
Abstract
Background:
The Thai Rural ENT foundation has been conducting ear camps in Bhutan for many years to address the shortage of ENT specialists in the kingdom where patients are examined and treated for various ear illnesses. However, there has been no study conducted to assess the outcomes of such camps. This is the first study of its kind to be carried out in Bhutan.
Objective:
To study the spectrum of ear cases seen during the mobile ear camp, the intervention done and treatment outcomes.
Materials and Methods:
The study enrolled patients with ear disorders who presented to the mobile ear camp at Monggar Regional Referral Hospital, Bhutan, from January 6, 2020, to January 8, 2020. The following data were recorded: demographic details, preoperative clinical symptoms and otoscopic findings, preoperative audiogram, treatment or surgery done, postoperative middle ear and mastoid infection, wound infection, graft condition, any complications, and postoperative audiogram of operated cases. Patients who underwent surgery were followed up at 1 day, 6 weeks, and 2 months postoperatively.
Results:
Two hundred ten patients presented with otologic conditions and 43 underwent surgeries. Otitis media was the commonest disease detected, and tympanoplasty was the commonest surgery performed. The tympanic membrane closure rate was 92.1%, and the rate of hearing improvement was 63.2%.
Conclusion:
The ear camp had beneficial effect and showed good results.
Introduction
Bhutan is a small country in the eastern Himalayas with a population of 735 553 as of 2017. 1 Although the country is small by area with west-east span of 300 km and north-south span of 200 km, getting around the country is hindered by the mountainous landscape; it can take up to 2 days to travel from west to east of the country. This fact is particularly significant with respect to people’s accessibility to health care services. Bhutan is currently classified as a lower-middle income country.
Essential health services in both modern and traditional medicines are free for Bhutanese citizens, as guaranteed by the Constitution, based on a primary health care approach. 2 To provide health care, all major towns have general hospitals and all villages have primary health centers. The focus is mainly on primary health care. For a small population, Bhutan has 49 hospitals and 186 primary health centers. 3 The first doctors in Bhutan were trained only in the 1970s. As of 2019, there are around 376 doctors in the entire country, including general doctors, dentists, and specialists. 3 Although Bhutan has been able to double the life expectancy in the past 50 years which could be attributed to the primary health care approach, the need and demand for tertiary health care services is increasingly being felt. 4 Bhutan can no longer afford to refer patients for such services abroad as is the current practice. Specialists and subspecialists are in demand now more than ever. 5,6
There have been only 8 Bhutanese Ear Nose and Throat surgeons so far, 2 of whom have retired and one is from the military. Five ENT specialists are currently serving at the national referral hospital. Four more are undergoing training in Thailand and will return home in 2021 to 2022. 7 The critical pool of ENT surgeons to service the national referral hospital and the 2 regional referral hospitals has not been met. This has led to patients traveling long distances to the capital to seek ENT services. The goal of free healthcare is therefore jeopardized due to high out-of-pocket expenditure incurred by our patients. The other drawback of the lack of ENT surgeons has been the long waiting times in the outpatient department and huge backlog of cases requiring surgery. This has led to ENT surgeons being overworked and not able to devote time to update themselves or conduct research. All these factors combined, Bhutanese patients face a lot of delay in diagnosis and treatment of ENT cases which can be disastrous in cases like cancer.
The Ministry of Health (MOH) of the Royal Government of Bhutan has been in close collaboration with the Royal Kingdom of Thailand in the field of medicine ever since formal diplomatic relations were established in 1989. Thai Rural ENT Foundation has been conducting mobile ear camps in Bhutan since 2009. 8,10 The camps are usually organized in different regions of Bhutan. The visiting team stays in the country for around a week, and the follow-up of the cases seen during the camp is done by technicians and doctors. Although rough data are available about the number of people visiting previous camps, little is known about the spectrum of cases and the types of interventions done. Moreover, there has not been any study conducted till date either to assess outcomes of such camps.
Materials and Methods
The study was approved by the Ethics Committee of Rajavithi Hospital, Department of Medical Services, Ministry of Public Health, Thailand, and Research Ethics Board of Health (REBH) Ministry of Health, Royal Government of Bhutan. Administrative clearance was also granted by the Policy and Planning Division, MOH, Royal Government of Bhutan.
The study was performed prospectively. Subjects included patients presenting with ear conditions during the ear camp at Monggar Regional Referral Hospital (MERRH), Monggar District, Bhutan from January 6, 2020, to January 8, 2020. The mobile ear camp was organized by the Thai Rural ENT Foundation, in collaboration with MOH, Bhutan. The unit team consisted of 8 experienced ear surgeons, 5 nurses and 1 manager from Thailand and 1 Bhutanese ENT surgeon, 2 ENT technicians and a second-year ENT resident studying at Thailand. Surgical supplies comprised of 4 operating microscopes, 8 hydraulic chairs, and 60 sets of surgical instruments, drapes, and drills. Surgical instruments and drapes were sterilized using autoclave. All supplies and medications were brought from Bangkok.
The target population in Bhutan was informed about the Thai Mobile Ear camp using television and radio broadcasts. District hospitals noted details about appropriate cases and referred them to Monggar district. Informed consent was obtained from all participants.
Data collected via questionnaires was entered on a computer and stored in a password-protected, secure location by the Principal Investigator. Each patient was accorded a unique identification number, and the recorded data did not contain any identifiers of the participants.
Data were cleaned for inconsistencies and coded data were entered twice using Epidata Version 3.1 with proper checks for quality control. Data management, processing, and analysis were done using Epidata Analysis Version 2.2.2.183.
Since this is an observational study of patients with ear problems, we performed descriptive statistics which have been expressed in terms of percentages and ratios. The same has also been displayed in pictorial form in the form of tables. Chi-square test and Fisher exact test were also used for inferential statistics. P value of <.05 was considered statistically significant.
The following data were recorded: demographic data; preoperative history including ear discharge, ear pain, ear fullness, reduced hearing, preexisting facial palsy, duration of problem, prior intervention done, and examination findings such as wax in ear canal, tympanic membrane perforation, ear discharge, keratin debris, pretreatment audiogram; diagnosis, intervention done during ear camp (conservative or surgery); and type of surgery. Pain was assessed subjectively during the initial assessment as well as during postoperative follow-up visits using a numerical rating pain scale from 1 to 10 with one being the least and 10 being the highest pain intensity. Tympanoplasty procedures used type I overlay or underlay technique via an en-aural or post-aural approach. Mastoidectomy usually involved drilling down of the posterior canal wall, with middle-ear preservation. Patients received postoperative antibiotics (amoxicillin with clavulanate and ofloxacin ear drops) and analgesics (paracetamol) for 2 weeks.
Only the patients who underwent surgery were followed up for assessment. Patients were followed up 1 day, 6 weeks, and 2 months postoperatively. In every visit, the next follow-up date was reminded to all patients. The following data were recorded during the follow-up visits: surgical site hematoma, middle-ear and mastoid infection, wound infection, wound dehiscence, facial palsy, graft condition, and any other complications and 2-month postoperative audiogram. Surgical success was assessed in terms of tympanic membrane perforation closure, absence of otorrhoea, and complications and improvement in air conduction hearing threshold by at least 10 dB HL. Follow-up assessment was carried out by the first author and technicians from MERRH.
Results
During the 2 days’ camp, 545 people came to avail services from the team. Among them, around 210 people came with problems related to ear. The rest had issues related to nose and throat and were excluded from the study. Table 1 shows demographic details of the patients.
Demographic Details.
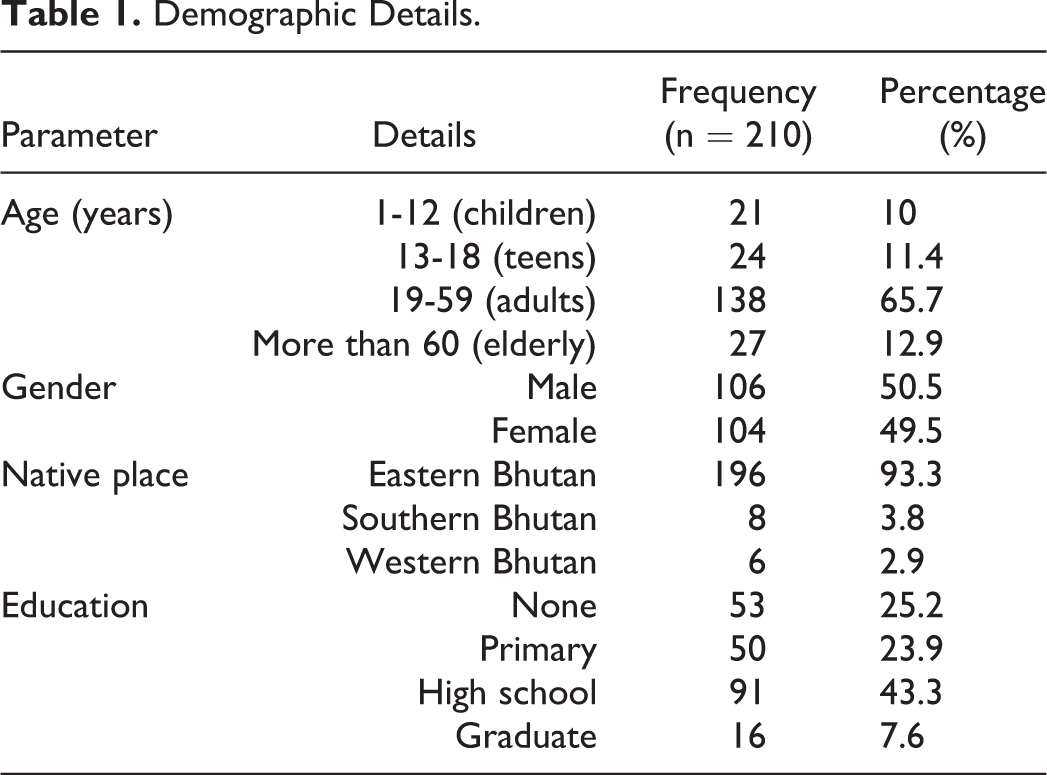
The majority of the study population were adults in the age group of 19 to 59 years (n = 138; 65.7%) with the youngest being 2 years and the oldest being 89 years old. The gender distribution was almost the same with 106 (50.5%) males and 104 (49.5%) females. The majority of the study population were from eastern Bhutan (93.3%) and most had received some form of formal schooling (74.8%).
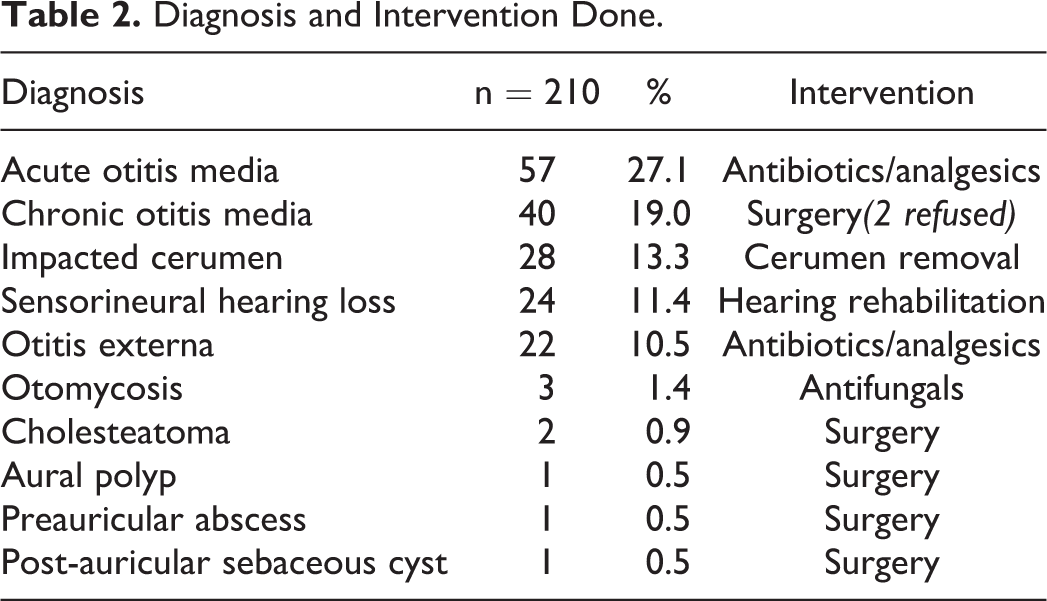
The most common diagnosis was acute otitis media (AOM; n = 57; 27.1%) followed by chronic otitis media (COM; n = 40; 19.0%) and impacted cerumen (n = 28; 13.3%). Thirty-one people had just come for ear checkup and had no significant findings (no diagnosis made). Table 2 shows the diagnoses and intervention given, and Table 3 elaborates on the commonest diagnosis made (otitis media).
Diagnosis and Intervention Done.
Details of Patients Diagnosed With Otitis Media.
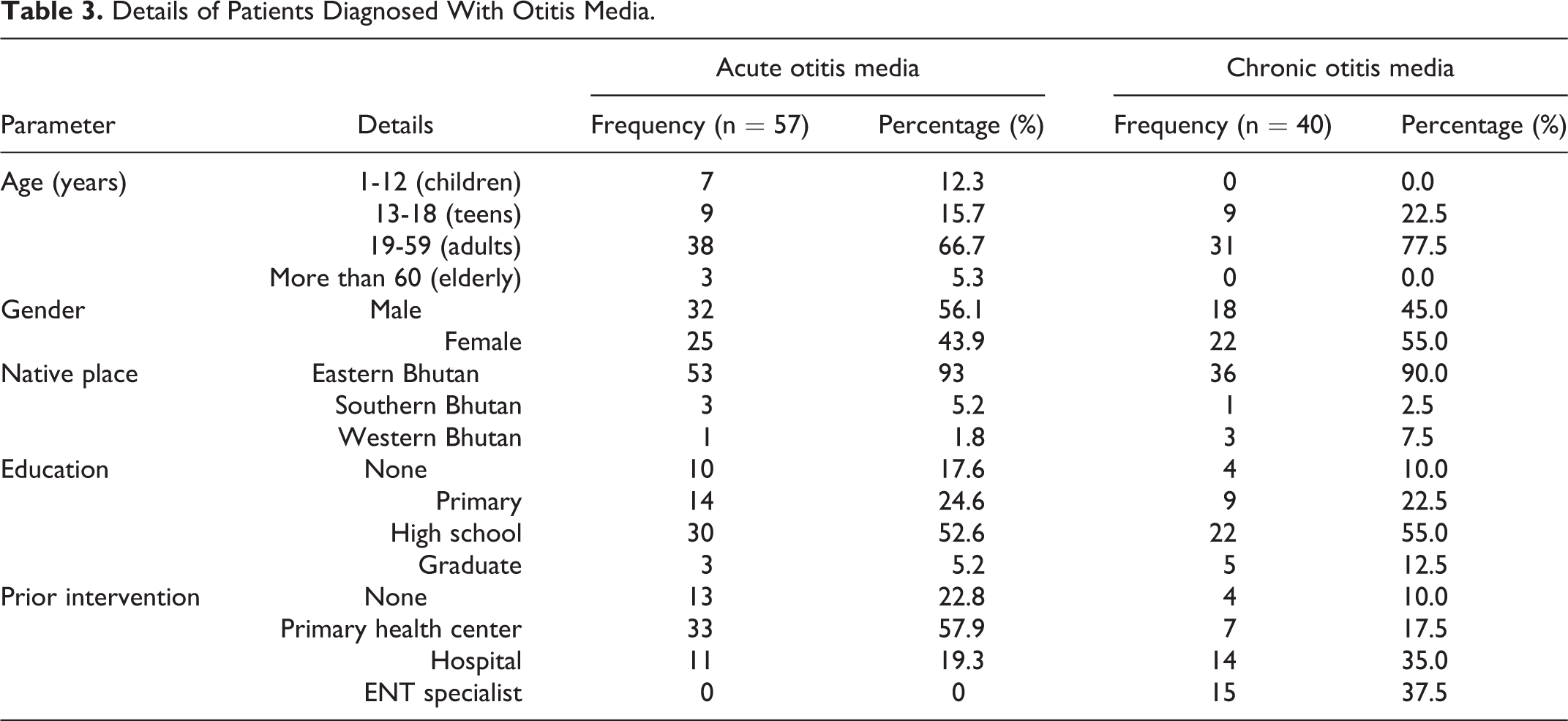
In children, AOM was more common (n = 7; 12.3%) compared to nil COM. None of the patients with AOM had received specialist care, whereas 37.5% of patients with COM sought ENT specialist care.
Surgical intervention was planned for 45 patients; however, 2 patients with COM refused and ultimately, 43 patients underwent surgery; 88.4% of the operated cases were COM and underwent tympanoplasty type I alone. Two patients underwent tympanomastoidectomy for cholesteatoma and 2 patients comprising of aural polyp and sebaceous cyst each underwent excision. One patient had preauricular abscess who underwent incision and drainage. Follow-up was classified as complete when the patient reported as advised on all 3 visits during 1 day, 6 weeks, and 2 months after the surgery. If the patient missed even one scheduled visit, it was classified as incomplete. Tables 4 and 5 show details of the operated cases and tympanoplasty cases, respectively.
Operated Cases.
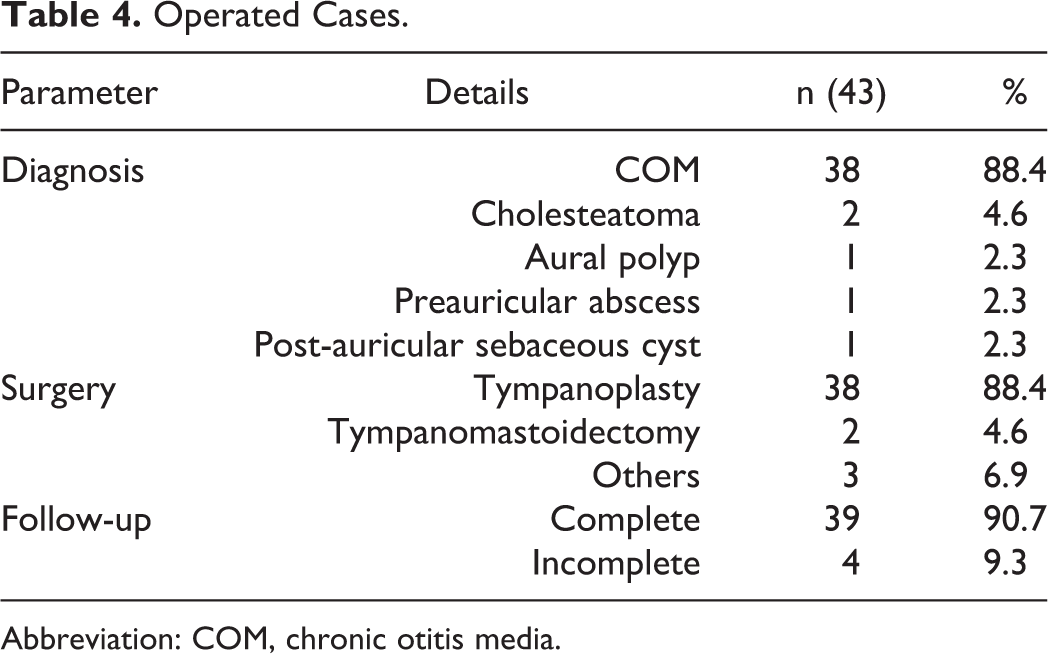
Abbreviation: COM, chronic otitis media.
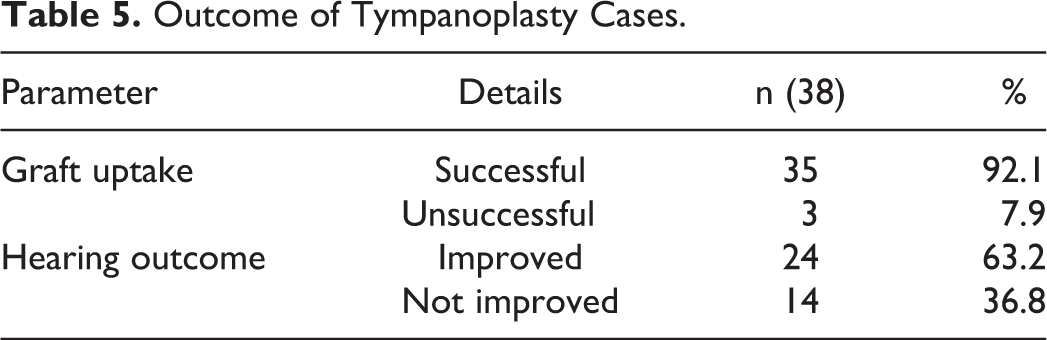
Outcome of Tympanoplasty Cases.
All the 43 operated patients came for day 1 follow-up and none had wound complications or facial palsy. Two of them complained of significant pain.
By 6 weeks postoperatively, only 40 of the 43 patients showed up for follow-up. They did not have any significant complications such as wound dehiscence, otorrhoea, and all tympanoplasty cases were observed to have good graft uptake.
By 2 months, 3 patients did not come for follow-up. The 40 patients who could be followed up did not have any major complications such as otorrhoea, wound complications but 3 patients had tympanic membrane graft perforation. Graft uptake was successful in 35 (92.1%) patients. A pure tone audiogram was done on patients who had undergone tympanoplasty during the 2-month review; 24 (63.2%) patients showed improvement in hearing. Follow-up completion rate was 90.7%.
Discussion
In the present study, we determined the outcomes of ear camp conducted by Thai Rural ENT Foundation at Monggar ERRH from January 6, 2019, January 8, 2019, and explored the spectrum of cases seen, the interventions done and outcomes of surgery in terms of tympanic membrane closure, absence of otorrhoea, and improvement in hearing. This is the first such study to be conducted in Bhutan.
Medical and surgical interventions were provided to 210 people with ear-related illnesses. Additional 335 people were also examined for nose and throat–related disorders and necessary medical advice given. The actual notification communicated between the visiting team and Bhutan’s Health Ministry was to register ear-related cases but people with other ENT illnesses had also come for consultation. This may have been due to miscommunication or perhaps due to perceived better service of previous Thai ear camps.
The camp happened during the winter season in eastern Bhutan. Due to extreme weather conditions, the team was one day late to arrive at the destination. The ear camp that was supposed to take place from January 5 to January 8 could do so from January 6 to January 8 thus losing one day of the camp due to the aforementioned reason. This was an inconvenience not just for the visiting team but also for the patients who were awaiting the team’s arrival. Better logistical arrangements and venue selection keeping in mind the target population and road conditions could enable satisfactory conduct of such mobile surgical camps in future.
Most of the study participants were adults in the age group of 19 to 59 years, and gender distribution was almost the same. The majority of the patients were from eastern Bhutan which can be explained by the fact that they were mostly from the region where the ear camp was conducted.
Otitis media was the commonest illness found among the study population which was the same as stated during previous Thai ear camp in Bhutan. 7,11,13,14,16 Research findings on the risk factors of otitis media among Bhutanese population are not available but the high incidence in our study could be attributed to the rural population where access to ENT care is difficult. 9 The habit of not following precautions to avoid water entry in ear like using cotton earplugs in cases of infection could be the cause for recurrent or persistent ear discharge. 11 Poor nutrition, unhygienic living conditions, and the habit of scratching ears with matchsticks, twigs, and feathers might lead to different ear infections such as otitis externa, traumatic tympanic perforation, and otomycosis. 12,15
Acute otitis media is usually more common among children as stated in other studies carried out in the region 17,18 but in our study, it was found more in adults. This could be attributed to adults representing the major portion of patients who came to seek medical consultation during this camp. Since it was winter season when the camp took place, may be it was inconvenient for the parents to bring their children for review.
The commonest intervention given was oral and/or topical antibiotics and surgical intervention was done on 43 patients. Since the commonest illness requiring surgery was COM, so was tympanoplasty the commonest surgery. Postoperative wound hematoma was not observed on any patients.
We had a tympanic membrane closure rate of 92.1% which was similar to studies done in Thailand 8 and even better than those reported in Namibia 19 and Mexico. 20 This can be attributed to the good surgical skills of experienced surgeons and good postoperative compliance by the patients. It can also be due to the standard of infection control observed for the surgical instruments and the operating room. All sets of surgical instruments, gowns, and drapes were brought sterilized from Bangkok, Thailand. Moreover, Monggar hospital is a tertiary-level hospital following the Bhutan Health Care Standard for Quality Assurance endorsed by MoH and Bhutan Standard Bureau.
The patients’ hearing improvement rate of 63.2% was not as high as their tympanic membrane perforation closure rate and was also lower than those reported by other studies. 8,17 This could have been influenced by other factors such as undetected ossicular chain discontinuity or fixation. Those patients who had good tympanic membrane graft uptake but no significant hearing improvement could benefit from ossiculoplasty or hearing aids.
We wanted to see whether patients who were previously seen by doctors had better surgical outcomes than those who had availed medical care from primary centers. There was no statistically significant corelation between prior intervention to the surgical outcome in terms of tympanic membrane closure and improvement in hearing. The surgical outcome could be affected by not just clinician factors but also other patient factors such as hygiene, nutrition, and compliance to medications and advice.
A limitation of this study was that all the operated patients did not have a complete follow-up of 3 occasions as planned. Although a follow-up completion rate of 90.7% can be considered satisfactory, complete follow-up data could not be assessed from 4 (9.3%) patients; 2 of them were tympanomastoidectomy cases, 1 had undergone aural polyp excision, and 1 had done incision and drainage of preauricular abscess. This could have affected the statistical analysis. The contact numbers provided by them during the ear camp could not be traced and hence, there was some form of attrition bias in this way. The importance of patient commitment to treatment cannot be stressed enough. Better compliance to follow-up is necessary not just in terms of data collection for research purposes but for the patients’ sake more importantly.
The follow-up period, at 2 months, was also short compared with that reported by other studies (eg, more than a year). Our patients’ success rates may possibly have reduced after 6 months, because all causative factors in our patients’ chronic ear diseases could not be corrected. Further studies of the long-term outcomes of mobile ear surgery units may be required.
Furthermore, this study represents findings from just one region of Bhutan carried out at one point in time. Similar studies of other ear camps in other districts need to be done to get more data about the pattern of ear disease in the entire kingdom.
Conclusion
The MOH of the Royal Government of Bhutan in close collaboration with the Royal Kingdom of Thailand has been cooperating in the field of medicine among others since formal diplomatic relations were established way back in 1989 so that patients visiting every referral hospital and major district hospitals can be screened and avail their services during ear camps. 21 The Monggar Hospital ear camp had good ear surgery outcomes, in terms of tympanoplasty closure, absence of otorrhoea, and hearing improvement. The mobile ear surgery unit is a useful venture for a developing country like Bhutan and especially for remote populations with limited access to health services.
Footnotes
Acknowledgments
The authors could like the convey our heartfelt appreciation to the Thai Rural ENT Foundation and Thai Red Cross Society for being important source of medical expertise for a developing nation like Bhutan and to its citizens who have been benefitting immensely from their mobile ear camps. Immense gratitude goes to Dr Paninee Charusripan, team leader and all the visiting surgeons, nurses and supporting staffs of the eighth Thai Medical Mission to Bhutan for their selfless service to the people of Bhutan. This study could not have been done without the guidance of Dr Pornake Apipan, Dr Phakdee Sannikorn, and all the staffs of Center of Excellence in ENT/Head and Neck Surgery of Rajavithi Hospital, and hence, they are worthy of distinctive mention. Special mention also goes to the doctors, nurses and technicians from Bhutan who helped during the data collection. Finally, we convey huge gratitude to all the study participants for consenting to be a part of this study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.