
Abstract
Objective:
Coronavirus disease 2019 (COVID-19), caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection, can result in persistent loss of taste and smell. This study was performed to assess acoustic reflex threshold (ART) in patients with taste disorders caused by SARS-CoV-2.
Material and Methods:
This retrospective study enrolled 11 patients (9 men, 2 women; average age = 22.3 years) with a history of COVID-19 and had complaints of taste disorder and sensitivity to loud sounds. The control group consisted of 13 healthy participants (10 men, 3 women; average age = 23.4 years). Anamnesis, neuro-otological, ear, nose and throat, and eye examinations, as well as a taste test, pure tone audiometry, speech discrimination test, and impedance audiometry were performed in all participants.
Results:
All participants in the study group had a negative taste test result. In addition, ART values were significantly higher in the study group than the control group at all frequencies.
Conclusions:
SARS-CoV-2 could be a neurotropic virus that can cause facial nerve neuropathy.
Introduction
More than 100 million cases, including 2 million deaths, of coronavirus disease 2019 (COVID-19) caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) have been recorded worldwide in the last year. 1 This pandemic has been responsible for many health, social, and economic problems worldwide. Common symptoms of COVID-19 infection include fever, cough, dyspnea, malaise, muscle and joint pain, headache, nausea, vomiting, and diarrhea. However, unlike usual upper respiratory viral infections, COVID-19 can be associated with long-lasting anosmia and taste disorders. 2 Many viral infections cause hearing impairment. Neurosensory hearing disorders have been reported to be due to effects on the organ of Corti, brainstem/temporal lobe involvement, and perfusion disorder.3-5 Recent studies also reported hearing loss is cases of COVID-19, but the underlying mechanism is not clear. SARS-CoV-2 has been reported to cause olfactory and gustatory dysfunction, cranial neuropathies, and hearing impairment.4,6-8 Recent studies have shown that SARS-CoV-2 infection can also cause peripheral facial palsy. 9 However, there have been no previous studies on the involvement of the stapedial nerve, which is a branch of the facial nerve, in COVID-19.
Some patients who had COVID-19 in the last year and complained of taste disorder were found to be especially disturbed by loud sounds. It is thought that this patient group may have facial neuropathy originating from the distal of greater petrosal nerve. This can cause discomfort from loud noise (because of stapedial neuropathy) and taste disorder (because of chorda tympani neuropathy). This study examined the acoustic reflex thresholds (ART) of COVID-19 patients with taste disorders who also reported being disturbed by loud sounds and compared the obtained results with a healthy group. The goal was to determine whether there was impairment of the stapedial nerve.
Material and Methods
This study was carried out after the patients were diagnosed with COVID-19 in 14th and 40th days. Eleven patients with a history of COVID-19 but no signs of active viral infection were seen at the otorhinolaryngology clinics of the Istanbul Yeni Yüzyıl Hospital Faculty of Medicine and Bahat Hospital between June and December 2020. The age range of participants (study and control groups) was between 19 and 27 years. Patients with hearing impairment and/or facial paralysis were excluded from the study. The study group consisted of 11 patients (9 men, 2 women; average age = 22.3 years) with complaints of taste disorder and sensitivity to loud sounds. The control group consisted of 13 healthy participants (10 men, 3 women; average age = 23.4 years). The control group was selected from people with age and gender characteristics similar to the study group whose routine ENT examination was natural, who had no health problems and no hearing thresholds above 10 dB HL. Polymerase chain reaction test was negative for SARS-CoV-2 in this group.
Detailed medical history, ear, nose, and throat (ENT), eye examinations, along with a taste test, pure tone audiometry, speech discrimination test, and impedance audiometry were performed in all participants. The solution-based taste test was applied in all participants: 0.1 g/mL sucrose solution was used for sweet taste, 0.1 mL of citric acid for sour taste, 0.15 mL of NaCl solution for salty taste, and 0.1 g/mL caffeine solution for bitter taste.10,11
Audiological examinations were performed by a specialist in the audiology center of our clinic using a clinical high-frequency audiometer (R37A-HF; Resonance) and clinical high-frequency tympanometry device (R36M-PT; Resonance) (Figure 1).
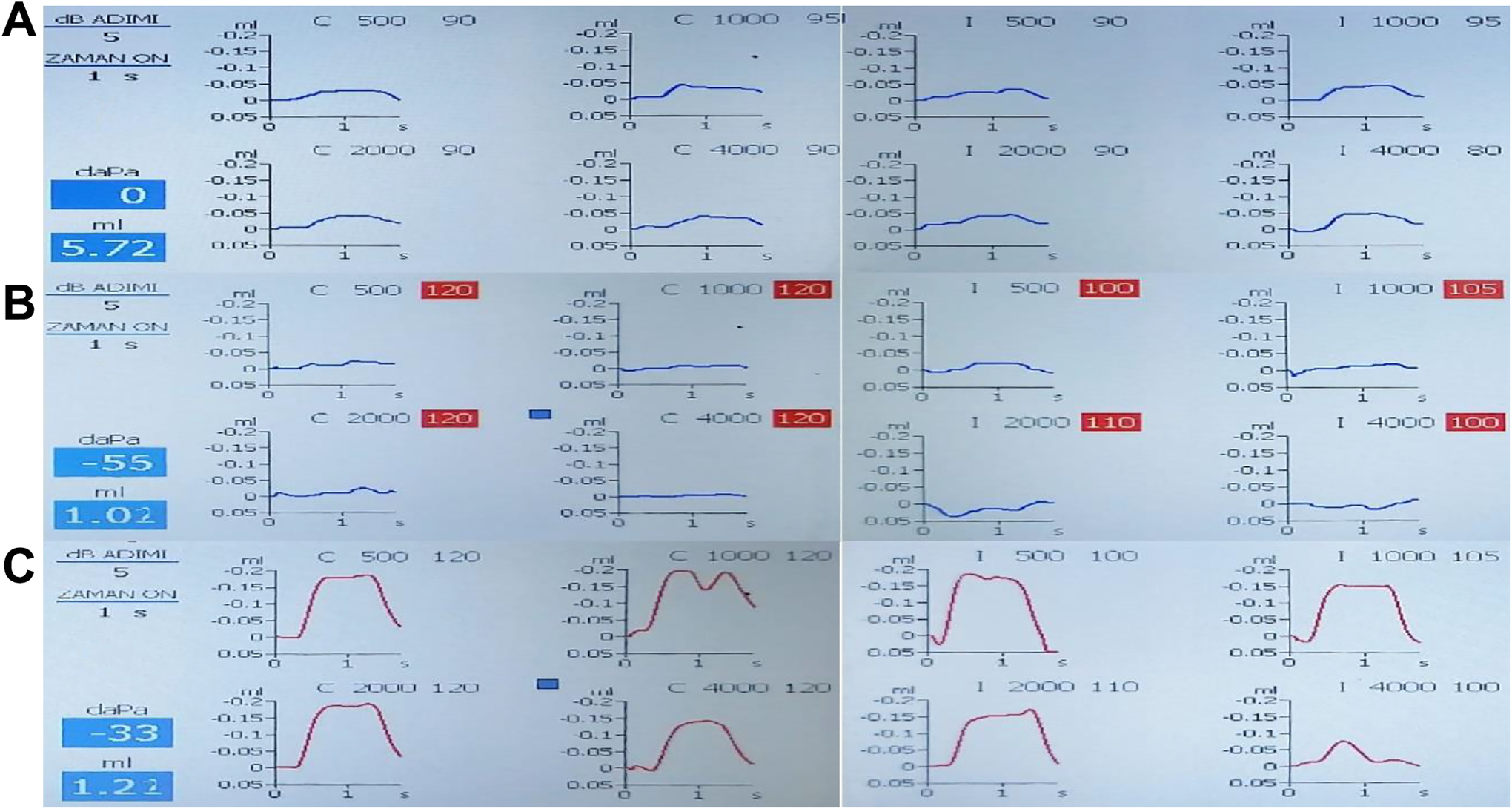
Acoustic reflexs threshold (ART) (A) control group, (B) study group (in 14th day after diagnosed with COVID-19), (C) study group (in 40th day after diagnosed with COVID-19). Stimulation frequency: 226 Hz: 85dB SPL ± 2dB, 678, 800 and 1000 Hz: 75dB SPL ± 2dB; frequency accuracy: ± 0.5%; harmonic distortion: less then 1%; reflex test method: threshold, automatic, manual; stimulus duration: 0, 5, 1, or 2 sec. Ipsilateral and contralateral stimulation for all reflex test.
Acoustic reflexes (AR) were evaluated ipsilateraly for each ear, as all but 2 patients (1 male, 1 female) in the study group showed sensitivity to loud sounds in the bilateral ears. Therefore, the study and control groups consisted of 20 and 26 ears, respectively.
This study was approved by the Ethics Committee for Non-Invasive Health Sciences Research of Istanbul Yeni Yüzyıl University (Date: 01.11.2020 and Decision No: 2021/01-555).
Statistical Analysis
The Mann-Whitney U test was used to compare groups, and was performed using SPSS software (version 20.0; SPSS Inc). Acoustic reflex threshold calculations were performed in accordance with the ipsilateral reflex values of the 2 groups. The P-value significance was P <.005.
Results
Table 1 provides the average acoustic reflex threshold values for all participants at 500, 1000, 2000, and 4000 Hz. Table 2 provides the average acoustic reflex threshold values for the study (in 40th day after diagnosed with COVID-19) and control groups. There were statistical significant differences between the 2 groups at all frequencies (P = .001).
Average Acoustic Reflex Threshold Values for All Participants.
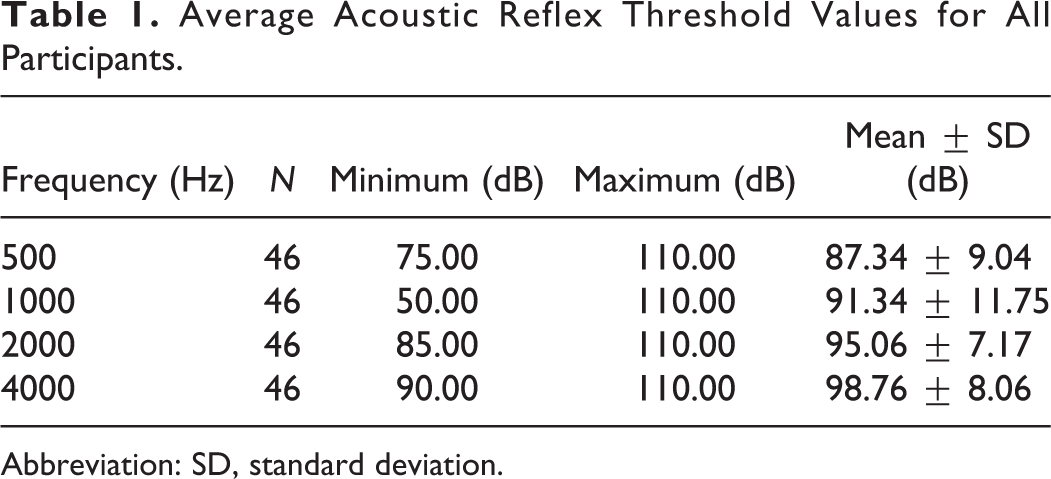
Abbreviation: SD, standard deviation.
Average Acoustic Reflex Threshold Values for the Study (40th Day After Diagnosed With COVID-19) and Control Groups.
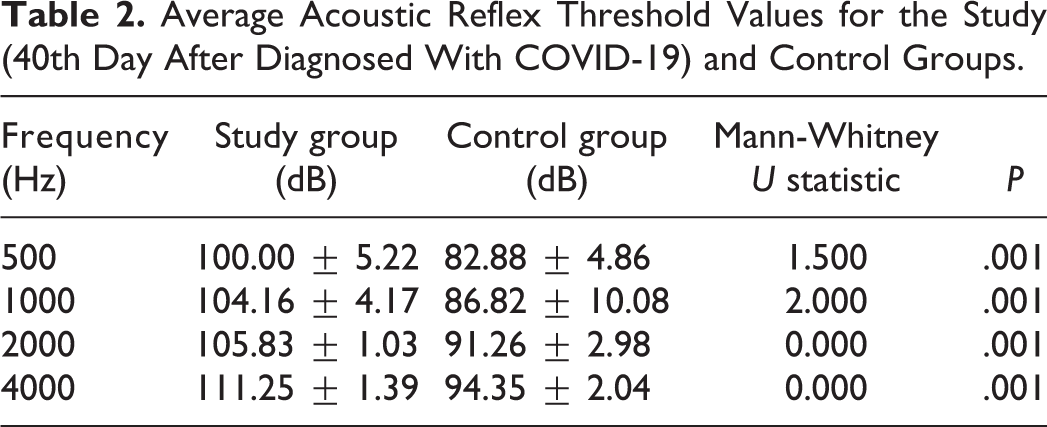
The values were higher for the study group at all frequencies. No participant in either group exhibited hearing loss or facial paralysis according to anamnesis and ENT examinations. In the 250, 500, 1000, 2000, 4000, and 8000 Hz high-frequency audiometry tests, the hearing levels were better than 10 dB, and there were no significant differences between the study and control groups. Speech discrimination (SD) tests were performed to check for retrocochlear pathology, and the discrimination ability was 100% bilaterally in both groups. The AR, which was assessed by impedance audiometry at 500, 1000, 2000, and 4000 Hz, was ipsilaterally present in both groups. But ART values were significantly higher in the study group (in 40th day after diagnosed with COVID-19) than the control group at all frequencies (Table 2).
During eye examinations and Schimer’s test, no symptoms of eye dryness were detected in the study and control group. The solution-based taste test was normal in the control group but the test indicated abnormalities in the study group.
Discussion
Herpes simplex virus 1, varicella zoster virus, and Borrelia burgdorferi are the main infectious agents responsible for facial palsy. 12 The rapid spread of the COVID-19 pandemic has facilitated examination of neurological symptoms in large numbers of SARS-CoV-2 patients. The results of the present study showed that SARS-CoV-2 infection could affect the stapedial nerve.
Goh et al reported that facial paralysis due to SARS-CoV-2 infection can be unilateral or bilateral. 9 Helbok et al reported bilateral facial palsy associated with SARS-CoV-2 infection via a mechanism similar to Guillain-Barré syndrome. 13 Another study reported that the facial nerve is affected mostly in younger people. 14 The high ART of the patients with loss of taste suggests minimal effect of COVID-19 on the facial nerve in these cases.
The mechanism by which SARS-CoV-2 induces facial neuropathy is not yet clear. However, some studies reported that SARS-CoV-2 has neurotrophic effects 14 and damages the facial nerve via activation of the immune response. 15 Idiopathic facial nerve paralysis associated with the inflammatory response may involve vasa nervorum ischemia and demyelination. 16
We initially predicted the effect to be ipsilateral absent AR in 75 to 85 dBs in the study group in 14th day after diagnosed with COVID-19 (in these levels present AR in control group), but the study group showed present AR in 100 to 120 dBs in 40th day after diagnosed with COVID-19 in the present study. However, we observed a significant increased ART in these cases. Retrocochlear pathology was checked for using SD tests. Previous studies showed present AR on the side with facial paralysis, especially during nerve regeneration, along with a higher ART. Such results have generally been reported in cases exhibiting lesions proximal to the stapedial nerve.17-19 In such cases, the chorda tympani nerve may also be affected, which may explain the taste disorders seen in our study group. However, as this was a preliminary investigation, further studies including larger populations and more advanced stages of facial nerve involvement, such as electrogustometry tests and nerve excitability tests, along with magnetic resonance imaging, are required.
Normally, AR works at a sound volume of about 80 dB and protects the inner ear from noise, but in this study, it was seen that AR occurs at 100 to 120 dB values due to facial and stapedial neuropathy. This explains the discomfort from loud noise in high ART values.
This study suggested that SARS-CoV-2 infection may affect the facial nerve, especially the sapedial nerve and chorda tympani nerve, and patients may experience loss of taste and sensitivity to loud sounds.
Footnotes
Acknowledgments
The authors would like to thank the chief physician of Bahat Hospital, Dr Hamza Bahat, as well as Yeni Yuzyil University, and the Department of ENT of Istanbul University.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.