
Abstract
Papillary thyroid carcinoma (PTC) is the most frequent thyroid malignancy. Intraparotid recurrence of PTC is, however, rare. Most parotid malignancies are either primary or metastatic from cancer outside the head and neck. We report a case of a 71-year-old man who had undergone lobectomy and completion thyroidectomy for PTC and presented to our clinic with an insidious intraparotid recurrence, for which he underwent a superficial parotidectomy and radioactive iodine therapy. We also present a review of the literature on similar cases. Intraparotid metastasis of PTC should be considered in the differential diagnosis of a parotid mass.
Introduction
The incidence of papillary thyroid carcinoma (PTC) from 1975 to 2012 increased from 4.8 to 13.3 per 100 000. 1 Papillary thyroid carcinoma is the most frequent type of thyroid carcinoma encountered. Lymph node (LN) metastasis occurs in up to 80% of PTC cases, depending on the extent of surgery. 2 Distal metastasis, however, is uncommon and occurs at a rate of 2% to 10%. 1
Residual involved LNs are the most common source of disease recurrence. 3 One-third of PTC will recur following initial treatment. 4,5 A nonstimulated thyroglobulin level of ≥5 ng/mL following total thyroidectomy or ≥30 ng/mL following lobectomy should prompt further investigation of recurrent disease. 3
Metastasis from thyroid carcinomas to the parotid gland is exceptionally rare. 6 Fine needle aspiration (FNA) of 184 secondary salivary gland malignancies (171 parotid and 13 submandibular glands) revealed that more than 80% originated from either squamous cell carcinoma or malignant melanoma. 7
Case Report
A 71-year-old man presented to the otolaryngology clinic in August 2020 with swelling at the angle of the right side of his jaw that had been present for 4 months. The swelling was neither painful nor itchy and was barely noticeable. The patient had no weight loss.
Clinical examination revealed a smooth, nontender, 1.5 × 1.5 cm mass fixed in parotid gland substance. Findings from examination of the patient’s ear, nose, and throat were normal. There was no palpable cervical LN, facial asymmetry, or weakness in his facial muscles.
The patient had undergone a left thyroid lobectomy with left neck dissection 15 years prior to this presentation at a different institution. Following surgery, he developed hematoma and respiratory distress for which he underwent a tracheostomy tube insertion. The tracheostomy was removed soon afterward.
In March 2019, he presented to our clinic with a 3-year history of another painless thyroid mass. The mass grew progressively to become very large. Clinical examination revealed a 5 × 6 cm nontender and irregular thyroid mass involving levels II and III and the posterior triangle. We performed a completion thyroidectomy with right neck dissection. Histopathological examination revealed classic PTC. The patient received radioactive iodine following surgery.
A computed tomography (CT) scan was performed on the intraparotid mass, and thyroglobulin levels were determined (Figures 1 and 2). The CT scan showed a 1-cm enhancing mass within the parotid gland. The patient’s thyroglobulin levels were checked periodically after the completion thyroidectomy and were decreasing over time.
The patient underwent a right superficial parotidectomy. The histopathological report indicated 7 intraparotid LNs and 2 LNs in adipose tissue. All of the intraparotid LNs and 1 of the 2 LNs in adipose tissue were positive for metastatic PTC (Figure 3). The patient is preparing to undergo radioactive iodine therapy.

Contrast-enhanced computed tomography image of the neck shows an asymmetrical appearance of the parotid gland with mild swelling of the right gland associated with a small contrast-enhanced intraglandular lesion measuring around 1.0 cm located at the inferior and posterior margin of the gland.
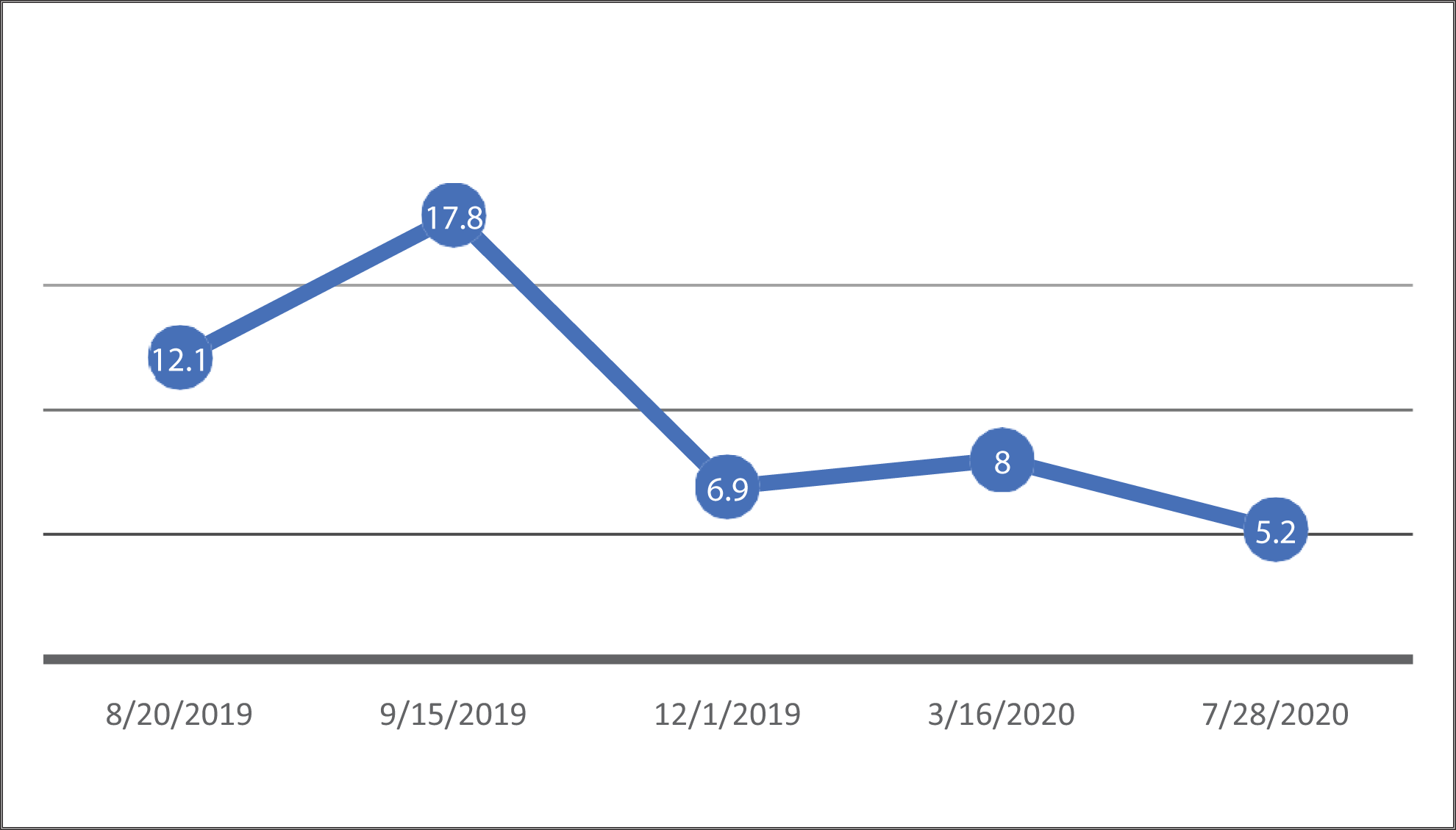
Graphic presentation of patient’s thyroglobulin levels across time (ng/mL).
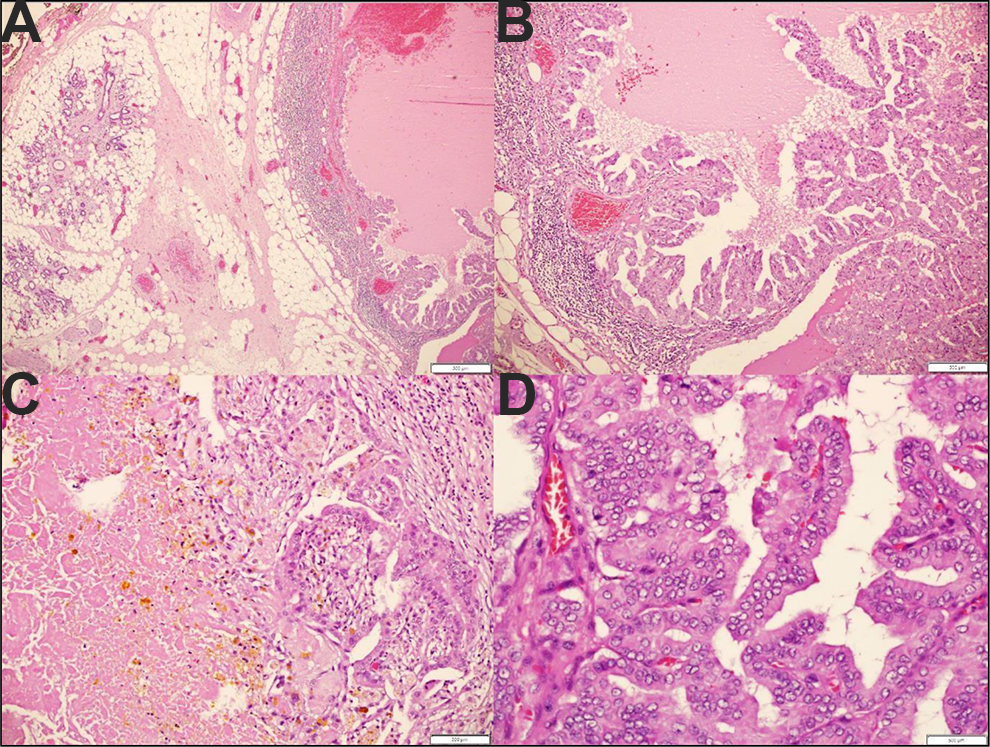
(A) A lymph node with metastatic papillary thyroid carcinoma (right) adjacent to uninvolved salivary gland tissue (left). (B) Papillary architecture in the same lymph node from image (A). (C) Tumor with necrotic material and pigmentation in a different intraparotid lymph node. (D) Characteristic features of papillary thyroid carcinoma, such as papillary architecture, cellular crowding, nuclear clearing, and grooves. The intranuclear pseudo inclusion is difficult to appreciate.
Review of the Literature
A review of the literature showed 7 other cases of PTC presenting as a parotid mass. 8 -14 The mean age was 62.7 years and all patients were older than 60, except for one who was 45 at presentation. The majority of these patients (4 of 7) had a previous history of PTC, and an intraparotid mass presented as a recurrence. Most cases were investigated by CT scanning of the parotid gland and FNA. All except 2 patients were treated surgically. Other details are shown in Table 1.
Reported Intraparotid Metastasis of Papillary Thyroid Carcinoma (PTC) Cases in the Literature.
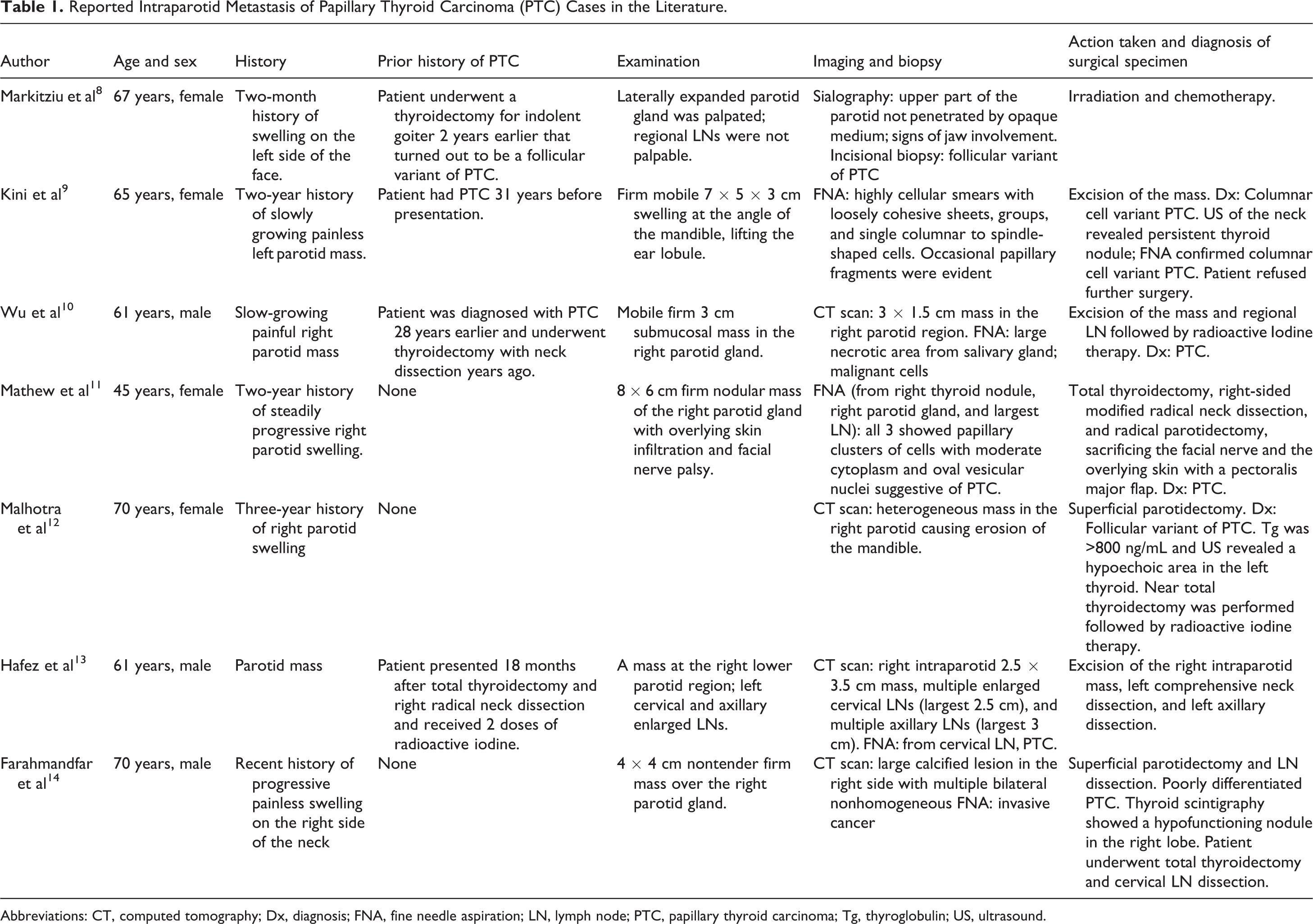
Abbreviations: CT, computed tomography; Dx, diagnosis; FNA, fine needle aspiration; LN, lymph node; PTC, papillary thyroid carcinoma; Tg, thyroglobulin; US, ultrasound.
Discussion
Most carcinomas derived from the follicular epithelium of the thyroid gland are well-differentiated (90%), with a 10-year disease-specific survival rate of 85% to 92%. 15 Distance metastasis decreases the 10-year survival rate to 10% to 40%. 16,17 Local and distant metastases of classic PTC mainly occur in the regional LNs, lung, and bones. 6 Although a rare occurrence, PTC has been described in case reports to metastasize to ectopic locations outside the central and lateral neck compartments. 18 The ectopic locations include retropharyngeal, parapharyngeal, sublingual, and axillary locations. 19
Published data by Goyal et al 19 showed that macroscopic nodes primarily reside in the central neck at initial surgery, with no ectopic nodes at initial presentation. In the recurrence setting, lateral neck nodes predominate and there is a 9% rate of ectopic nodal metastasis. Metastasis of PTC to the parotid gland occurs by retrograde extension through lymphatic channels, which might also be involved by direct invasion. 20,21
Although this case report and review of the literature emphasizes the importance of considering PTC in the differential diagnosis of a parotid mass, primary parotid tumors and metastasis from a more anatomically distant site should not be overlooked. With the exception of scalp and ear melanoma, parotid metastasis from a primary site in the head and neck is uncommon. 7
We advocate performing a careful history and physical examination of the patient. Fine needle aspiration and imaging of parotid masses are useful tools for distinguishing primary from metastatic disease. 22
Despite our patient having undergone a completion thyroidectomy with neck dissection and receiving radioactive iodine, and despite his decreasing levels of thyroglobulin, he developed a parotid recurrence of PTC. Regarding the histological subtype, our patient had a classic PTC variant similar to some of the reported cases in the literature, as shown in Table 1.
Conclusion
Decreasing thyroglobulin levels alone should not rule out PTC recurrence. Papillary thyroid carcinoma recurrence or metastasis should be considered in the differential diagnosis of a parotid malignancy of unknown primary cancer. Most cases are treated by surgical excision.
Supplemental Material
Supplemental Material, sj-pdf-1-ear-10.1177_01455613211033124 - Intraparotid Recurrence of Papillary Thyroid Carcinoma After Thyroidectomy Coincident With Declining Thyroglobulin Levels: A Case Report and Review of the Literature
Supplemental Material, sj-pdf-1-ear-10.1177_01455613211033124 for Intraparotid Recurrence of Papillary Thyroid Carcinoma After Thyroidectomy Coincident With Declining Thyroglobulin Levels: A Case Report and Review of the Literature by Azmi Marouf, John C. Heaphy, Abdullah Mohammed Sindi, Ahlam Hadi Alamri, Firas R. Abi Sheffah, Ahmed Noorsaeed, Anas H. Al-Tammas and Bilal Issa Rammal in Ear, Nose & Throat Journal
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.