
Abstract
Post-vaccine olfactory and gustatory disorders are very rare and were reported in patients who received influenza vaccines. In this article, we report 6 cases of post-coronavirus disease 2019 (COVID-19) vaccine olfactory and gustatory disorders in patients with negative nasal swabs. Precisely, olfactory and gustatory dysfunctions were reported in 5 and 1 patients, respectively. Sense disorders occurred after the first injection of AstraZeneca (n = 4) or the second injection of Pfizer (n = 2) vaccines. In 4 cases, the olfactory or gustatory disorder was confirmed with psychophysical evaluations. The duration of chemosensory dysfunction ranged from 4 to 42 days. None of the patient reported mid- or long-term olfactory or gustatory disorder. The occurrence of olfactory and gustatory dysfunctions in adults benefiting from COVID-19 vaccines is still rare but has to be known by otolaryngologists.
Introduction
Coronavirus disease 2019 (COVID-19) is a worldwide infection that led to more than 3 500 000 deaths as of May 28, 2021. 1 To date, 1 545 967 545 vaccine doses have been administered. 1 The various vaccines were demonstrated as safe and protective against the virus, 2,3 but as all vaccines, they may have adverse effects related to known and unknown mechanisms. In this article, we retrospectively reported several cases of patients developing olfactory or gustatory disorders after the administration of anti-COVID-19 vaccine.
Patients and Methods
We reviewed patients who presented with post-vaccine smell or taste disorders in 5 European hospitals (Sassari University Hospital, Italy; Ferrara University, Italy; Foch Hospital of Paris, France; CHU Brugmann and CHU Saint-Pierre, Brussels, Belgium). To be included, patients had to present self-reported loss of smell or taste within the days following the administration of COVID-19 vaccine and negative COVID-19 reverse transcription-polymerase chain reaction (RT-PCR). We did not include patients with history of COVID-19 throughout the 6 months preceding the vaccination. Taste dysfunction was defined as impairment of salty, sweet, bitter, or sour perception. 4 The epidemiological and clinical features of patients were reviewed. Because the design of the study, the institutional review board was not necessary to report these cases.
Results
The retrospective chart review included 6 patients (5 females). Patient age ranged from 25 to 50 years old. The epidemiological and clinical data are available in Table 1. The most implicated vaccine was AstraZeneca (first injection; Astra AB Zeneca), while 2 patients reported sense impairments post-Pfizer vaccine (second injection; Pfizer Inc). Two patients self-reported hyposmia, while 2 others reported anosmia. One patient reported parosmia. The last one complained of dysgeusia without smell disorder. Note that one patient reported history of COVID-19, which occurred 8 months before the vaccine. This patient did not have smell or taste dysfunction. One patient reported dysgeusia with an increased perception of sweet and loss of salty taste according to psychophysical test. The duration of chemosensitive disorders ranged from 4 to 10 days. At baseline, 3 patients underwent rhinofibroscopy that did not report nasal or olfactory cleft obstruction. The histories of cases are summarized in the present paper.
Patient Features.
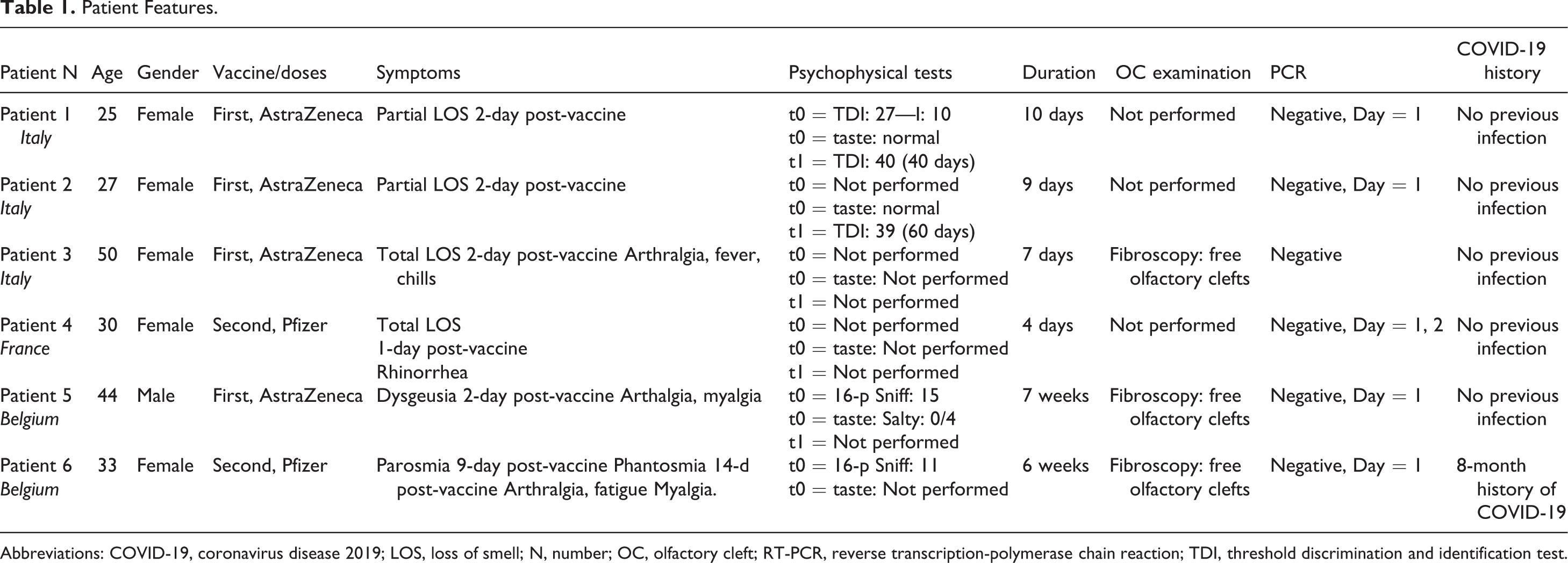
Abbreviations: COVID-19, coronavirus disease 2019; LOS, loss of smell; N, number; OC, olfactory cleft; RT-PCR, reverse transcription-polymerase chain reaction; TDI, threshold discrimination and identification test.
Case 1
A 25-year-old female developed partial loss of smell 2 days after the injection of the AstraZeneca vaccine (first injection). Patient did not report other general or nasal symptoms. Her medical history was unremarkable. As per protocol in patients with suspicious COVID-19 symptoms, nasal swab was performed reporting negative RT-PCR. She consulted the Smell Unit of the maxillofacial department of University Sassari Hospital (Italy) where physicians performed olfactory and gustatory psychophysical evaluations. The baseline Sniffin-Sticks test reported hyposmia (threshold discrimination and identification test, TDI = 27; Medisense). The taste evaluation was normal. Patient did not take any medication and did not follow olfactory training. She reported that the smell disorder lasted 10 days. Forty days after the onset of the olfactory disorder, the Sniffin-Sticks improved to normal values (TDI score = 40) meaning the resolution of hyposmia. Patient did not report adverse event after the second vaccine injection.
Case 2
A 27-year-old female consulted the Smell Unit of the maxillofacial department of University Sassari Hospital (Italy) for a 60-day history of post-vaccine partial loss of smell. At the onset of the smell disorder, patient benefited from nasal swab, which was negative. She did not report any otolaryngological or general symptoms. The smell disorder occurred after the first injection of the AstraZeneca vaccine. The patient medical history was unremarkable. Patient explained that she perceived an improvement of smell sense 9 days after the vaccine without olfactory training or medical treatment. The 40-day TDI testing with Sniffin-Sticks reported normosmia (TDI = 40) without taste dysfunction. There was no adverse effect after the second vaccine injection.
Case 3
A 51-year-old female consulted the ear, nose, and throat unit of Catania University Hospital (Italy) for a history of post-vaccine total loss of smell. The patient developed self-reported total loss of smell 2 days after the first injection of AstraZeneca vaccine. She also reported arthralgia, fever, and chills during a few days. Patient was examined by an otolaryngologist who did not observe nasal obstruction, rhinitis signs, or obstructed olfactory cleft. The total loss of smell persisted one week with a subsequent progressive improvement of smell. The patient reported fever and arthralgia after the second vaccine injection.
Case 4
A 30-year-old female consulted the otolaryngological department of Foch Hospital in Paris for a total loss of smell, which appeared suddenly after the second injection of the Pfizer vaccine. She had no medical or surgical history. Patient reported rhinorrhea but no nasal obstruction within the post-vaccine days. She benefited from 2 nasal swabs; performed one and 2 days after the onset of the olfactory disorder, both being negative. Four days after the onset of the olfactory dysfunction, patient reported progressive olfactory recovery. Note that she did not have adverse event at the first vaccine injection.
Case 5
A 44-year-old male consulted the Neurology department of CHU Brugmann (Belgium) for a post-vaccine history (AstraZeneca, first injection) of 10-day arthralgia, myalgia, and abdominal pain. Patient reported that sweet taste of foods and beverages was significantly increased, while the salty taste disappeared. The taste disorder of patient was associated with an inability to drink coffee or to eat sweet foods; leading to a mild weight loss. The otolaryngological examination did not report olfactory cleft inflammation. The history of patient just reported renal lithiasis. Patient benefited from nasal swab that was negative. The brain computed tomography scan was normal. The 16-pen Sniffin-Sticks test (Medisense) was normal (15/16), while the psychophysical taste evaluations (Burghart Taste strips; Medisense) confirmed the total loss of salty (0/4). The detection of sweet, acid, and bitter tastes was normal. General symptoms resolved after 10 days, while the dysgeusia persisted 7 weeks. Patient did not report adverse events at the second vaccine injection.
Case 6
A 33-year-old female consulted the Otolaryngology department of CHU Saint-Pierre for a history of post-vaccine severe parosmia. Patient reported the occurrence of parosmia and phantosmia 9 and 14 days after the second injection of Pfizer vaccine. She also reported arthralgia, myalgia, and fatigue that resolved after one week. The nasal swab was negative. The history of the patient included COVID-19 infection 8 months ago, which lasted a few days with a history of 7-day loss of smell. The patient recovered smell after 1 week of COVID-19 infection and did not report any smell disorder over the next few months. The otolaryngologist performed a 16-pen Sniffin-Sticks test reporting hyposmia (11/16). The olfactory clefts were free and there was no nasal obstruction or rhinorrhea. Patients received 7-day oral corticosteroids and B9 to B12 vitamins and the parosmia and phantosmia progressively improved throughout the 6 weeks post-vaccine without reaching full recovery.
Discussion
The development of smell and taste disorders after the administration of vaccine seems to be a very rare complication, which was previously reported with the influenza vaccine. 5,6 According to Doty et al, the occurrence of olfactory dysfunction after influenza vaccine may concern 0.19% of patients, while they did not observe gustatory dysfunction. 6 To date, the pathophysiological mechanisms are still unknown. The most prevalent post-vaccine symptoms include fatigue, headache, arthralgia, myalgia, and fever, 7 but there is no mention of olfactory or gustatory dysfunction in studies. 2,3,7 A few studies reported very rare otolaryngological adverse events, consisting of rhinorrhea, postnasal drip, cough, and nasal obstruction. 8,9 The development of a post-vaccine inflammatory reaction in the olfactory neuroepithelium could explain a transient smell disorder but this hypothesis remains not demonstrated according to our observations because patients did not have blocked olfactory clefts. A second hypothesis involves the presence of virus in the neuroepithelium or in olfactory bulbs without clinical findings. In these asymptomatic carriers, the vaccination could generate the development of antibodies and a related inflammatory reaction against the virus in this region, leading to transient loss of smell related to the destruction of infected cells. Recent studies supported that the prevalence of healthy carriers ranges from 17.9% to 51% of cases. 10 The high prevalence may support this second hypothesis, but the negative repeated swabs in our patients limit us in drawing firm conclusions. Future studies are needed to determine the prevalence of olfactory and gustatory dysfunctions in individuals who received vaccines. As stated by Doty et al, the presence of olfactory disorder after vaccine may be not event reported by the patient and require psychophysical olfactory evaluations.
Conclusion
The occurrence of olfactory and gustatory dysfunctions in adults benefiting from COVID-19 vaccines is still rare but has to be known by physicians and otolaryngologists. The report of these cases does not have to lead to a reduction of the vaccination because they appear exceptional. The pathophysiological mechanisms are poorly understood.
Footnotes
Authors’ Note
Luigi A. Vaira and Sven Saussez equally contributed and as co-senior author. Electronic informed consent was obtained from all individual participants. Informed consent was obtained from patients enrolled in the study. IRB not required.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.