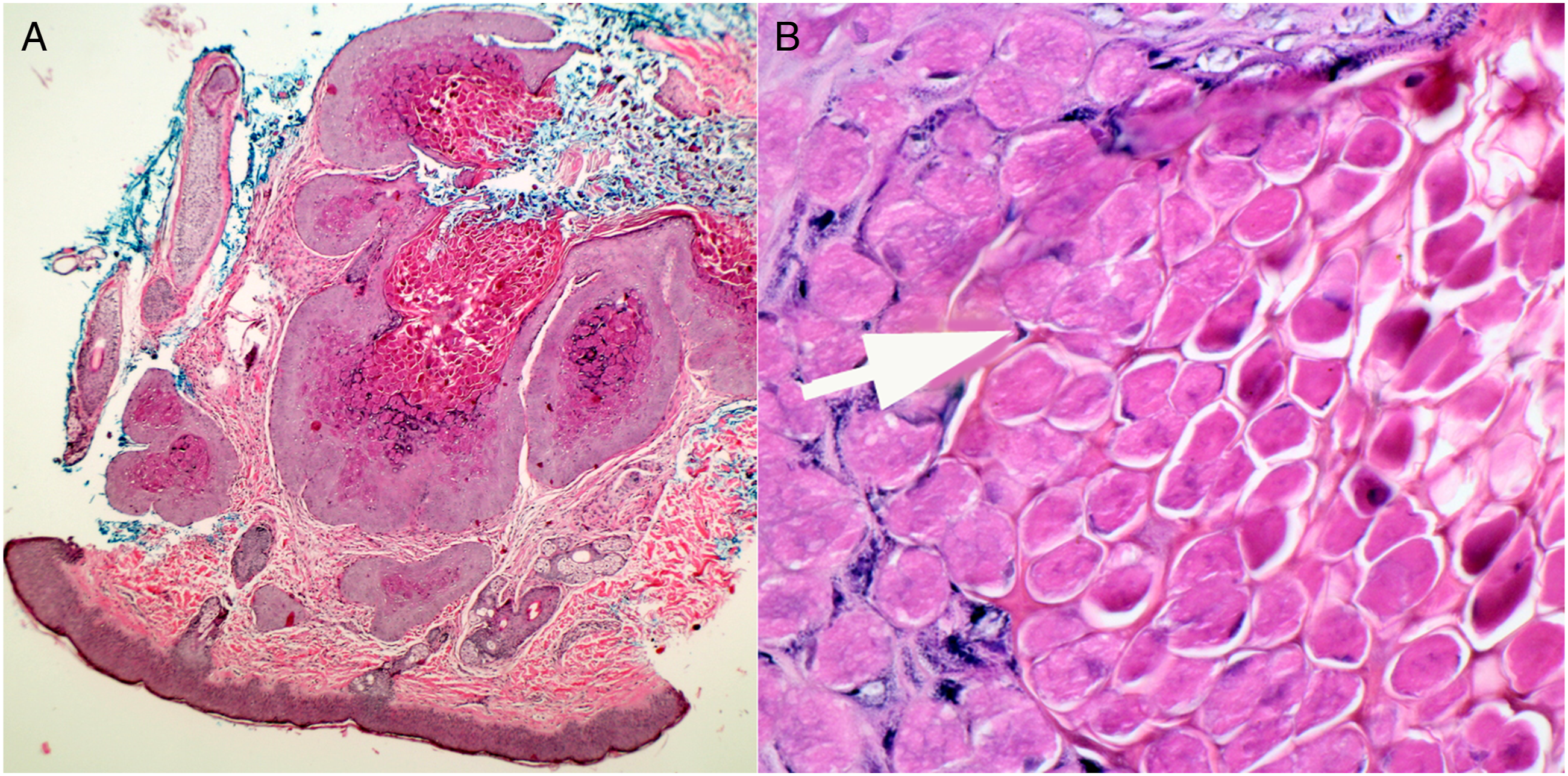
We encountered no description of the ultrasound appearance of giant molluscum lesions in our literature review. Diagnosis of giant molluscum contagiosum lesions requires excision and histopathologic examination.
To Image or Not to Image
In their 2016 systematic review of pilomatrixomas in children, Schwarz et al 1 include an algorithm for suspected pilomatrixoma with classic history and physical features. They recommend surgical excision without prior imaging for typical lesions. For atypical presentations, preoperative ultrasound confirmation was suggested. Fine needle aspiration was reserved for lesions that lacked classic features and where ultrasound was nondiagnostic. The effectiveness of this algorithm has not been tested.
High-frequency ultrasound has become the technology of choice for evaluating small lesions of the skin and subcutaneous tissue. Ultrasound of benign subcutaneous lesions usually demonstrates characteristic findings enabling a specific diagnosis. 34 Unfortunately, in the case of pilomatrixomas, the variable morphology of the cystic component and the incomplete calcification of early-stage lesions makes ultrasound less reliable. In a large series of histologically confirmed pilomatrixomas, preoperative ultrasound was diagnostic in only 15% (9/59) of suspected tumors. While 37 of these lesions had typical ultrasound features, 22 lesions (37%) were not calcified. Among the noncalcified lesions, 10 were hypoechoic, and 12 had a cystic appearance. 35 This calls into question ultrasound’s utility in the work-up of suspected pilomatrixomas.
Among the 19 lesions we studied, 18 (16 pilomatrixomas, 1 epidermal inclusion cyst and 1 ruptured trichilemmal cyst) required the same treatment for cure—complete excision in continuity with the hair follicle of origin. While molluscum contagiosum lesions may resolve spontaneously or with treatment of underlying immunodeficiency, the natural history of giant cystic molluscum contagiosum lesions is unknown, as all reported cases have been treated surgically.
Conclusion
Our results and literature review support the concept of complete surgical excision of suspected pilomatrixomas without prior imaging in most cases. For children at increased risk from surgery or general anesthesia, or when families desire greater preoperative certainty, high-resolution ultrasound examination may be useful, especially for typical lesions.
Footnotes
Acknowledgments
The authors wish to thank Nancy Tsui for her artistic contribution to figure 5.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.