
Abstract
The clinicopathologic features of thyroglossal duct cyst when it develops ectopically in the thyroid gland remain unclear because of its rarity, which makes diagnosis difficult. Clinical diagnosis and treatment should not disregard the possibility of thyroglossal cysts located in the thyroid gland. We here report the current case to prepare others and provide data for the diagnosis and treatment of this kind of disease.
Background
Thyroglossal duct cyst (TGDC) is one of the most common neck swellings seen in clinical settings. The most useful clue visible in imaging is a midline cystic neck mass embedded in infrahyoid strap muscles, called “claw sign.” Most of the patients have no obvious symptoms and are often found by chance. If they have secondary infection, they may have pain along with swelling. TGDC diagnoses usually require a combination of ultrasound and fine needle aspiration (FNA). Thyroglossal duct cyst treatment does well with a modified Sistrunk procedure incorporating central lymph node dissection. Although they are closely related to the thyroid anatomically, intra-thyroid extension is very rare. Some patients have no visible symptoms.
Introduction
Thyroglossal duct cyst is a common congenital malformation located at the neck. 1,2 Thyroglossal duct cyst usually appears at the same position and shows the same structure. The primordium of the thyroid gland is combined with the tongue by a narrow tubular structure called the thyroglossal duct, the site of whose connection with the epithelial floor of the mouth is signified by the foramen caecum intra-thyroid TGDC. However, few cases of intra-thyroid TGDC have been reported in the literature. 2,3 Thyroglossal duct cyst diagnosis relies on the combination of ultrasound and FNA. However, clinical diagnosis and treatment do not just rely on auxiliary examination. This time, we report a case about TGDC located in the thyroid gland that was misdiagnosed with thyroid carcinoma.
Case Presentation
A 65-year-old man initially presented with an incidental asymptomatic 0.9-cm thyroid goiter in 2020. The patient did not exhibit any significant findings upon physical examination. The results of laboratory analysis, including alpha-fetoprotein, carcinoembryonic antigen, cancer antigen 19-9, cancer antigen 125, cancer antigen 724, cancer antigen 50, and cancer antigen 242, were within normal ranges. Ultrasound suggested that the goiter might be a thyroid carcinoma (Figure 1). A computed tomography (CT) scan revealed a 0.9-cm mass in the right thyroid gland (Figure 2). Fine needle aspiration shows well-differentiated squamous cells (Figure 3). Based on the aforementioned findings, the preoperative diagnosis was still more suggestive of a thyroid carcinoma. In surgery, the right thyroid gland was found to be about 4 × 4 × 2 cm3 in size. A cystic nodule was found in the thyroid tissue with a diameter of about 1 cm. These clumps were hard in texture and had clear boundaries, but there was no thyroglossal duct tract noted. Examination of the frozen section showed that the patient was treated with thyroidectomy plus lymph node dissection. Pathological histology: To the naked eye: thyroid tissue 6 × 2 × 1 cm3, cut to see a cystic nod diameter of about 0.5 cm, thin sac wall, with a small amount of translucent liquid in the sac. A hard, white area was also visible. Pathological diagnosis: “Right leaf of the thyroid gland and gorges” nodular goiter (NG), in which a cyst was visible. The cyst wall was covered by squamous cells. A TGDC accompanied the NGs (Figure 4). Details are presented in Table 1. Until June 04, 2021, the patient has a good diet and sleep well with a normal thyroid function.
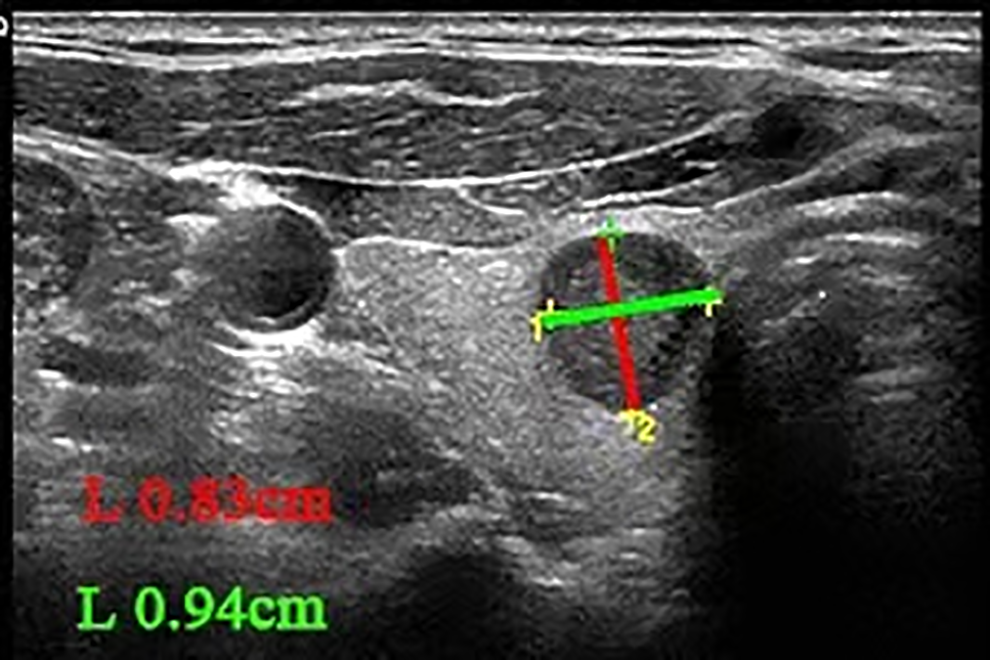
Ultrasound: the low echo size of about 0.94 × 0.83 cm was found under the right leaf of the thyroid gland, the morphological rules, the boundary was clear, and no significant calcification was seen inside, and the rear echo did not change significantly. CDFI shows no obvious blood flow signal. Low echo of the right-hand leaf of the thyroid gland; type TI-RADS4B.
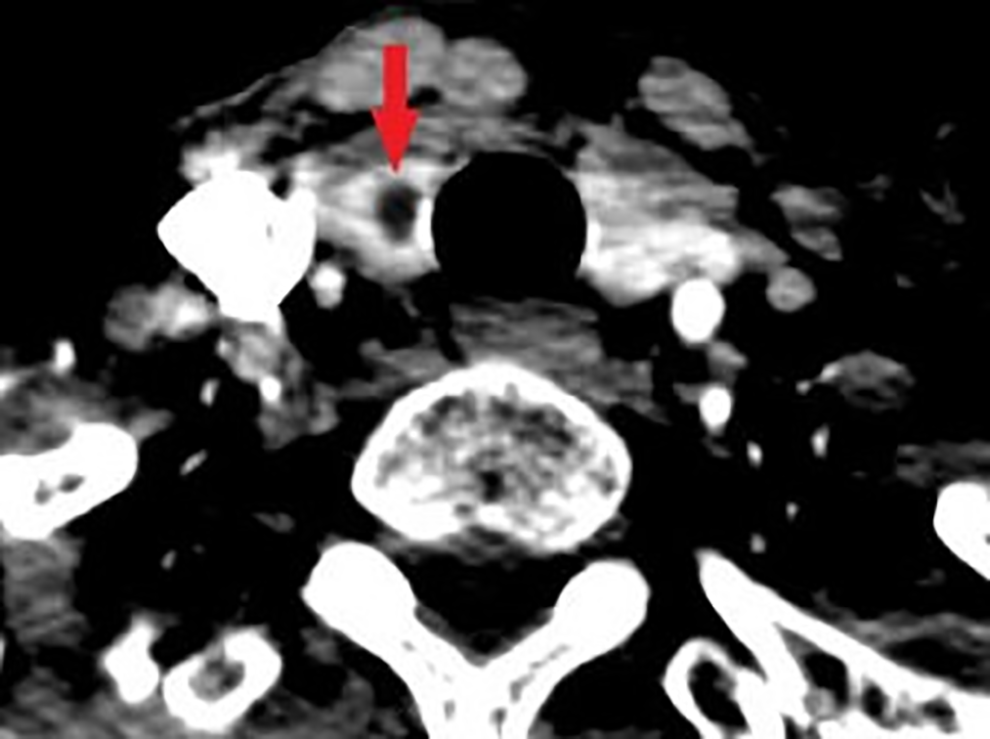
November 17, 2020: Neck chest enhancement computed tomography (CT):1, thyroid right leaf cyst may be.
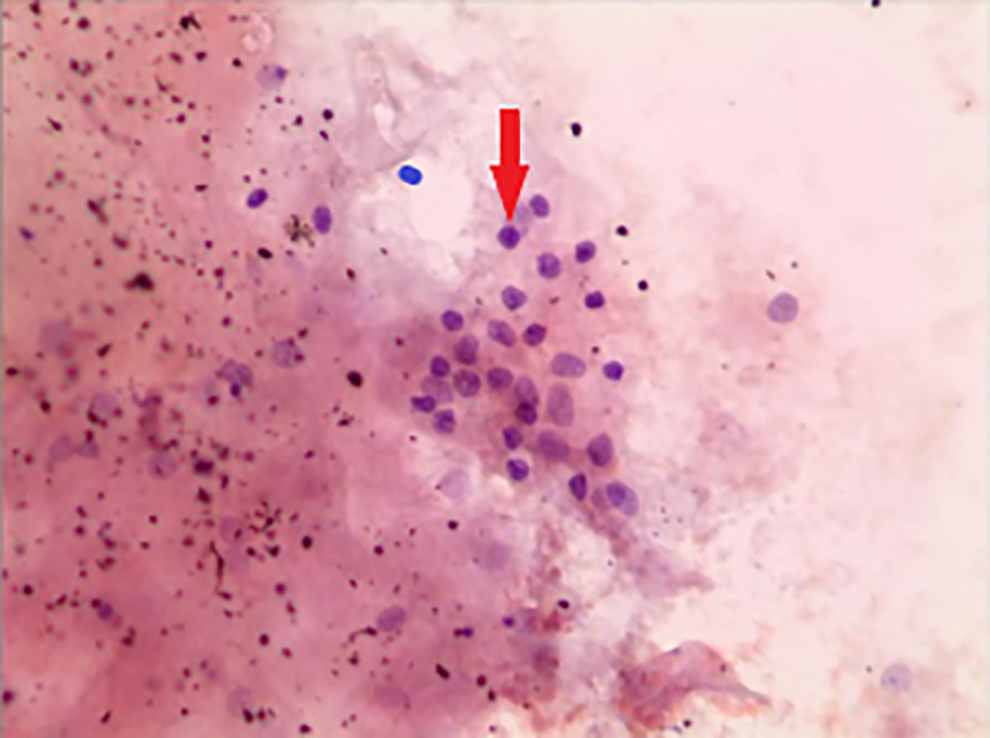
November 18, 2020: Fine needle puncture cytology: more scaly, epithelial cell a small number of glial and tumor-like growth of thyroid epithelial cell.
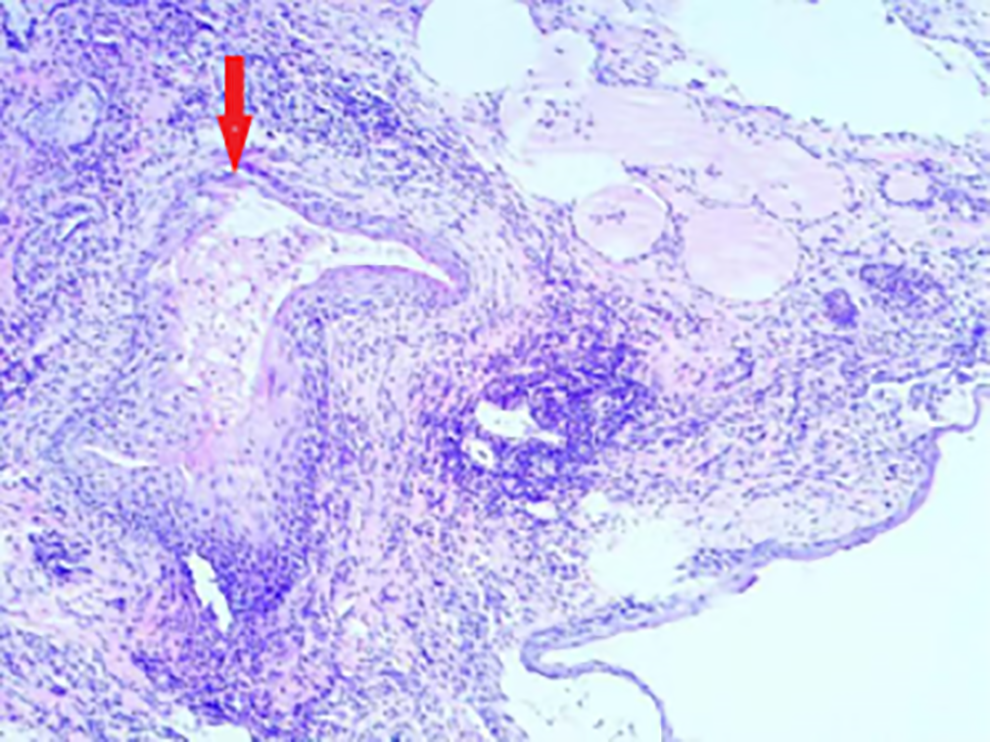
The right leaf of the thyroid gland and the gorge: “right leaf of the thyroid gland and gorges” nodding goiter, during which a cyst is seen, the cyst wall is squamous epithelium except for the mycelium cyst may be.
Auxiliary Examination.
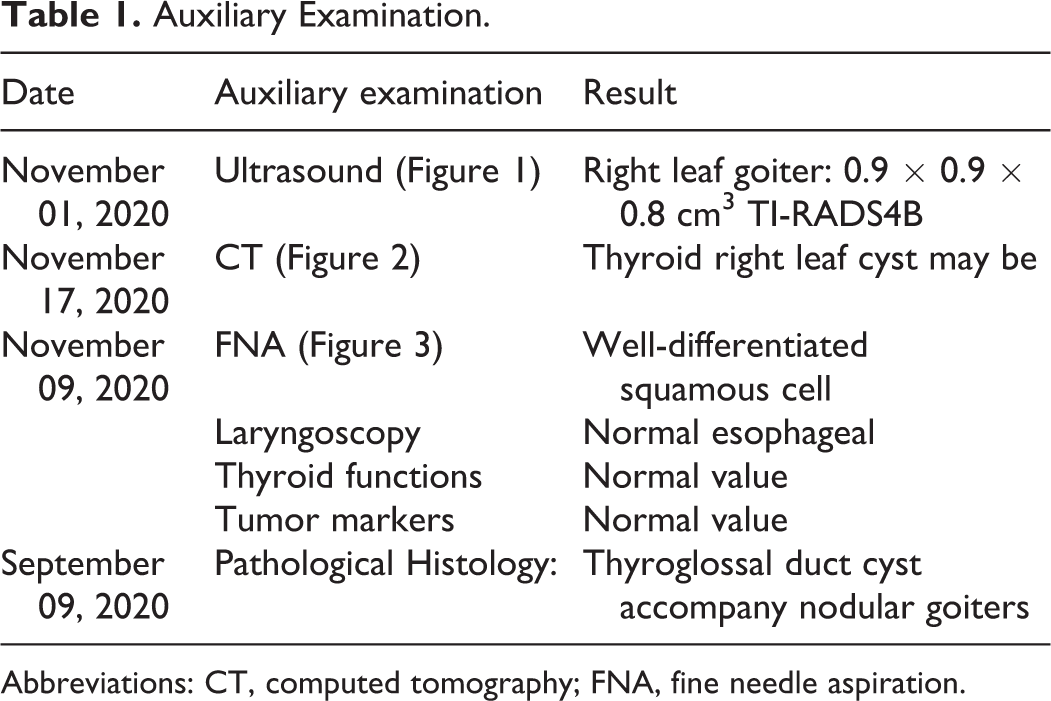
Abbreviations: CT, computed tomography; FNA, fine needle aspiration.
Discussion
Thyroglossal duct cyst is a common congenital malformation located at the neck, typically occurring in children. To our knowledge, there may be extremely rare case reports of intrathyroidal TDGC in adults in China. 3,4 It often appears as an asymptomatic mass that moves up and down while swallowing. 5 The most useful clue visible in imaging is a midline cystic neck mass embedded in infrahyoid strap muscles, called “claw sign.” Thyroglossal duct cyst is benign in appearance, though the cystic neck mass and wall may worsen if infected. Location is important to diagnosis. Ultrasound is mainly evaluated in the following ways: localization, appearance, internal echo, septate status, capsule wall, and post enhancement. 3,6 Histologically, TGDCs are composed of squamous cells. 7 Here, a 65-year-old patient was admitted to the hospital for treatment of thyroid nodes. Fine needle aspiration results showed good differentiation of squamous cells. Cranial CT, gastroscopy, neck chest enhancement CT, and tumor markers were used to exclude the primary pathogenesis from the lungs, stomach, esophagus, brain, and other major organs. We performed FNA twice to reduce the risk of puncture and the possibility of mistaken puncture as the esophagus. According to the patient’s medical history and results of auxiliary examination, the risk of thyroid malignancy was considered high. The patient underwent a thyroidectomy plus lymph node dissection. During surgery, we found a solitary nodule growing in the thyroid gland, but no thyroglossal duct tract was found. Histological examination of samples collected during surgery showed the following: the right lobe of the thyroid gland and the gorge had benign lesions. The central area lymph nodes had granuloma at 24 sites. We thought it was not necessary to expand the scope of surgery. The patient’s pathological histology results showed a TGDC accompanying NGs. However, before the operation, this goiter was diagnosed with thyroid cancer, based on the ultrasound and FNA.
As the detection rate increases, unnecessary thyroid surgery rates have also increased. Fine needle aspiration is the most reliable initial method for diagnosing thyroid nodules, as mentioned in the 2014 ATA guidelines. However, although this method has obvious advantages as a diagnostic tool, the damage caused by FNA can alter tissue histology and foster diagnostic misinterpretations. 8 Fine needle aspiration does not accurately distinguish follicular adenoma from well-differentiated follicular carcinoma or hyperplastic nodules in the NG. 7 Moreover, the possibility of a nodule developing into a TGDC carcinoma is less than 1%. The vast majority of TGDC carcinomas are papillary carcinomas, and only a small number of TGDC carcinomas are squamous cell or follicular carcinomas. Thyroglossal duct cysts have walls composed of alternating nonkeratinizing stratified squamous epithelium and respiratory epithelium. 2 In this case, both the FAN reports of the patient showed well-differentiated squamous cells. The origin of squamous cells is unclear. They may have come from the TGDC hydatid fluid or they could have come from squamous cell metaplasia in the thyroid tissue. Also, it could have been diagnostic misinterpretations of FNA results.
The term “nodular thyroid disease” refers to a thyroid gland occupied by nodules, including one or more goiters. These can be palpable or imperceptible. 9,10 In addition to local symptoms, such as any other occupying tumors in the upper suprasternal fossa area, and the possibility of developing subclinical or overt thyrotoxicosis, nontoxic diffuse goiter does not have extrathyroidal symptoms, such as ophthalmopathy in Graves’ disease. 10 Nodular goiters are associated with a lack of iodine, natural tendency toward goiter, elevated levels of thyroid-stimulating hormone, iron and selenium deficiency, or smoking. 11 It can be further subdivided into toxic and nontoxic goiters. 8 In this case, the patient was diagnosed with TGDC accompanied by NG. He had normal thyroid function and ate a healthy balanced diet before he was diagnosed with this disease. However, he had no family history of any disease as this. He said he had no history of exposure to radioactivity. Etiological factors need to be explored.
Thyroglossal duct cyst treatment preferred a modified Sistrunk procedure. The Sistrunk procedure should be added to the repertoire of central lymph node dissection techniques. 12,13 The surgical option that is best suited for NGs remains unclear, that is, for patients with different conditions, the choice of surgical method may also be different. Patients with especially large goiters or retrosternal NG may be best served by total thyroidectomy. However, for unilateral NG, subtotal thyroidectomy is better. In this case, the patient had both TDGC and NGs. Nontypical TDGC is considered an affliction of the thyroid gland. 9 The nontypical TGDC structure during the surgical process and the frozen sections showed both the thyroid gland and the central lymph nodes to be benign lesions. Based on all the auxiliary examinations and medical history, the treatment suggested was subtotal thyroidectomy plus central lymph node dissection.
Conclusion
In this case, we report a 65-year-old man with the chief complaint of an asymptomatic 0.9-cm thyroid goiter. Ultrasound and FNA suggested that the goiter may have developed from the thyroid. However, we used pathological histology to make our final diagnosis: TGDC accompanied by NG. Had this patient been treated with a more accurate technique, his disease might not have been misdiagnosed with thyroid carcinoma before surgery. Despite the rarity of intrathyroidal TGDC and the lack of features characteristic of benign lesions, the diagnostic pitfall was avoided in the case of this intrathyroidal TGDC lesion due to the limited medical technology and our rigid ideas. Generally, the diagnosis and treatment of such cases are few; so, summaries are very important. This case also reminds us that if we encounter such cases in future, although there are other sources of tumors, we should start from a conventional point of view and not disregard the most basic and simple possibilities. The diagnosis and treatment of TGDC remain controversial, neither FNA nor frozen sections are absolute. With the advancement of medical technology, more and more methods and equipment are being invented and discovered. We expect the clinical diagnosis and treatment of this disease to improve along with them.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.