
Abstract
Introduction
Question mark ear is a relatively rare ear deformity, first reported as a familial case by Vincent, and later formally named question mark ear by Cosman.1,2 It is also known as butterfly ear in China. This deformity is characterized by varying degrees of notches or complete separation between the helix and the earlobe, and in severe cases, even earlobe absence. It is often accompanied by protrusion and outward rotation of the upper part of the ear, with partial or complete disappearance of the antihelix. This deformity can occur as a sporadic case, a familial case, or as one of the specific manifestations of auriculocondylar syndrome (ACS), but the etiology is still unclear. From an embryological perspective, the discontinuity between the helix and the earlobe may be related to the deficiency or absence of the fifth and sixth hillocks located in the first and second pharyngeal arches.2,3 From a genetic perspective, the occurrence of ACS is related to abnormalities in the EDN1-EDNRA-DLX signaling pathway, which plays an important role in the development of pharyngeal arches and mandibular differentiation in vertebrates. 4 Studies have found that gene variations in EDN1, PLCB4, GNAI3, and MEF2C are important targets for the occurrence of various genetic patterns associated with ACS,5-11 but the specific pathogenic mechanism is still unclear and requires further research. Currently, there is limited literature on the treatment of question mark ear. We thought that the correction of question mark ear mainly involves 2 parts: one is improving the wide and outward appearance of the upper part of auricle, another is repairing the continuity between the helix and the earlobe or the absence of the earlobe. So that, we have explored a surgical method that combines costal cartilage transplantation with the auricular cartilage folding technique, which address these issues simultaneously and achieved ideal and stable outcomes.
Patients and Methods
A retrospective medical record review of all question mark ear patients who underwent correction surgery through autologous costal cartilage graft combined with auricular cartilage folding technique between January 2020 to December 2022 was conducted for this study. A total of 26 patients, in the range age of 6 to 25 years old (mean age of 9.4 years), were enrolled in this study. All cases were sporadic and unilateral. According to the clinical manifestation of the lower part of auricle, 11 cases showed a discontinuity between the helix and the earlobe and 15 cases showed earlobe absence (Figure 1). All patients underwent their first operative related to otoplasty. Written informed consents were obtained from the legal guardians of each patient participating in the study. Patients were followed up by outpatient appointments. The Visual Analog Score (VAS) was used to assess the cosmetic outcomes of the donor-site scar, which ranges from 0 (no cosmetic issue) to 10 (worst cosmetic outcome imaginable) and the Numerical Rating Scale (NRS) was used to assess the pain throughout the 10 day hospitalization period. An NRS of 0 signifies the absence of pain, 1 to 3 indicate mild pain, 4 to 6 indicate moderate pain, and 7 to 10 signify severe pain. Satisfaction was recorded based on a 5-point Likert Scale, which was in order of satisfied, partial satisfied, fair, dissatisfied, very dissatisfied.

(a-d) Question mark ear deformity, characterized by a discontinuity between the lower border of the ear helix and the earlobe. (e-h) Question mark ear deformity, characterized by the absence of the earlobe structure, protrusion and outward deviation of the upper half of the auricle, and absence of the antihelix.
This study was approved by the independent ethics committees of the Plastic Surgery Hospital, Chinese Academy of Medical Sciences, and the Peking Union Medical College.
Preoperative Design
A computed tomography scanning and 3D reconstruction of the costal cartilage was performed to guide the harvesting of the cartilage. In our study, taking the natural curvature and width of the costal cartilage into consideration, all patients used the ipsilateral portion of the seventh costal cartilage, which prefer to get better match to the existing structure of the auricle. In addition, an ear template was drawn based on the size and shape of the healthy side ear to guide the carving of the costal cartilage and morphological comparison during the procedure (Figure 2).
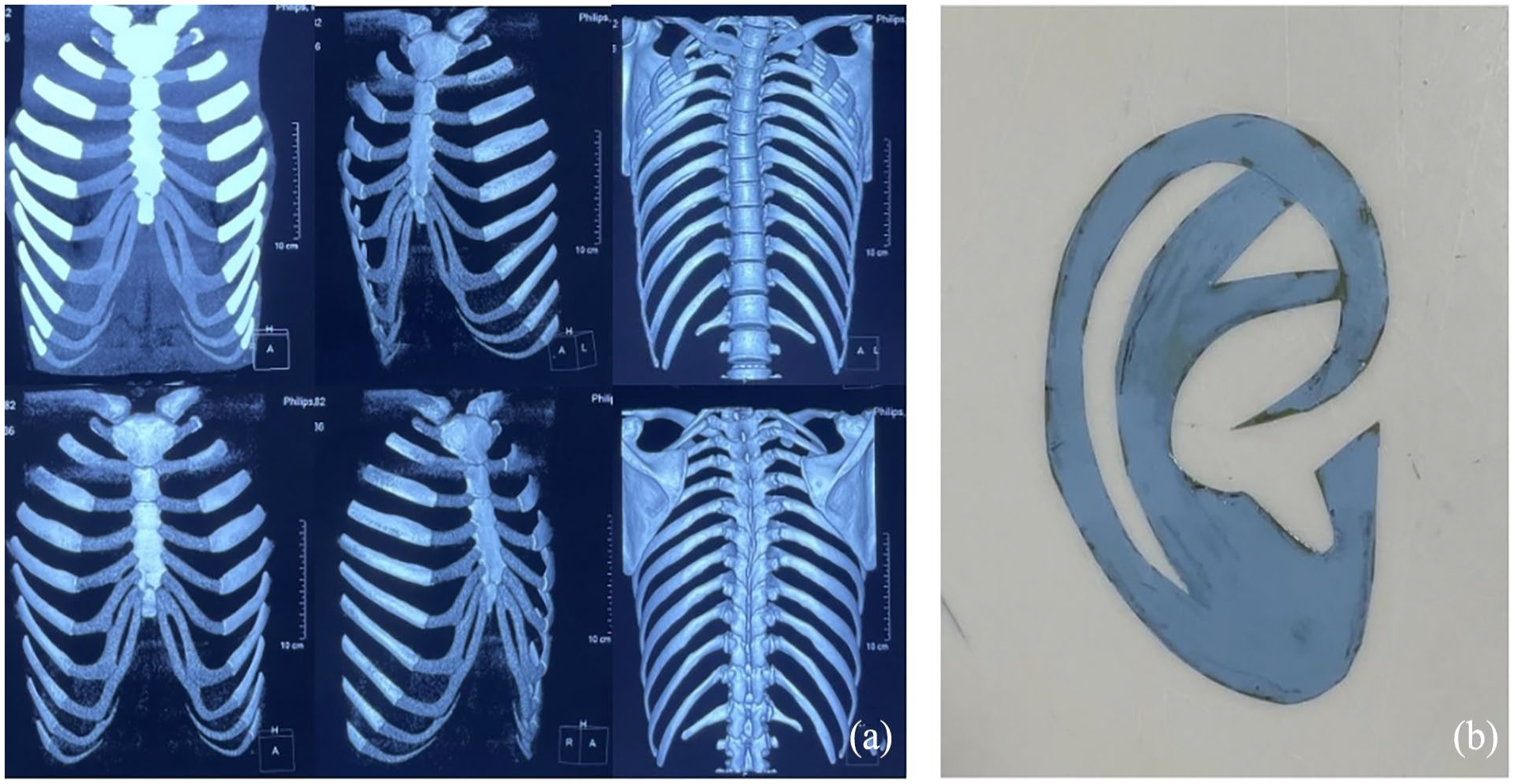
(a) CT scanning and 3-dimensional reconstruction of costal cartilage. (b) Ear template drawn based on the structure and size of the healthy side ear. CT, computed tomography.
Soft Tissue Dissection and Costal Cartilage Carving
The procedure was performed under general anesthesia in conjunction with adequate local infiltration anesthesia administered (2% lidocaine combined with epinephrine 1:100,000). The skin was incised along the predesigned vertical cut located behind the ear and the subcutaneous layer was dissected to create a posterior auricular skin flap. And then, the lower part of the auricular cartilage was expanded to create a subcutaneous pocket as well.
The ipsilateral seventh costal cartilage was fully dissected from the perichondrium, and then a segment of approximately 4 to 5 cm in length, which centered around the bulging area, was harvested. After personalized carving, the rib cartilage was placed into the subcutaneous pocket and the position was adjusted until satisfactory alignment was achieved with the upper and lower parts of the auricle. The upper part of the costal cartilage was connected to the auricular cartilage with polydioxanone synthetic absorbable suture, and the lower part was sutured and secured to the subcutaneous layer of the skin with 4-0 absorbable thread. At last, Vaseline rolls were used to fix the cartilage in place with #0 silk thread, and the auricular posterior skin flap was pushed back and sutured with 5-0 polypropylene nonabsorbable suture (Figure 3).
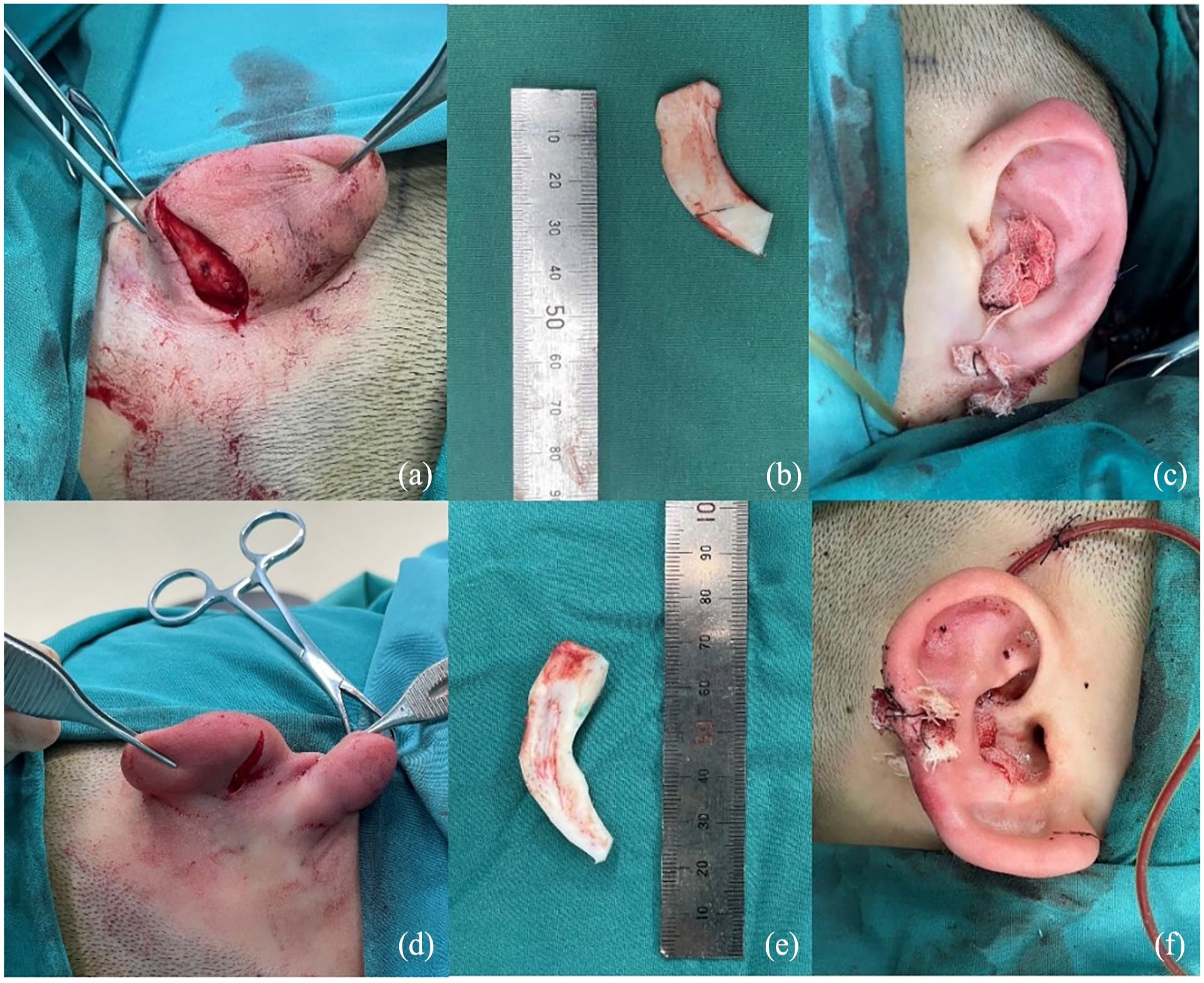
(a and d) Designed incision behind the ear; (b) earlobe carved from a portion of the seventh costal cartilage; (e) ear concha carved from a portion of the seventh costal cartilage, used to reshape the ear contour with natural continuity; (c and f) immediate postoperative outcomes.
Folding of the Upper Half of the Auricular Cartilage
The skin was incised according to the scissor-shaped incision on the upper posterior part of the ear. After adequate hemostasis, the auricular cartilage was appropriately folded backward in parallel to reshape the morphology of the antihelix and concha. Until the morphology of the upper portion of the auricle, the auriculocranial angle and the continuity between the upper and lower parts of the auricle were adjusted satisfied, the subcutaneous layer is sutured with 4-0 absorbable suture, and the skin is sutured with 5-0 polypropylene nonabsorbable suture One drainage tube was placed, which would be removed 5 days postoperatively. The sutures were removed 10 days after the surgery (Figure 3).
Results
All 26 patients were followed. The average follow-up period was 8.4 months (6-12 months). Representative results are shown in Figures 4 and 5. Patients got natural continuity between the helix and the earlobe or complete earlobe structure by autologous costal cartilage transplantation. Meanwhile, by removing a certain amount of skin and folding auricular cartilage backward, the prominent of the upper part of auricle and the inconspicuousness of antihelix were successfully addressed. Temporary swelling was the main complication and generally recovered within 3 to 6 months after surgery. The scars were located behind the ear, concealed, and without obvious hypertrophy. No hematoma, poor wound healing, infection, deformity recurrence, or obvious cartilage rebound occurred during the follow-up period. The patients’ chest scars were evaluated by an experienced plastic surgeon, with results showing the mean VAS was 0.85 (range 0-2). This indicates that all patients did not show significant scar hyperplasia during the follow-up period. No chest wall depression was observed through physical examination. The pain care record during hospitalization showed that all patients’ NRS scores were highest on the first day after operation, with an average score of 2.2 (range 0-4). Only one patient felt moderate pain, while the rest were mild pain. The pain scores gradually decreased over the 10 days, and none was recorded significant pain on the 10th day postoperatively. Twenty-three patients (88.5%) were satisfied, 3 (11.5%) were partially satisfied, and none was unsatisfied.
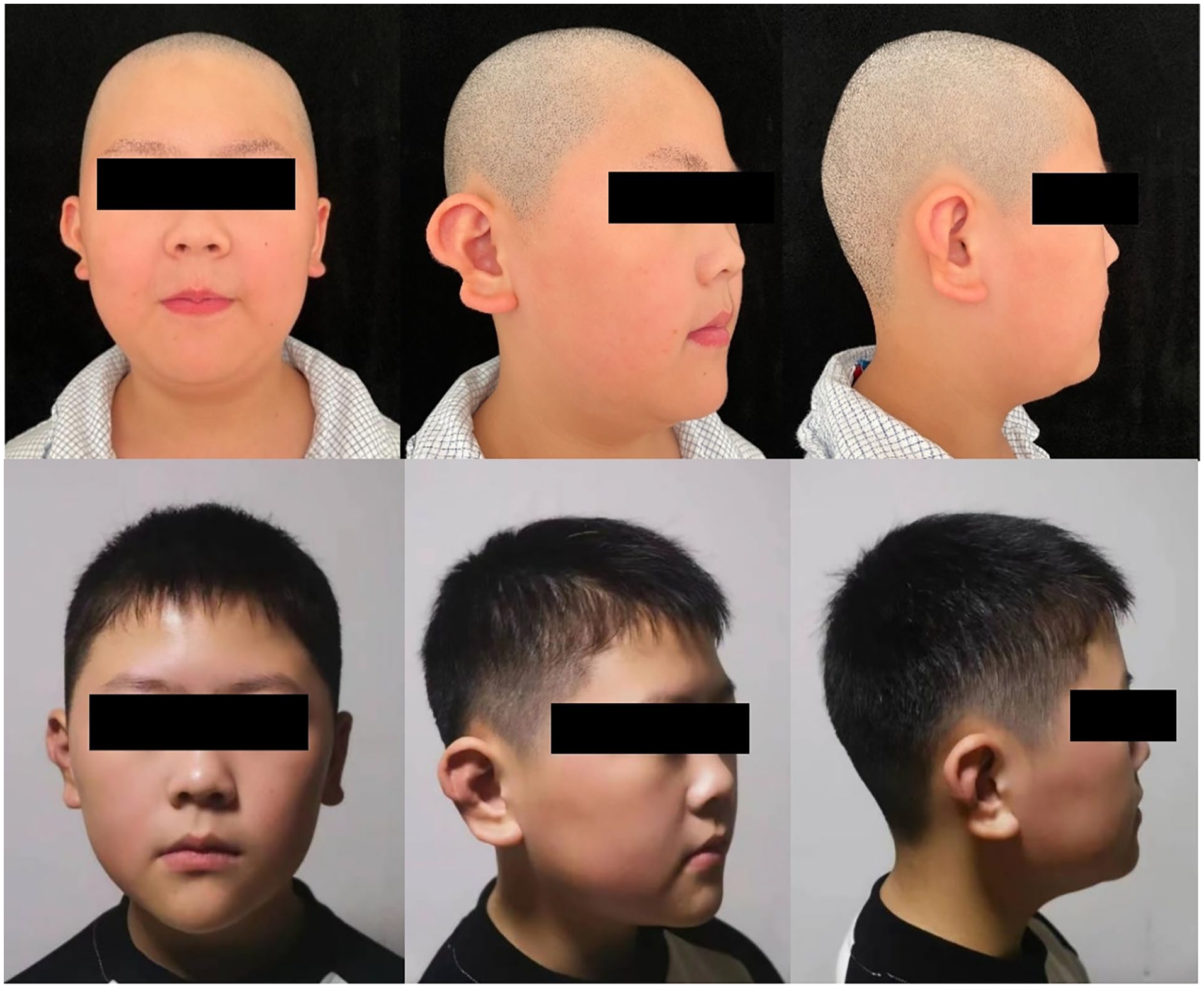
An 8-year-old boy with a right question mark ear, characterized by a discontinuity between the lower border of the ear helix and the earlobe, as well as a mild outward deviation of the upper half of the ear contour. The antihelix remained relatively intact. At 6 months after surgery, the reconstructed ear exhibited a natural and smooth contour along the edge, with an improvement in the outward deviation. Both sides of the ears were essential symmetrical.

A 10-year-old boy presented with a right question mark ear deformity characterized by the absence of the earlobe and a significant outward deviation of the upper half of the ear contour, with no apparent antihelix. At 9 month follow-up of the patient, the earlobe appeared natural, and the antihelix was clearly defined. The protrusion of the upper part of the ear showed significant improvement.
Discussions
Question mark ear is a rare congenital ear deformity, and there is no systematic classification and treatments internationally. There are some researchers who divide the deformity into moderate and severe cases according to the clinical manifestations of the lower part of the auricle. Moderate cases exhibit varying degrees of notches or complete separation between the helix and the earlobe, while severe cases involve the partial or complete disappearance of the lower border of the helix and the earlobe. Different surgical methods have been reported for different degrees. For moderate deformities, Cosman and Brodovsky12,13 initially used a local skin flap transfer technique with an anterior ear incision. This method was relatively simple and improved the shape of the deformed ear. However, it increased the anterior scar and lead to asymmetry in the sizes of both ears, which limited its use in the treatment of unilateral cases. 14 In addition, due to the lack of cartilage support, there was a higher possibility of deformity recurrence. Subsequently, Elsahy, Vayvada, Al-Qattan, and others1,14-16 introduced methods using a postauricular incision, combined with skin flap transfer and auricular cartilage grafting. These methods not only hide the scar but also address the issues of protrusion in the upper part of the auricle and soft tissue deficiency in the lower part of the auricle respectively. During the surgery, the size of ear could be effectively adjusted, providing a potential strategy for unilateral question mark ear. For severe deformities, Panbo 17 introduced a 2-stage expansion method. In the first stage, local skin expansion was got by implanting an expander. In the second stage, costal cartilage was harvested and sculpted, which was then covered with the expanded skin flap. Although this method effectively offers sufficient skin, the increased number of surgeries and longer treatment period cause repeated psychological and physical trauma to the child.
In general, the core treatment of question mark ear mainly involves solving 2 problems: the first is to improve the morphology of the upper half of the auricle. The aim of this step is to reduce the width of the upper half of the auricle and the auriculo-cranial angle, and to reshape the inconspicuous antihelix structure when necessary. Various methods based on classic techniques such as mattress sutures, cartilage flap tumbling, and folding suturing of auricular cartilage folding have been maturely applied.18-21 In this study, we folded and sutured the auricular cartilage after scratching the back surface of it. The purpose of scratching is to destroy the original mutual force of the cartilage, which is conducive to folding the cartilage in the direction we want, while minimizing the damage to the auricular cartilage and avoiding causing greater tissue deficiency. The second is to repair the discontinuity or tissue deficiency of the middle and lower parts of the auricle. This process often relies on tissue transplantation techniques. Rib cartilage and auricular cartilage are currently the most commonly used autologous materials in reconstructive surgery. They are used in different situations for nasal and auricular plastic surgeries due to their respective unique characteristics. 22 Autologous rib cartilage is abundant in supply, strong in support, and easy to carve. When sufficient septal cartilage is not available, rib cartilage has been a graft material for major nasal reconstruction. 23 It can play a significant role in lifting the tip of the nose, making it an ideal material for low nose. Compared to septal cartilage, thin rib cartilage has a stronger ability to maintain nasal tip height and nasal tip rotation. 24 It can be an effective alternative to rhinoplasty in Asians with features such as thick skin and a short nose. In addition, it is also commonly used in revision surgeries after multiple rhinoplasties or secondary nasal deformity correction surgeries.25-28 In auricular reconstruction, rib cartilage remains the first choice. The auricle carved from rib cartilage is clear and stable in shape, with strong compression resistance. 29 However, the downside is that rib cartilage is not easy to obtain, and excessive harvesting may lead to chest wall deformity. Iatrogenic pneumothorax and scar hyperplasia are also possible occurrences. Besides, rib cartilage often has varying degrees of calcification with the increase of age, and a high degree of calcification will limit its use. 30 The texture of the auricular cartilage is soft, easy to harvest, and the incision is concealed. Because it is similar to the characteristics of the alar cartilage, it can be used to repair local alar defects. 31 At the same time, it has a great advantage in shaping the mobility of the nasal tip so that it can be used alone or in combination with the septal cartilage for nasal tip reshaping.27,32 It is also commonly used for various congenital and secondary ear deformities.33-35 In addition, auricular cartilage can also be used for lower eyelid reconstruction, which is even superior to septal cartilage from the perspective of complications. 36 But its downsides are that the amount is limited, the sustaining power is weak, and the carving space is small, so it is not the first choice in the case of large tissue defects and high morphological requirements. To achieve more precise and stable results and reduce the possibility of re-repair, this study all adopted autologous rib cartilage graft. Its role in this deformity is to form the auricular concha to connect the discontinuous lower edge of the auricle and the earlobe, or to reconstruct the earlobe. We used the ipsilateral seventh rib cartilage, which is consistent with the base framework carvement in the modified Nagata method or expansion method for auricular reconstruction.37-39 Moreover, the ipsilateral rib cartilage with lower inner, higher outer contour and a naturally upturned tail matches the natural earlobe. The cartilage was harvested through an approximately 3 cm incision in the chest. Only 4 to 5 cm rib cartilage, which centered around the bulging area need to be harvested. Preserving perichondrium in donor site, filling the perichondrial pocket with cartilage remnants 40 and postoperative fixation with a chest strap for 3 to 6 months contribute to reduce the possibility of chest deformity. In addition, serratus anterior block was routinely administered by experienced anesthesiologist before surgery, and patient-controlled intravenous analgesia was arranged if necessary to reduce postoperative pain from cartilage harvesting. No significant donor site complications were observed in all patients during the follow-up period.
All patients in this study obtained substantial subcutaneous space and covering flaps by sufficiently dissociating and liberating, suggesting that not all patients with severe question mark ear deformities require skin expansion. Mobility of the mastoid skin and size of the opposite ear are important factors to make surgical plan. For patients with loose mastoid skin or a difference in length or width of the auricle on both sides within 5 mm, sufficient flaps can be obtained directly by sufficiently dissociating and liberating. For those with tighter skin or contralateral auricle is obviously larger, priority should be given to designing transfer flaps in the deformed ear itself and retroauricular hairless area.33,41 Although the 2-stage expansion effectively offer sufficient skin, multiple surgeries and longer treatment period cause repeated psychological and physical trauma to children. The superiority of the method we described is that most question mark ear patients can address the aforementioned problems in a single surgery and achieve stable results.
Also worthing mention, our study included a case presented with ipsilateral earlobe protrusion preoperatively, which is the same as that of contralateral. Earlobe protrusion can occur as an alone deformity or as an accompanying deformity in a variety of auricular deformities.18,42,43 Lobule is aligned to the helical rim on the same straight line in normal situation. 44 However, the congenital incongruity of the rotation of cavum and antihelix fold, or changes in the overall shape after auriculoplasty may lead to relative protruding earlobe. It is suggested that surgeon has better to reevaluate lobule prominence after the completion of the otoplasty techniques. 42 There are relatively limited literatures on the treatment for correcting protruding earlobe. Dermal-mastoid sutures have been used by some surgeons, although it may provide stable outcomes, it rises the risk of hematoma in mastoid region.45,46 The popular treatment strategy tends to design incision in the posterior lobule area and remove excess skin and (or) fat issue. Z-plasty, ellipse, dumbbell, or tennis racket shape excisions have been utilized. 47 Fishtail incision is the most commonly used basic design. Fishtail incision combined with asymmetric oblique suturation technique, fishlike excision combined with V-Y plasty, fishtail combined with triangular skin excision, and so on all have achieved good results.42,48 In this study, the patient’s supervisor did not wish the healthy side auricle receive extra wound and surgery. Considering to ensure symmetry in the earlobe shape of both auricles, we did not correct his protruding earlobe.
This study has 2 major limitations in term of small-scale patient series and relatively short-term follow-up. In addition, the basis of result evaluation is purely subjective and no routinely available quantitative measure of corrected auricle status. The technique and insights we proposed need further verification in the future practice. During the follow-up period, we did not receive unsatisfactory feedback.
Conclusions
The technique of autologous costal cartilage grafting combined with auricular cartilage folding is reliable in question mark ear correction. This method solves all deformities in a single procedure and achieves well-shaped auricle. It can be promoted in the future practice.
Footnotes
Acknowledgements
We thank the subjects and their families for participation in this study and all of the authors and coworkers for their contributions.
Data Availability Statements
All data generated or analyzed during this research are included in this article. Data supporting the findings of this study are available from the corresponding author on reasonable request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Natural Science Foundation of China (grant number 81701930).
Ethical Approval
This study was approved by the institutional review board of the Chinese Academy of Medical Sciences, Beijing, People’s Republic China (approval number: z201707).
Statement of Human Rights
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Declaration of Helsinki and its later amendments or comparable ethical standards.
Statement of Informed Consent
Informed written consent was obtained from the patient or their legal guardians for publication of this report and any accompanying images.