
Abstract
Objectives:
The present study attempted to investigate the clinical efficacy of a surgical method involving a combination of cross flap with autologous auricular cartilage transplantation in the treatment of type I to III congenital concha-type microtia.
Methods:
The present retrospective study was conducted on the clinical and postoperative data of 50 patients with unilateral type I to III concha-type microtia treated with a combination of cross flap and autologous auricular cartilage transplantation at the Plastic Surgery Hospital of Chinese Academy of Medical Sciences from January 2018 to December 2021.
Results:
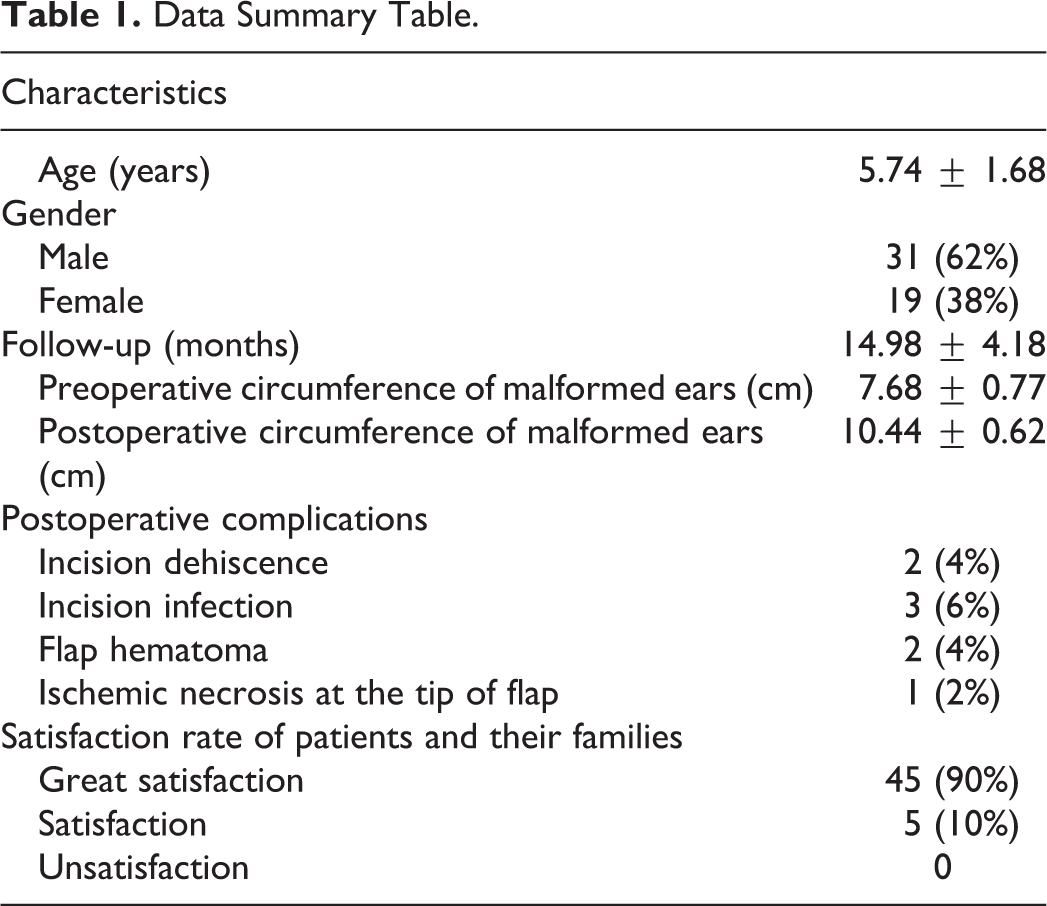
The postoperative perimeters of malformed ears were significantly larger than the preoperative perimeters (P < .05). Of the total, 2 patients exhibited incision dehiscence, 3 patients exhibited incision infection, 2 patients exhibited flap hematoma, and 1 patient exhibited ischemic necrosis at the flap tip. The satisfaction rate of the patients and their families was 100%.
Conclusions:
The surgical method involving a combination of cross flap and autogenous auricular cartilage transplantation was effective in treating patients with type I to III congenital concha-type microtia, and therefore, this surgical approach can be applied widely to correct this deformity.
Introduction
The human ear is a complex organ made of tissues formed by a close bonding of the skin and cartilage, 1 and it exhibits a 3-dimensional structure composed of many subunits. 2 Symmetrical and structurally normal ears are vital for facial aesthetics. However, abnormal growth and development of the ear may occur due to various reasons such as ethnic factors, genetic factors, and exposure to teratogenic drugs during pregnancy, resulting in congenital concha-type microtia. 3,4 Moreover, no unified guideline is available for the treatment of minor congenital concha-type microtia through plastic and reconstruction surgery.
Based on our experience in the treatment of congenital concha-type microtia, we have classified this deformity into 4 types. 5 A malformed ear having a perimeter more than three-fourth of the normal contralateral ear perimeter––exhibiting normal shapes of the scapha, antihelix, and inferior crura of antihelix and partial formation of the superior crus of the antihelix and triangular fossa––constitutes type I concha-type microtia. A malformed ear having a perimeter less than three-fourth of the normal contralateral ear perimeter––exhibiting normal shapes of the antihelix and inferior crura of antihelix and abnormal shapes of the scapha, superior crus of antihelix, and triangular fossa––constitutes type II concha-type microtia. A malformed ear with a perimeter less than three-fourth of the normal contralateral ear perimeter––exhibiting abnormal shapes of the antihelix, inferior crura of antihelix, scapha, superior crus of antihelix, and triangular fossa––constitutes type III concha-type microtia. A malformed ear with a perimeter less than one-third of the normal ear perimeter constitutes type IV concha-type microtia, and most auricle structures in this deformity are abnormal.
Although the surgical treatment for this deformity has not been standardized yet, the treatment of type IV concha-type microtia by auricular reconstruction has been a consistent choice of plastic surgeons. 6 In the present study, cross flap along with autologous auricular cartilage transplantation was used to achieve favorable outcomes in patients with type I to III concha-type microtia.
Patients and Methods
Clinical Data
The present retrospective study was conducted on the clinical and postoperative data of 50 patients with unilateral type I to III concha-type microtia who were treated with a combination of cross flap and autologous auricular cartilage transplantation at the Plastic Surgery Hospital from January 2018 to December 2020. The study was approved by the Medical Ethics Committee. All patients participating in the present study signed informed consent.
Surgical Methods
The “Z” flap was designed at the upper edge of the helix and lower edge of the auricular conchal cavity (Figure 1). Local anesthesia was administered by injecting lidocaine along the design line. The surgeon incised the skin at the lower edge of the auricular conchal cavity by using a scalpel. Approximately 1 to 3 cm long auricular cartilage was removed from the auricular conchal cavity (Figures 2 and 3). The skin of the helix was excised according to the design line (Figure 4). The cartilage of the helix was separated from the skin and stretched. Then, the cartilage of the outer ear wheel was cut from the middle part, and the spare cartilage piece that was removed from the lower edge of the auricular conchal cavity was transplanted to the incised cartilage of the helix (the spare auricular cartilage was trimmed or spliced before transplantation; Figures 5 and 6) to extend the perimeter of the ear. The skin on the upper edge of the helix and that on the lower edge of the auricular conchal cavity were cross-sutured (Figure 7).

Preoperative design.
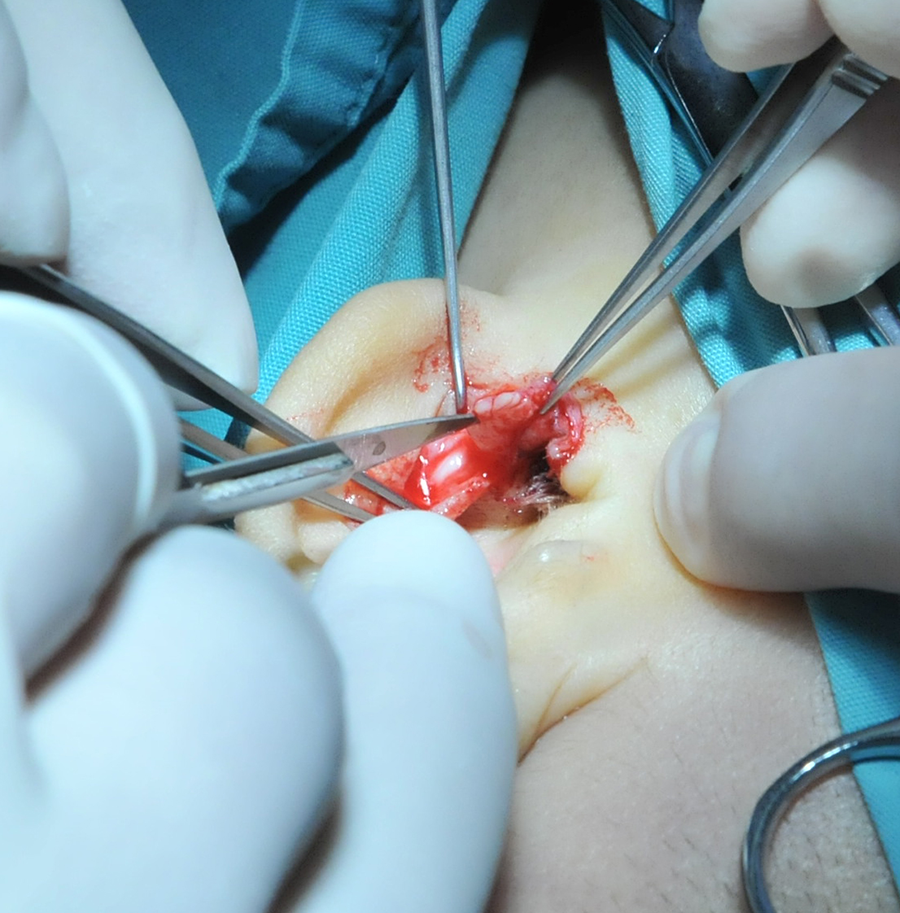
Cut the skin at the lower edge of the cavity of auricular concha and the auricular cartilage was removed from the cavity of auricular concha.

The spare auricular cartilage.
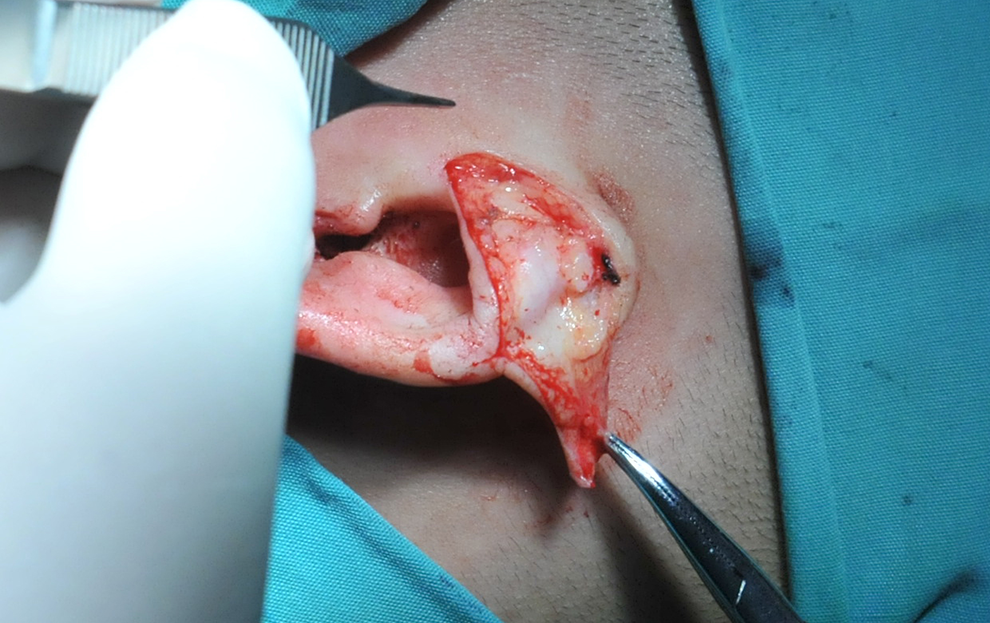
Cut the skin of the helix to the ear cartilage.
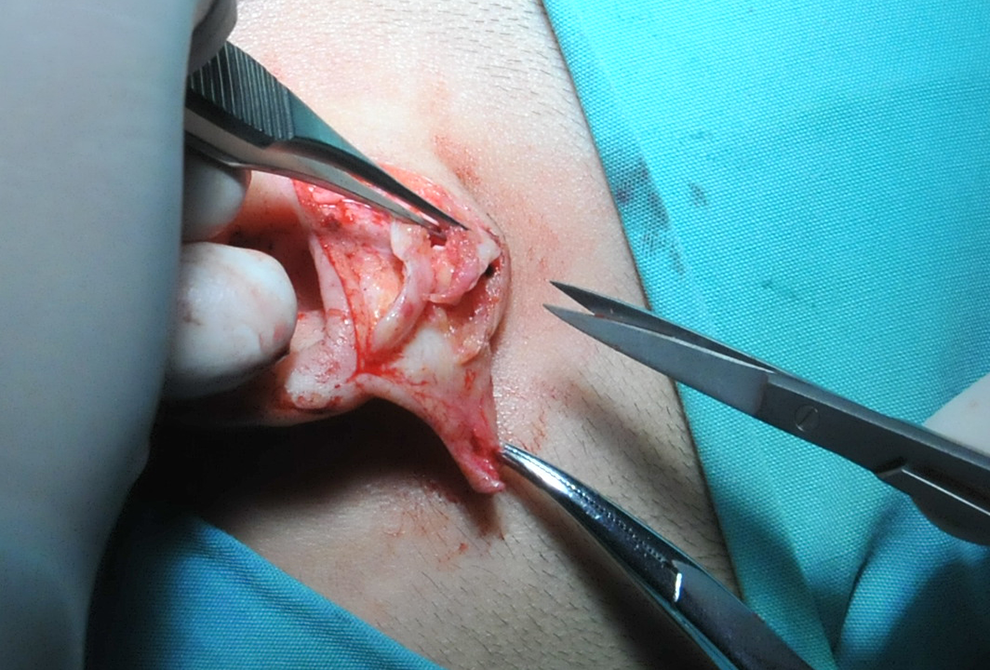
The cartilage of the outer ear wheel was cut from the middle part.
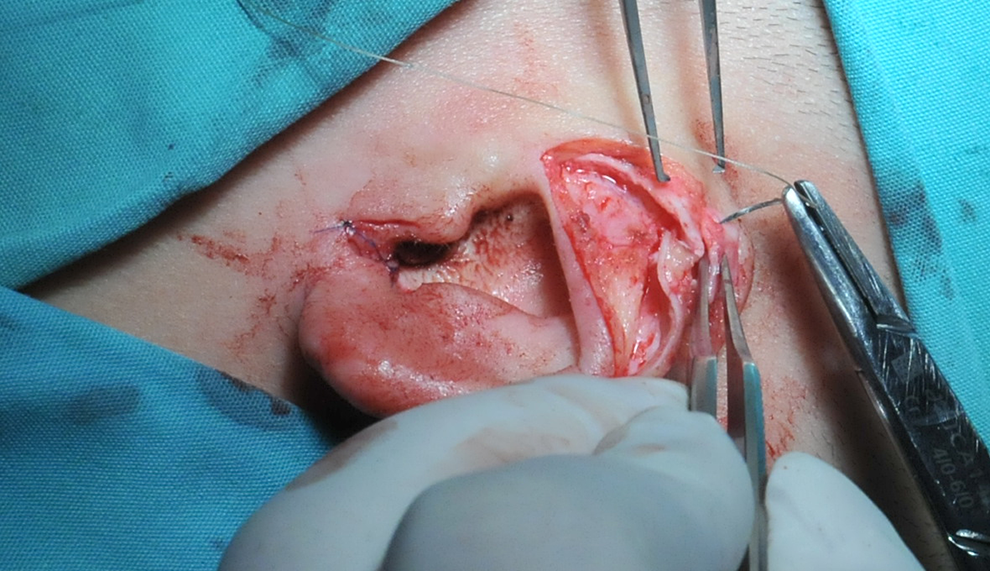
The spare cartilage piece was transplanted to the incised cartilage of the helix.

The skin on the upper edge of the helix and the skin on the lower edge of the cavity of auricular concha were cross-sutured, respectively.
Main Outcome Measures
The main outcome measures were the preoperative and postoperative perimeters of the malformed ears, postoperative complications, and satisfaction rate of the patients and their families (the survey on satisfaction of patients and their family was conducted by outpatient follow-up nurses).
Results
All the 50 patients were aged between 2 and 9 years, with an average age of 5.74 ± 1.68 years. Of these, 31 patients were male and 19 patients were female. Type I concha-type microtia was observed in 8 patients, type Ⅱ concha-type microtia was observed in 17 patients, and type III concha-type microtia was observed in 25 patients. None of the patients exhibited diseases that could affect the surgical outcome. The patients were followed up for 5 to 22 months, with an average follow-up period of 14.98 ± 4.18 months. The average preoperative and postoperative perimeters of the malformed ears in the 50 patients were 7.68 ± 0.77 cm and 10.44 ± 0.62 cm, respectively. The Shapiro-Wilk test was used to perform the normality test, which revealed a normal distribution of the preoperative and postoperative data of the malformed ear perimeters (P > .05). Then, the SPSSAU Data Science Analysis platform (https://spssau.com) was used to perform paired t test for the 2 datasets, which indicated that the postoperative perimeters of the malformed ears were significantly larger than the corresponding preoperative perimeters (P < .05). Of the 50 patients, 2 patients exhibited incision dehiscence, 3 patients exhibited incision infection, 2 patients exhibited flap hematoma, and 1 patient exhibited ischemic necrosis at the flap tip. The questionnaire survey for the satisfaction rate of the patients regarding the therapeutic effect of operation exhibited that 45 patients and their families were very satisfied and 5 patients and their families were satisfied. Overall, the satisfaction rate of the patients and their families was 100% (Table 1).
Data Summary Table.
Case Report
Patient 1 (male, aged 5 years) exhibited type III concha-type microtia. The patient underwent surgery under general anesthesia. The cartilage piece that was removed from the lower edge of the auricular conchal cavity was transplanted to the helix by the surgeon to extend the perimeter of the ear. The skin on the upper edge of the helix and that on the lower edge of the auricular conchal cavity were cross-sutured, The patient was followed up for 12 months. The postoperative auricle morphology of the patient improved significantly, and no postoperative complications were observed. The patient and his family were satisfied with the operation (Figures 8 –11).

Preoperative frontal view of the patient 1.

Preoperative profile view of the patient 1.

Postoperative frontal view of the patient 1.

Postoperative profile view of the patient 1.
Patient 2 (male, aged 6 years) exhibited type III concha-type microtia. The patient was successfully treated with a combination of cross flap and with autologous auricular cartilage transplantation under general anesthesia and then followed up for 15 months. After the operation, the auricle perimeter in the patient was increased significantly, and no complications were observed. The patient and his family were satisfied with the operation (Figures 12 –15).

Preoperative frontal view of the patient 2.

Preoperative profile view of the patient 2.

Postoperative frontal view of the patient 2.

Postoperative profile view of the patient 2.
Discussion
The surgical method involving a combination of cross flap and autologous auricular cartilage transplantation reconstructs the shape and size of the deformed ear similar to those of the normal contralateral ear, mainly by increasing the deformed ear perimeter. This surgical procedure renders the ears on both sides symmetrical, which allows patients to easily wear glasses and masks. The present study used the cross flap along with autologous auricular cartilage transplantation to treat type I to III congenital concha-type microtia. The normal ear perimeter is approximately 11 cm. We observed that patients having malformed ears with a preoperative perimeter of >6 cm were suitable for this operation. The therapeutic effect of the surgical method, which involved a combination of cross flap and autogenous auricular cartilage transplantation, was found to be superior in ears with a perimeter close to that of normal ears.
Because of differences in the ear size and degree of deformity among patients with type I to III congenital concha-type microtia, the therapeutic effect of surgery varies among these patients. The perimeter of the ear in type I concha-type microtia is more than three-fourth of the contralateral ear perimeter, and the morphology of the ear substructures is majorly normal. Therefore, the shape and size of the deformed ear can be constructed similar to those of the normal ear by using this surgical method. The perimeter of the ear in type II concha-type microtia is less than three-fourth of the normal ear perimeter, and the shapes of scapha, antihelix, and triangular fossa are abnormal. Thus, this surgical method can increase the perimeter of the deformed ear and repair the abnormal morphology of the scapha, antihelix, and triangular fossa simultaneously. For example, for patients with deformed antihelix, the surgeon incised the antihelix area open while extracting the ear cartilage. Then, the surgeon constructed the open cartilage part of the antihelix area into a cartilage tube (Figure 16) and used the cartilage tube to form the antihelix with a normal shape. The perimeter of the ear in type III concha-type microtia is less than three-fourth of the normal ear perimeter, and most of the ear subunits are abnormal. Therefore, the size and shape of the deformed ear must be adjusted initially in these patients. The ear cartilage may require splicing to increase its length during the ear cartilage transplantation to reconstruct the perimeter of the deformed auricle similar to that of the normal auricle. The surgical method described in the present study exhibited a significant therapeutic effect in terms of the increased ear perimeter and improved ear morphology in patients with type I to III congenital concha-type microtia. However, the comprehensive therapeutic effect was optimal in type I and type II concha-type microtia, followed by type III concha-type microtia.
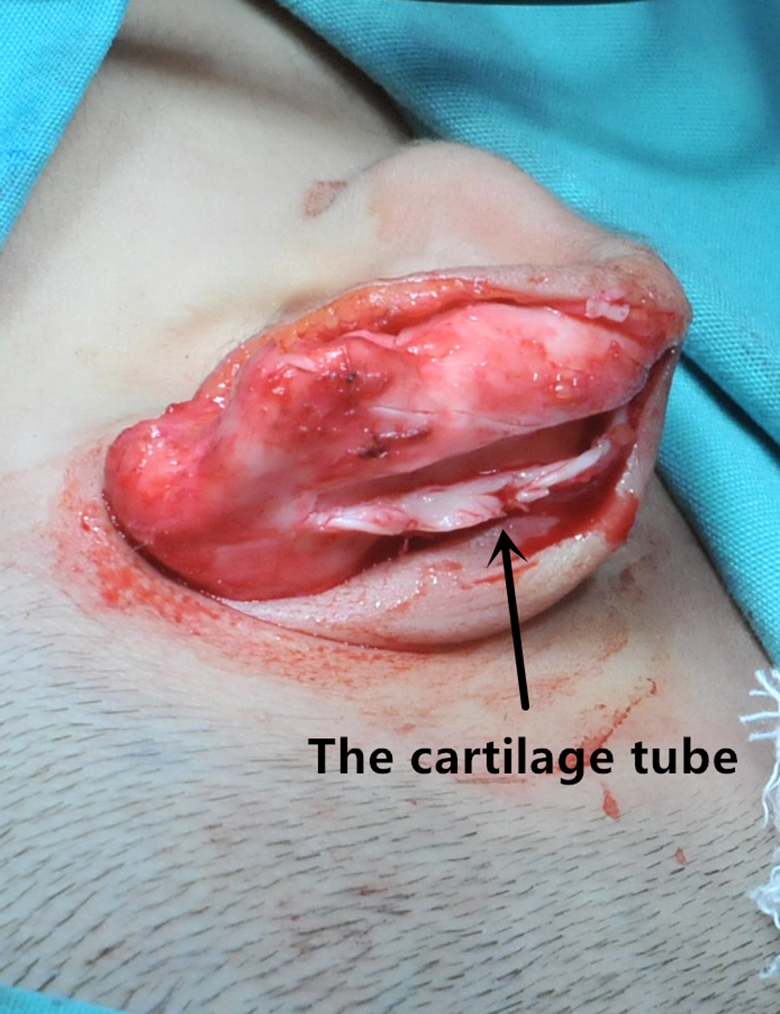
The surgeon makes the open cartilage part of the antihelix area into a cartilage tube.
A special standard satisfaction questionnaire was designed to evaluate the satisfaction of patients and their families with the operation from the following 4 perspectives: postoperative ear size, postoperative ear shape, symmetry of the bilateral ears, and postoperative complications. The full score of the satisfaction questionnaire was 20, with scores of 16 to 20 denoting great satisfaction, those of 12 to 15 denoting satisfaction, and those of <12 denoting dissatisfaction. The questionnaires were filled out anonymously by the patients and their families. The satisfaction survey was conducted by outpatient follow-up nurses, and the chief surgeon did not participate. Thus, the possibility of statistical deviation due to fear of the family members expressing their opinions was obliterated, and therefore, the results of our satisfaction survey were credible. Additionally, conversation with patients and their families before operation considerably affected the satisfaction rate of the patients after operation. The expectation of patients and their family regarding the outcomes can be effectively reduced through preoperative conversation, which can help patients easily accept the postoperative outcomes. This may also be the main reason for the 100% satisfaction rate of patients and their families for the postoperative results in the present study.
Special attention should be paid to the protection of blood circulation of the skin flap in the cross skin flap combined with autologous auricular cartilage transplantation. Superior blood circulation can ensure the survival of the cross flap and the success of the surgical procedure. Additionally, firm fixation of suture should be ensured when the autogenous auricular cartilage is transplanted to the helix cartilage to avoid failure of the operation. Hemostasis should be achieved at the active bleeding points before suturing the incision to prevent postoperative hematoma formation. Additionally, aseptic conditions should be maintained to prevent bacterial infection.
The present study exhibited the incidence of incision dehiscence after surgery in 2 patients due to increased tension in the incision caused by hematoma, indicating that the incidence of incision dehiscence after surgery can be reduced by preventing postoperative hematoma. The treatment of postoperative hematoma caused by incision dehiscence involves the removal of hematoma after opening the incision in a sterile environment and then resuturing the incision. The incision healed well after treatment. Postoperative infection of the incision, which manifested as redness and swelling of the incision and fever, was observed in 3 patients in the present study. The infected incision was treated with antibiotics, disinfected with 75% alcohol, and redressed. The redness and swelling of the incision disappeared, and the patients’ body temperature returned to normal after treatment. Thus, the incision healed uneventfully. Postoperative ischemic necrosis of the flap tip was observed in 1 patient. The necrotic area of the flap was treated by changing the dressing due to the small area of necrosis. The incision healed well after treatment. The suture knot should be loose when the flap tip is sutured because it can effectively prevent postoperative necrosis of the flap tip.
To the best of our knowledge, the present study is the first to use cross flap along with autologous auricular cartilage transplantation for the correction of type I to III congenital concha-type microtia, and the treatment exhibited favorable clinical results. However, the present study has certain limitations. The sample size of the study was small, with the participating patients being mainly from China. Therefore, future multiracial studies with a larger sample size are required to verify the findings of this study.
Conclusion
The combination of cross flap and autogenous auricular cartilage transplantation is an effective procedure for correcting type I to III congenital concha-type microtia. After surgery, the perimeters of the malformed ears increased significantly, with fewer complications, and the patients and their families were highly satisfied. Therefore, this procedure can be widely used for the treatment of type I to III congenital concha-type microtia.
Footnotes
Acknowledgments
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article:This study is supported by the Medical and Health Science and Technology Innovation Project of Chinese Academy of Medical Sciences (2016-12M-1-002), National Multidisciplinary Cooperative Diagnosis and Treatment Capacity Building Project for Major Diseases of China (1112421015 21025) and Fundamental Research Funds of the Chinese Academy of Medical Sciences (20077).