
Abstract
Objective:
Lateral neck dissection (LND) is important in managing papillary thyroid carcinomas (PTCs). This study aimed to evaluate the relationship between lymph node yield (LNY) for LND and patient outcomes, specifically postoperative serum thyroglobulin levels (sTG) and radioiodine uptake on thyroid scan, and to estimate a threshold LNY to signify adequate LND.
Methods:
Patients diagnosed with PTC who underwent LND from 2006 to 2015 at a single institution were included. Linear regression with restricted cubic splines was used to characterize the association of LNY with outcomes. Outcomes were log-transformed to achieve a more symmetric distribution prior to regression. For nonlinear associations, a Monte Carlo Markov Chain procedure was used to estimate a threshold LNY associated with postoperative outcome. This threshold was then used to define high LNY versus low LNY in the subsequent analyses.
Results:
In total, 107 adult patients were included. There was a significant relationship between LNY and postoperative sTG level (P = .004), but not radioiodine uptake (P = .64). An LNY of 42.96 was identified, which was associated with the maximum change in sTG level. No association was found between LNY groups (LNY ≥ 43 vs < 43) and radioiodine uptake, risk of complication, or longer operative times (all P > .05). High LNY was associated with a decrease in log(sTG) (estimate = −1.855, P = .03), indicating that adequacy of LND is associated with an 84.4% decrease in sTG.
Conclusion:
These results suggest an association between LNY and postoperative sTG level, with an estimated threshold of 43 nodes. This has implications for adequate therapeutic LND; additional work is needed to validate thresholds for clinical practice.
Keywords
Background
Papillary thyroid carcinomas (PTCs) constitute over 80% of diagnosed thyroid malignancies. 1 Adequate surgery remains the most important prognostic factor for the management of PTC, although other therapies such as radioactive iodine (RAI) and thyroid-stimulating hormone suppression have important adjuvant roles in some patients. 2 Despite having an excellent prognosis with a 10-year survival rate for overall differentiated thyroid cancer ranging between 87% and 94%, 3 PTC frequently tends to spread to cervical lymph nodes. Several clinical studies showed that papillary carcinomas and even microcarcinomas have a high incidence of lymph node metastasis and recurrence.4,5 It has been reported that 60% of PTC patients present initially with lymph node metastasis 6 and that cervical recurrence in PTC after initial treatment occurs in up to 30% of patients. 7 The 2015 revised American Thyroid Association guidelines recommend that lateral neck dissection (LND) should be performed for patients with biopsy-proven lateral cervical metastasis detected clinically. 8 The number of lymph nodes removed has been shown to be an important prognostic factor in a number of cancers including breast, 9 colorectal, 10 and esophageal. 11 Postoperative sTG levels and RAI uptake on thyroid scan have been shown to correlate with persistent disease 12 and could potentially be used as surrogate markers for the completeness of LND in patients with PTC. In this study, we explore the effect of lymph node yield (LNY) on these surrogate markers of PTC disease burden.
Materials and Methods
Approval for this study was obtained from the Duke University Medical Center Institutional Review Board. Adult PTC patients who underwent an LND at Duke University Hospital between 2006 and 2015 were included in this study. Patients with prior LND for unrelated disease, prior external radiation to the neck, and those with concurrent malignancies were excluded. Retrospective chart review was performed to collect patient and pathologic specimen characteristics, as well as sTG and RAI levels. The distributions of sTG and RAI uptake were examined, and a log-transformation was applied to sTG level to achieve a more normal distribution. Lymph node yield was defined as a total raw count of lymph nodes removed for patients who underwent a unilateral neck dissection, and one-half (1/2) of the total raw count of lymph nodes removed for patients who underwent a bilateral neck dissection. Postoperative stimulated thyroglobulin levels were measured 4 to 8 weeks after surgery, typically at the time of thyroid scan. If the scan was not performed, levels were taken at 30 days or more after surgery.
Analysis of LNY
Separate multivariate linear regression models with restricted cubic splines (RCS) were used to characterize the functional association of log(sTG) and RAI uptake with LNY, after adjustment for age, gender, body mass index (BMI), hypertension, hyperlipidemia, tumor size, and family history of thyroid cancer, and a univariate logistic regression model with RCS was used to characterize the functional association of odds of complication with LNY. This model was limited to univariate due to a small number of patients experiencing complications. The RCS methodology allows for the functional relationship between a continuous variable and an outcome to be examined, without prior knowledge of the shape of the association. 13 Three-, 4-, and 5-knot models were examined and the model with the lowest Akaike information criterion (AIC) was chosen. AIC is a measure of model fit, with smaller values indicating a better fit to the data. Knots were placed as recommended by the literature. 14 The RCS method also allows for testing of linearity of the functional association. A significant nonlinear association P-value indicates that the association is nonlinear and should be modeled with this taken into account. If found to have a nonlinear relationship, it is appropriate to estimate a threshold value. When appropriate, a threshold was estimated using a Monte Carlo Markov Chain procedure that assumed a multivariate normal distribution, with possible threshold range determined by visual inspection of the associated RCS curve. In this study, only log(sTG) exhibited a nonlinear association with LNY. An LNY of 42.96 was estimated as the point within the prespecified range that was associated with the maximum change in log(sTG). Based on this value, 2 study groups were defined: low LNY (LNY < 43) and high LNY (LNY ≥ 43).
Effects of LNY in LND
Patient characteristics were summarized with N (%) for categorical variables and median (interquartile range, IQR) for continuous variables for all patients and by the adequacy of lymph node dissection. Differences were tested using the Wilcoxon Rank Sum test for continuous variables and the χ2 or Fisher exact test for categorical variables, as appropriate. Multivariate linear regression models were used to estimate the effect of low LNY versus high LNY on log(sTG) and RAI uptake. Multivariate linear regression was also used to estimate the association of continuous LNY with RAI uptake. Univariate logistic regression models were used to estimate the association of low LNY versus high LNY and continuous LNY on odds of complication. Negative binomial models were used to account for the skewed nature of operative time and to estimate the effect of LNY group on operative time based on the threshold identified above (data not shown, available upon reviewer’s request).
Only patients with available data for all covariates were included in each analysis and effective sample sizes are included for each table/figure. No adjustments were made for multiple comparisons. All statistical analyses were conducted using SAS version 9.4 (SAS Institute).
Results
Population Demographics
One hundred and seven patients fulfilled our inclusion criteria (Figure 1). The median age at the time of neck dissection was 41 (IQR 30-52.5). The sample was predominantly female (66.4%). The median tumor size was 2.2 cm (IQR 1.2-3.5), and the median LNY was 24 (IQR 16-32; Table 1). Only 14 patients experienced a postoperative complication with recurrent laryngeal nerve injury (n = 8) being the most common followed by chyle leak (n = 4) and Horner’s syndrome (n = 2).
Patients consort diagram.
Patient Characteristics.
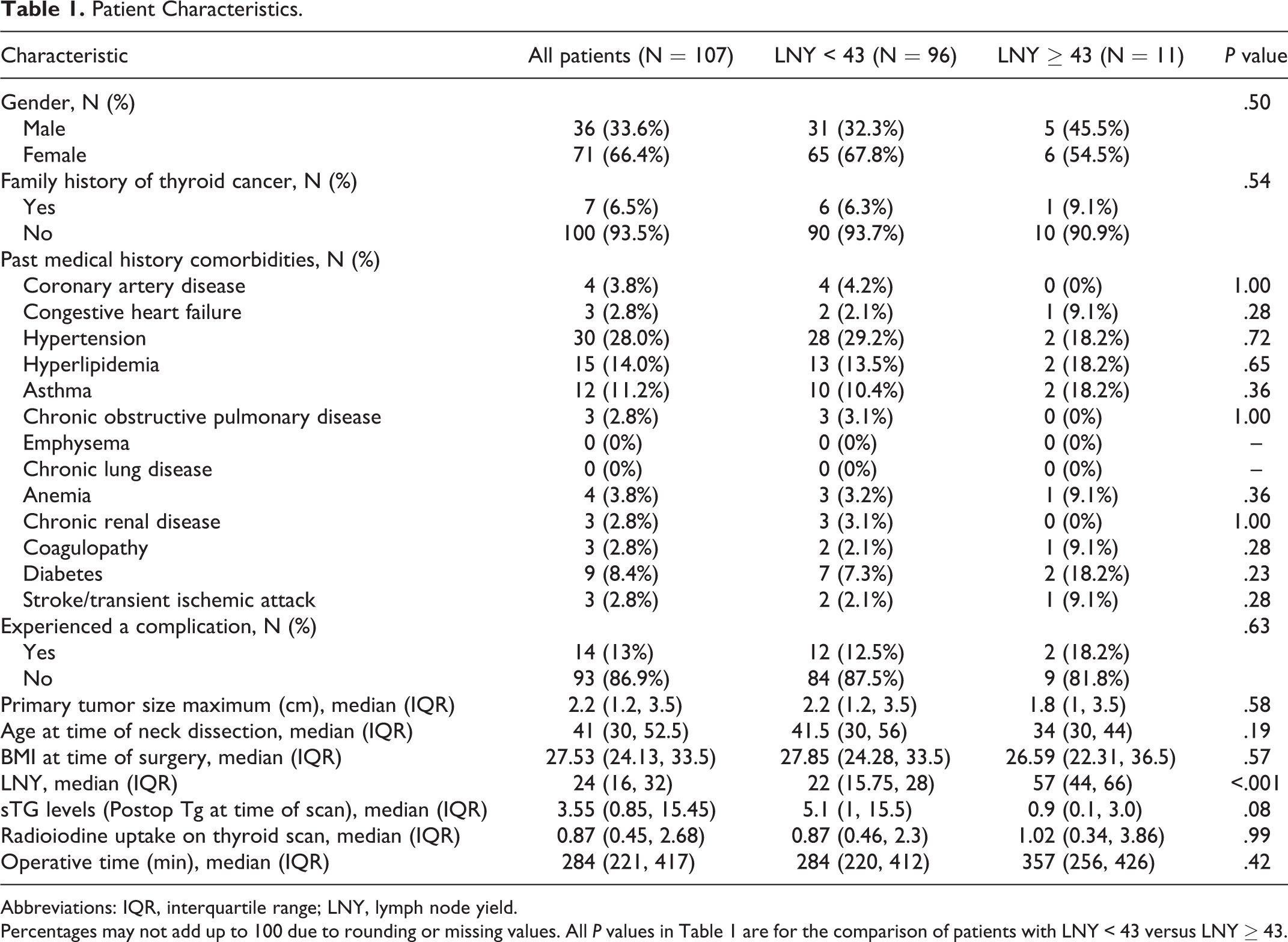
Abbreviations: IQR, interquartile range; LNY, lymph node yield.
Percentages may not add up to 100 due to rounding or missing values. All P values in Table 1 are for the comparison of patients with LNY < 43 versus LNY ≥ 43.
Restricted Cubic Spline Analysis
For the adjusted linear regression model with RCS estimating the functional association of log(sTG) with LNY, a 4-knot model was selected based on the lowest AIC (3-knot AIC = 249.51, 4-knot AIC = 244.37, and 5-knot AIC = 246.24; Figure 2). Based on statistical literature, knots were placed at the 5th, 25th, 75th, and 95th percentiles of the distribution of LNY. A nonlinear association was identified between log(sTG) and LNY (P = .004). For the adjusted linear regression model with RCS estimating the functional association of RAI uptake with LNY, a 3-knot model was selected based on the lowest AIC (3-knot AIC = 300.73, 4-knot AIC = 302.72, 5-knot AIC = 301.04), and knots were placed at the 5th, 50th, and 95th percentiles (Figure 3). A nonlinear association was not identified between RAI uptake and LNY (P = .64). For the unadjusted logistic regression model with RCS estimating the functional association of odds of complication with LNY, a 3-knot model was selected (3-knot AIC = 88.29, 4-knot AIC = 89.53, 5-knot AIC = 90.00) with knots placed at the 5th, 50th, and 95th percentiles (Figure 4). A nonlinear association was not identified between odds of complication and LNY (P = .56).
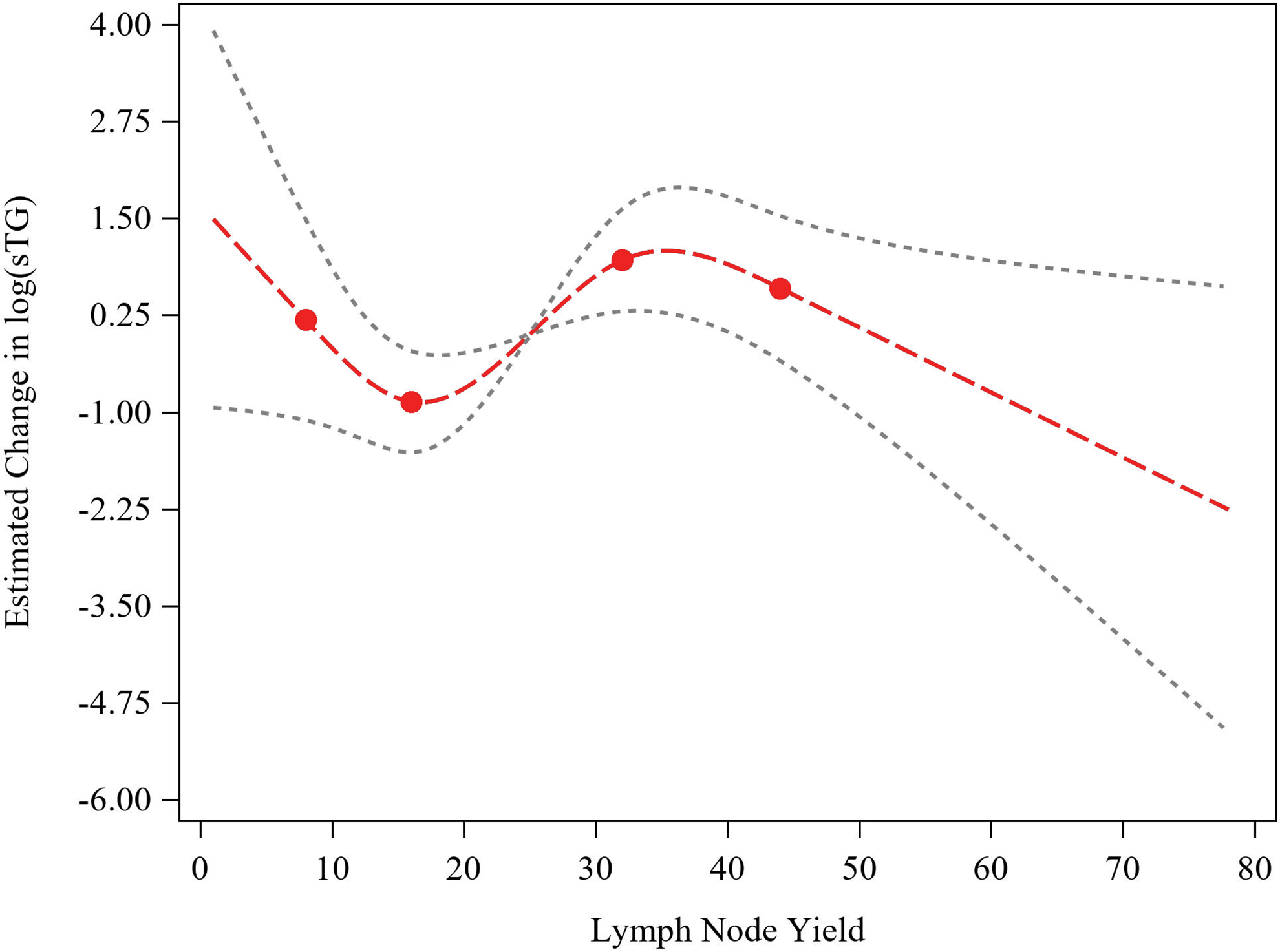
Linear regression model with restricted cubic splines for LNY on log(sTG), after adjustment for age, gender, BMI, hypertension, hyperlipidemia, tumor size, and family history of thyroid cancer (N = 56). Red curve indicates restricted cubic spline fit, black dashed lines indicate confidence limits for fitted line, and red dots indicate knots placed at the 5th, 25th, 75th, and 95th percentiles of the distribution of LNY. The median LNY was used as reference to estimate the change in log(sTG). BMI, body mass index; LNY, lymph node yield.
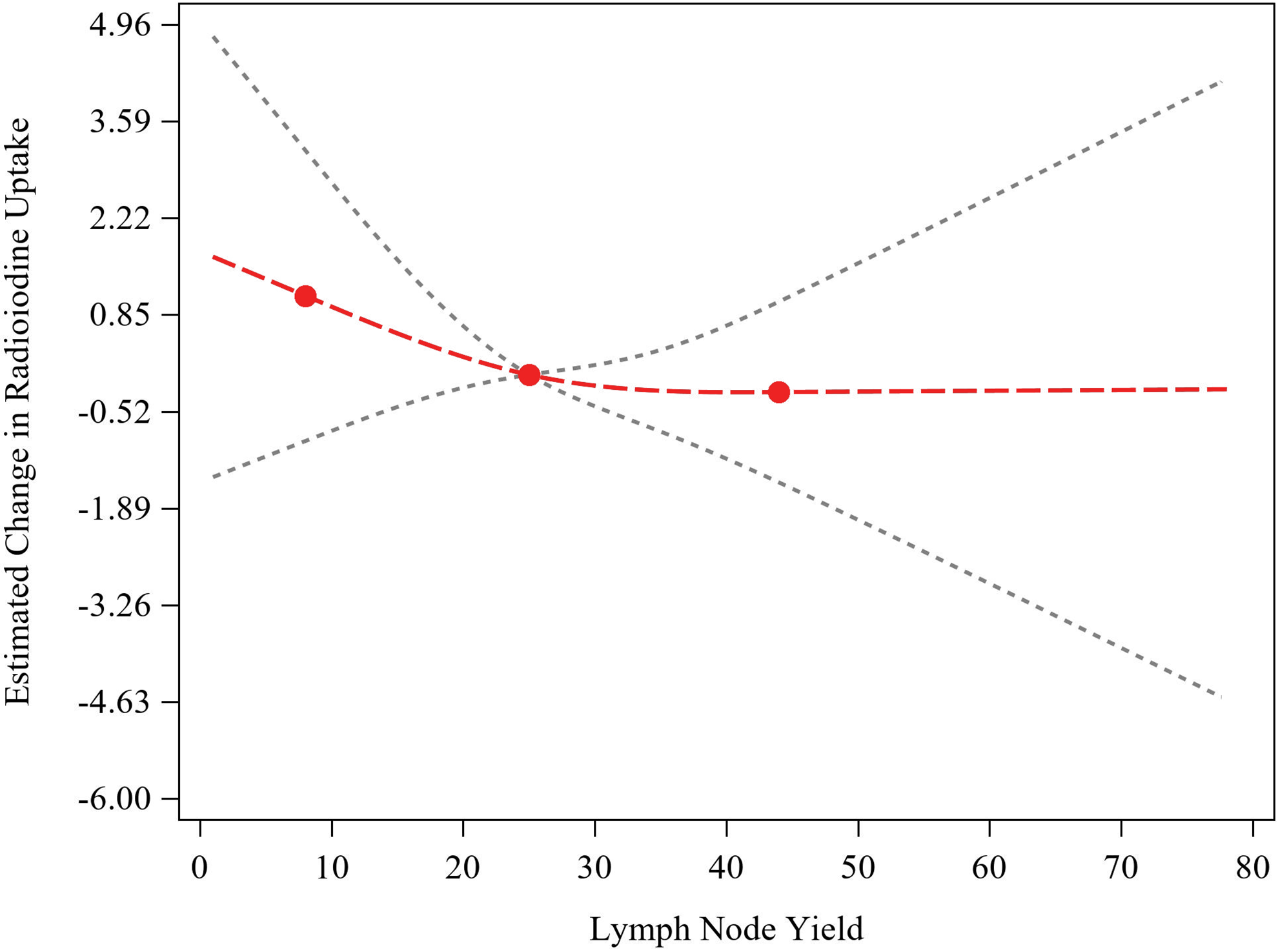
Linear regression model with restricted cubic splines for LNY on radioiodine uptake, after adjustment for age, gender, BMI, hypertension, hyperlipidemia, tumor size, and family history of thyroid cancer (N = 56). Red curve indicates restricted cubic spline fit, black dashed lines indicate confidence limits for fitted line, and red dots indicate knots placed at the 5th, 50th, and 95th percentiles of the distribution of LNY. The median LNY was used as reference to estimate the change in radioiodine uptake. BMI, body mass index; LNY, lymph node yield.
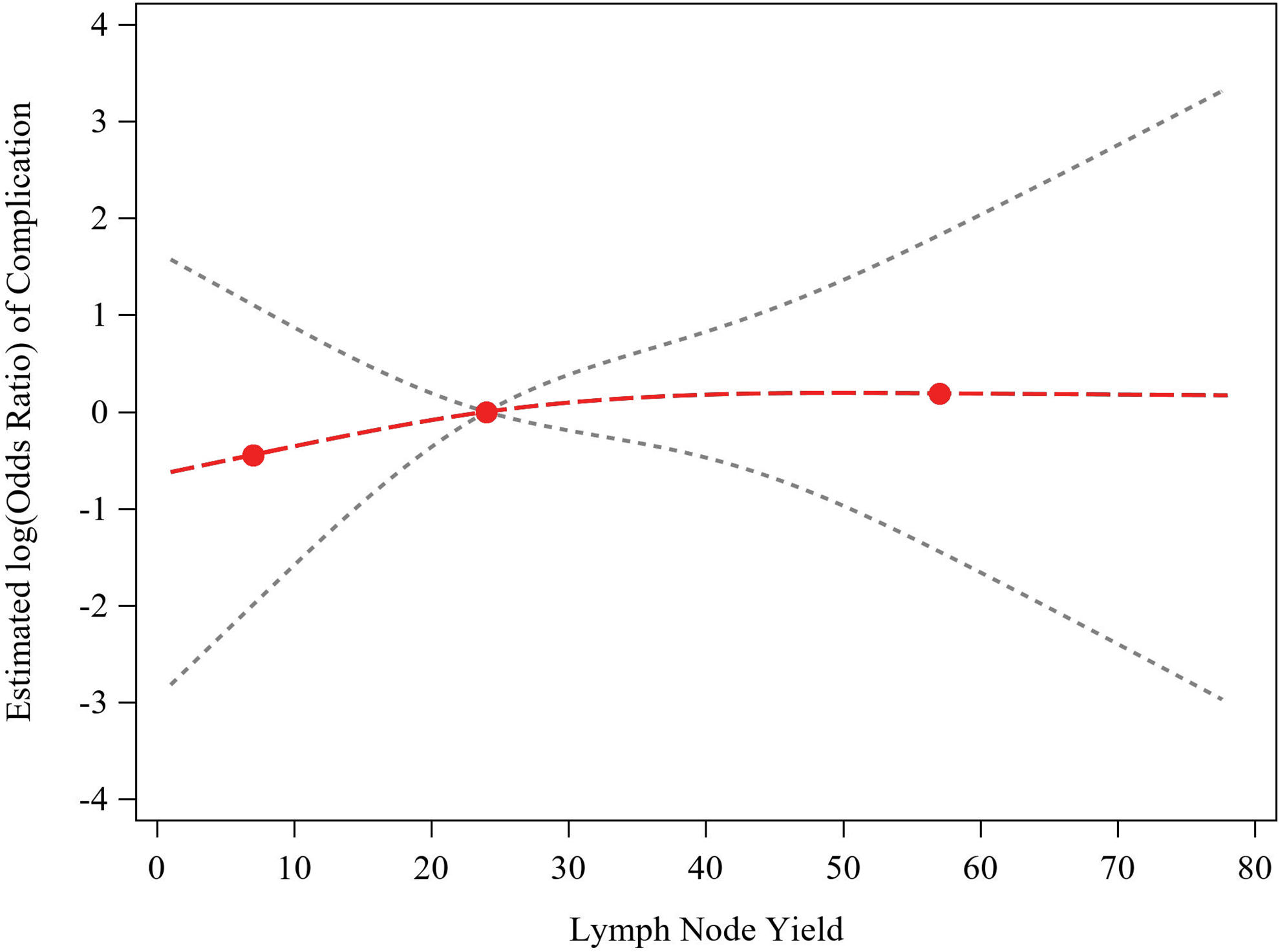
Logistic regression model with restricted cubic splines for LNY on odds of complication (N = 107). Red curve indicates restricted cubic spline fit, black dashed lines indicate confidence limits for fitted line, and red dots indicate knots placed at the 5th, 50th, and 95th percentiles of the distribution of LNY. The median LNY was used as a reference to estimate the log (odds ratio) of complication. LNY, lymph node yield.
Lateral Neck Dissection
In our cohort, 24 patients presented with at least one positive lymph node on the contralateral side of the lateral neck detected either by fine-needle aspiration or by imaging and underwent a bilateral LND. As previously reported, patients who had an LNY ≥ 43 were categorized as having a high LNY and those with LNY < 43 as a low LNY. The majority had a low LNY (N = 96, 89.7%), whereas only 11 (10.3%) patients had a high LNY. The patients in the 2 LNY groups did not differ in age, gender, comorbidities, operative time, or tumor size. Using a linear regression model (Table 2), a high LNY was associated with a lower log(sTG; estimate = −1.855 [95% confidence interval −3.482, −0.228], P = .03), translating to a decrease of 84.4%, whereas age, gender, hyperlipidemia, and family history of thyroid cancer were not associated with log(sTG). No association was found between RAI uptake and LNY group (P = .93; Table 3A) or LNY as a continuous variable (P = .38; Table 3B). Other predictors such as age, BMI, and tumor size were also not associated with RAI uptake. Similarly, no association was found between odds of complication and LNY group (P = .60) or LNY as a continuous variable (P = .52; data not shown, available upon reviewer’s request).
Linear Regression Model for LNY Group on Log(sTG; N = 56).
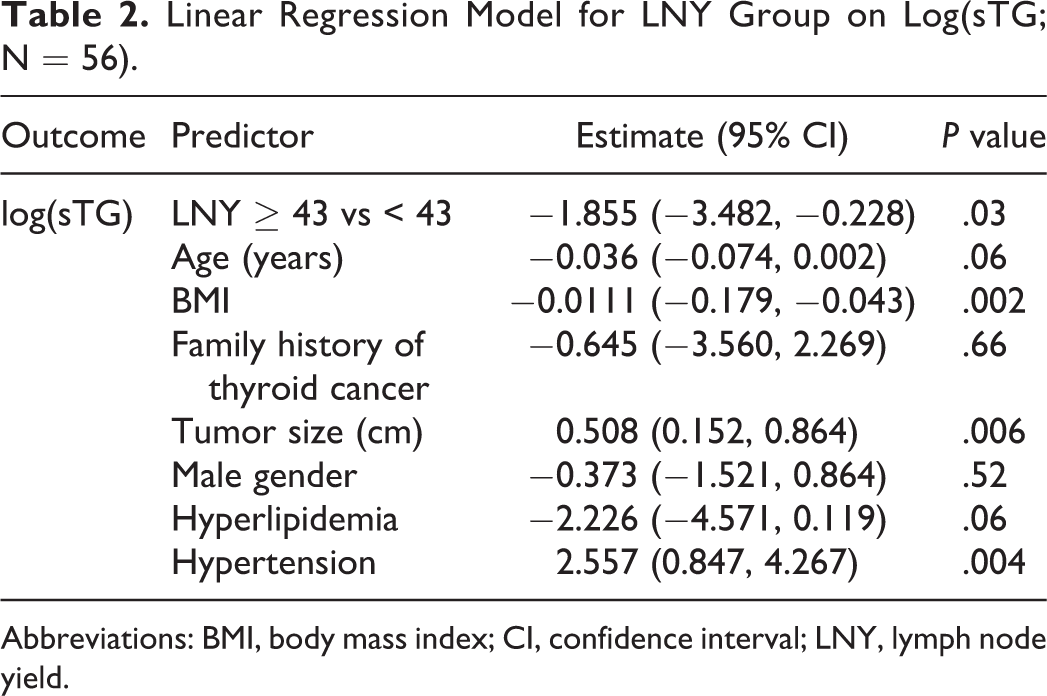
Abbreviations: BMI, body mass index; CI, confidence interval; LNY, lymph node yield.
Linear Regression Model for LNY on Radioiodine Uptake (N = 56).
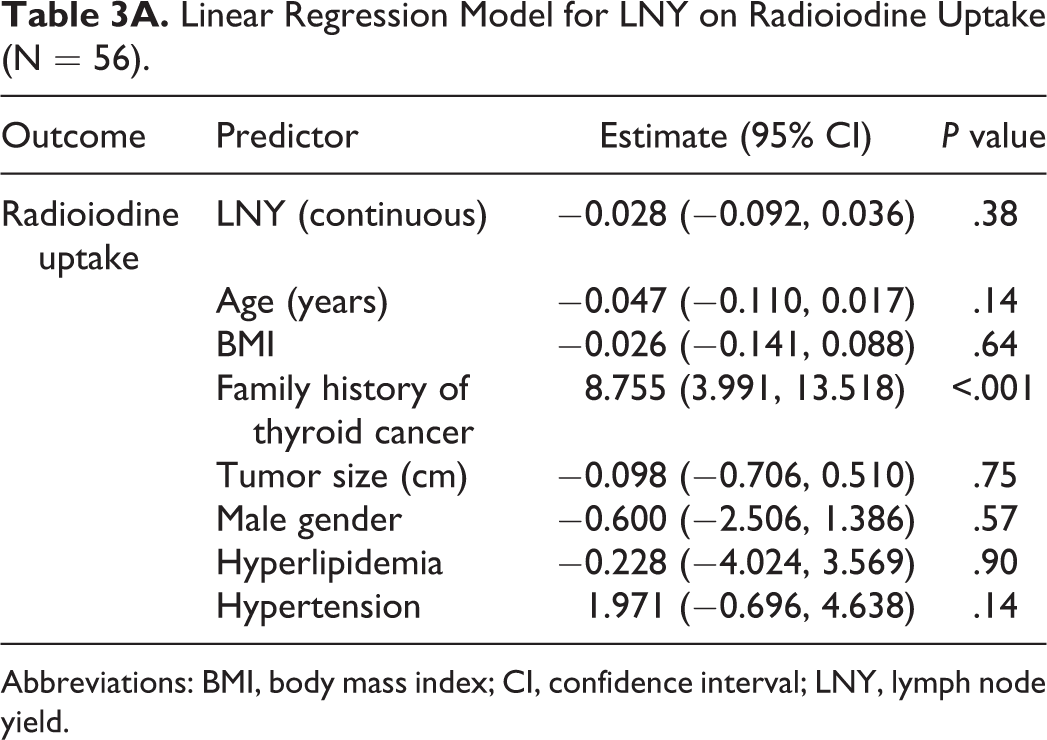
Abbreviations: BMI, body mass index; CI, confidence interval; LNY, lymph node yield.
Linear Regression Model for LNY Group on Radioiodine Uptake (N = 56).
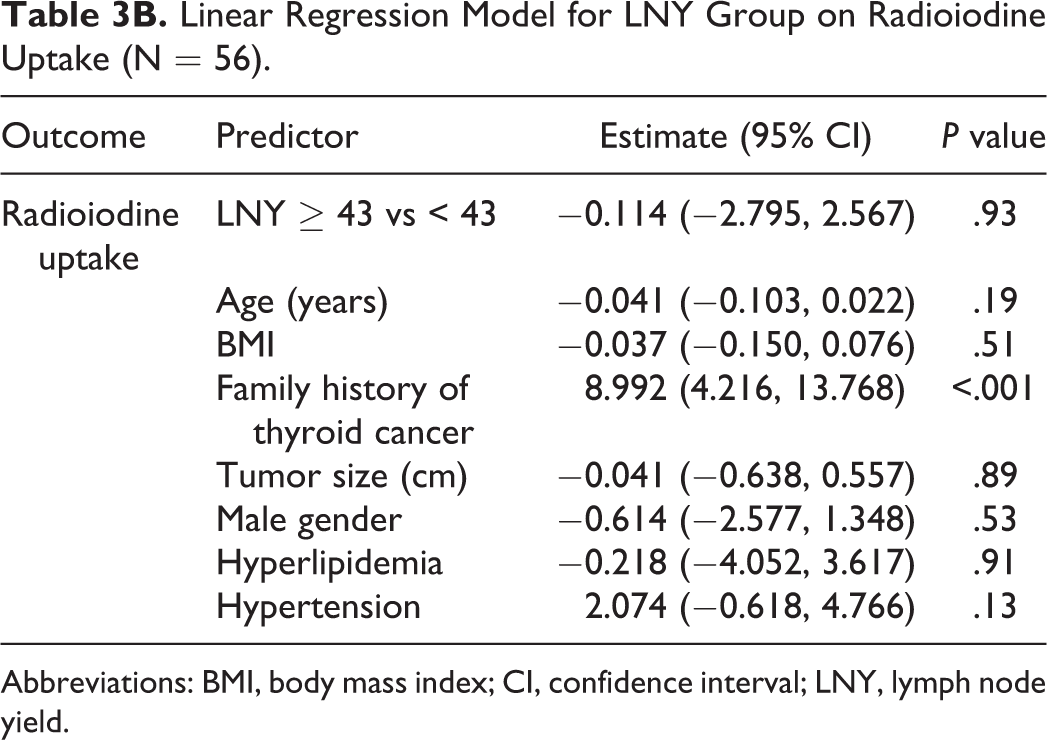
Abbreviations: BMI, body mass index; CI, confidence interval; LNY, lymph node yield.
Discussion
Over the years, treatment of the lateral neck in PTC has varied from “berry picking” lymph nodes to radical neck dissection. More recently, guidelines have strongly recommended compartment-oriented neck dissections directed at clearing the most likely sites of nodal spread, while preserving normal function postoperatively. It is unclear, however, if the completeness of the neck dissection is associated with improved patient outcomes. We find in this study that an LNY of 43 and above is found to be a threshold associated with an improved postoperative sTG. This is an important finding that suggests that a more complete lateral compartment lymphadenectomy could lead to improved outcomes.
Well-differentiated thyroid carcinomas are known to have an indolent course, and the prognostic significance of nodal metastasis is less profound than other malignancies. Studies have shown that nodal metastases larger than 3 cm and lateral neck metastases in older patients are associated with poorer outcomes. 15 The data on PTC and LNY are not as well studied, however. Heaton et al followed 71 patients for a period of 5 years and concluded that LNY from LND in PTC are significantly lower in the group with recurrence compared with the group without recurrence. 16 While their patient characteristics are similar to ours, they did not assess the impact of LNY on postoperative sTG levels. In this study, we tried to replicate their findings by estimating the association of LNY with an sTG: a surrogate marker for recurrence. Other authors dispute these findings, however. Beal et al demonstrated that an increase in LNY was associated with a decrease in survival and that nodal understaging does not have an effect on survival. 17
To adequately power a study to establish a survival or regional control improvement from LNY, large numbers of patients would be needed. Thus, we used sTG and iodine uptake as surrogate markers to assess the impact of completeness of neck dissection. Other studies are in agreement that postoperative measurement of sTG levels can be used to predict the risk of persistent or recurrent disease. A recently published study by Jayasekara et al showed that this measurement quantifies the risk of structural disease recurrence and that patients with a postoperative sTG of 2 ng/mL and lower have a lower recurrence risk. 18 Multiple studies are in agreement with postoperative sTG being a prognostic indicator19,20; Webb et al showed that a low postoperative sTG is considered as a favorable prognostic factor in PTC 19 and, therefore, can be used as a surrogate marker for patients’ outcome.
Our conclusion that a more complete LND for PTC may lead to improved patient outcomes is in line with what is known about LNY in other malignancies.9-11 Within the head and neck region, nodal yield in neck dissection for oral-cavity squamous-cell carcinoma proved to be an independent prognostic factor affecting disease-free survival, disease-specific survival, and overall survival. 21 Increased LNY in patients undergoing neck dissection for medullary thyroid cancer was also associated with improved survival. 22
Interestingly, no significant association was found between LNY and RAI uptake. One would expect that the same factors contributing to sTG elevation would also contribute to RAI uptake. It is possible that leaving functional benign thyroid tissue has more of an impact on RAI uptake than postoperative sTG and that completeness of thyroidectomy impacts RAI uptake more than postoperative sTG. The studies on RAI uptake are inconsistent. According to Bai et al, central lymph node dissection (CLND) was found to be the primary factor affecting uptake, 23 whereas another study by Yoo et al did not find any significant difference in RAI uptake in patients with or without CLND. 24 In addition, the different timing of measurement might have influenced RAI uptake more than postoperative sTG. 23
We found that a more comprehensive LND was not associated with an increased operative time nor with the odds of complications. This suggests that achieving a high LNY may not pose an additional risk to patients undergoing surgery. This finding could also be due to the experience of the surgeon, assuming that a very experienced surgeon is likely to take more nodes and also more likely to have a lower complication rate. Other studies have shown a higher complication rate when a concomitant LND is performed for thyroid cancer. 25 Our study suggests that the completeness of the neck dissection may not be the driving factor in this.
A limitation of this study was the retrospective nature and the relatively small sample size, which could result in limited power to detect true associations. Moreover, undetectable levels of thyroglobulin can be seen in patients having a PTC with cervical metastasis and in patients with high anti-TG antibody levels suggesting that recurrence monitoring should combine thyroglobulin levels and ultrasonography. In addition, the use of surrogate markers is inferior to using overall survival and recurrence rates, but in order to assess these outcomes, a larger sample size would likely require a multicenter study. Unfortunately, large databases such as the National Cancer Database do not distinguish between unilateral and bilateral neck dissection and do not give data on nodal distribution between the central and lateral compartments, thus making LNY difficult to assess.
We endeavored to propose an LNY that would improve patient’s outcome and reduce recurrence rates. Forty-three lymph nodes in a single LND specimen is a particularly high number of nodes and not often obtained, even in very comprehensive neck dissections. The inflection point that we identified may be related to our small sample size, and because of this, we do not suggest that this threshold be used as a quality metric. It does, however, offer evidence that a more complete neck dissection may be associated with improved outcomes. This study should serve as a cornerstone for future prospective projects involving a larger dataset to determine an applicable LNY that correlates with favorable postoperative outcomes.
Conclusion
This study suggests that LNY is associated with postoperative serum TG levels, and a threshold of 43 nodes is associated with a marked change in sTG levels. Lateral neck dissection is a challenging procedure that should be done by surgeons familiar with this complex anatomical compartment to decrease the risk of recurrences and revision surgeries. Additional work is needed to validate thresholds for clinical practice.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.