
Abstract
Minor salivary gland cancer is a relatively uncommon disease of head and neck, arising across the upper aerodigestive tract. This is a malignant neoplasm with diverse clinical behaviors and histological types which are prognostically significant. Although complete surgical resection, with adequate free margin, is currently the treatment of choice for locoregional diseases, the optimal treatment is still not standardized. We presented here a case of locally advanced minor salivary gland cancer that was treated by radical resection, reconstruction, and adjuvant radiation therapy at Vietnam National Cancer Hospital and had promising outcomes.
Introduction
Salivary gland carcinomas constitute an uncommon, heterogeneous group of tumors that vary in their original anatomical sites, histological, and clinical manifestations. Those malignant tumors are classified according to the 2017 World Health Organization (WHO) system. 1 Anatomically, most salivary gland tumors derive from parotid glands, accounting for 80% to 85% of cases. 2 In addition to 3 pairs of major salivary glands, there are approximately 450 to 750 minor salivary glands across the upper aerodigestive tract submucosa. 3 Tumors originating from these glands which tend to behave malignantly account for 50% to 70%. 4 Histopathologic type plays an essential role in the prediction of treatment response, survival, and time to relapse. 5
The clinical manifestation of minor salivary gland cancer depends on its original site and the extent of the tumor to adjacent structures, typically presenting with a painless mass or ulceration of aerodigestive tract mucosa and cervical lymphadenopathy. The most frequent sites of distant metastasis are the lungs, liver, and bones. 6 The staging of salivary gland cancer is similar to head and neck squamous cell carcinoma of the involved site, according to American Joint Committee on Cancer classification system version 8 (2017). 7
Radical surgical resection is the cornerstone in treatment of locoregional minor salivary gland cancer. Adjuvant radiation therapy is recommended for cases with increased risk for local and regional recurrence like bulky disease, cervical node involvement, positive resection margin, or highly aggressive subtypes. Previous data do not provide evidence for the benefit of adding chemotherapy to radiation therapy for resected patients. Definitive radiotherapy may be an alternative for medically inoperable patients or who have unresectable disease, but radical surgery with or without adjuvant radiotherapy remains the preferred treatment. 8 -10
Case Presentation
A 33-year-old female patient presented to our hospital with an increasing sore throat and painful swallowing of 3-year duration. Noticeably, 6 months earlier, she was diagnosed with right submandibular sialadenitis and underwent a complete resection of ipsilateral submandibular gland. The postoperative histological finding was chronic inflammation of salivary gland. Upon clinical examination, there was a firm, fixing mass in the right of the floor of the mouth with unclear boundaries to the right alveolar ridge and buccal mucosa; the tumor also extended to right pharyngeal wall. No suspected cervical lymph node was clinically detected.
A 55 × 65 mm solid, right deviated mass in the mouth floor was identified on magnetic resonance imaging; this mass showed contrast enhancement after intravenous gadolinium administration and extension to lateral pharyngeal muscles (Figure 1). Magnetic resonance imaging finding also revealed bilateral submandibular lymphadenopathy, and the largest node was 15 × 20 mm in size. Further diagnostic procedures including chest and abdominal computed tomography (CT) scan, bone scan, endoscopy of the upper gastrointestinal tract; and ENT demonstrated no abnormality. Opening biopsy of the mouth floor lesion revealed adenoid cystic carcinoma.
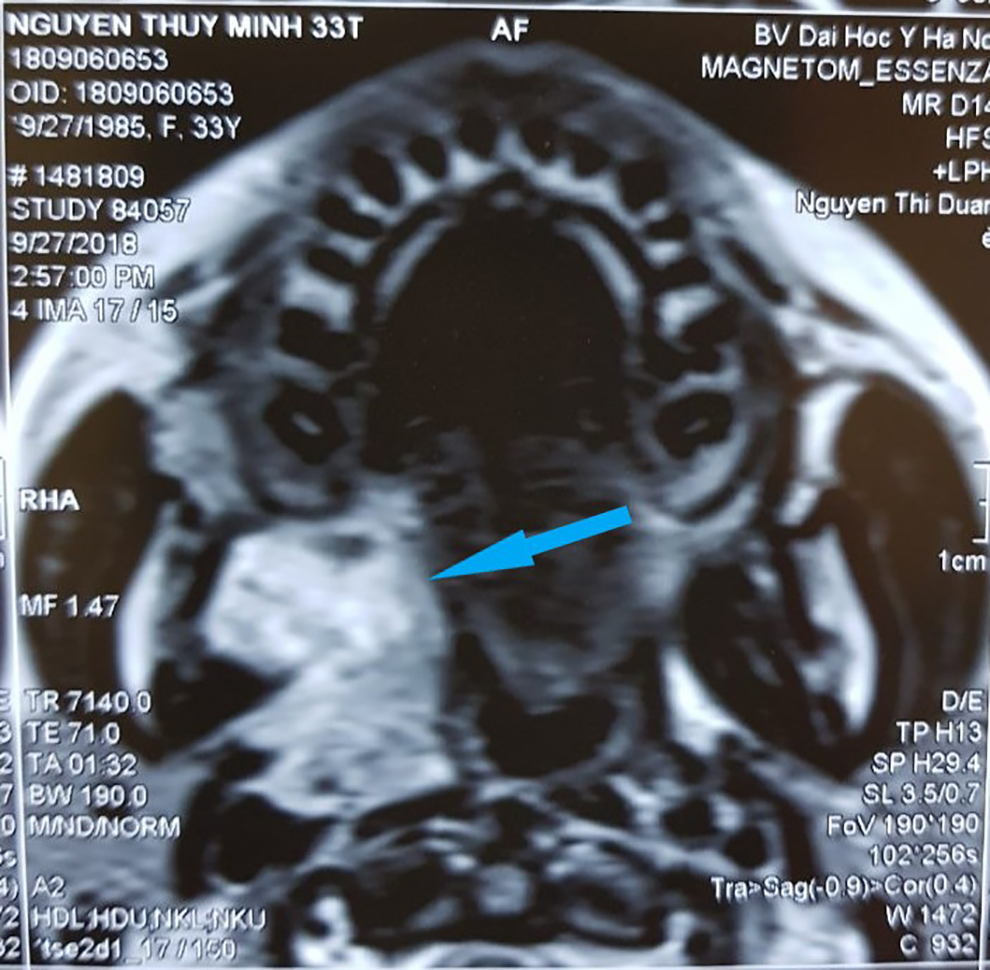
A 55 × 65 mm solid, right deviated mass in the mouth floor showed contrast enhancement after intravenous (IV) gadolinium administration and extension to lateral pharyngeal muscles (arrow).
A provisional diagnosis of a cT3N2M0 (stage IVa) oral minor salivary gland cancer was made based on the clinical and radiological appearance. Upfront tumor resection and lymphadenectomy were employed (Figure 2). The lesion was a huge mass, extended from the mouth floor to the right alveolar ridge, encompassed the mandibular body without bone invasion. The primary tumor, sublingual glands and surrounding tissue with a clear margin of 1 cm, was completely resected. In addition, a reconstruction of the floor of the mouth defects and skin covering for the mandibular were performed. Our patient also underwent neck assessment of bilateral lymph nodes from group I to V, according to Robbins classification system; these nodes were small, soft, and well defined. Cranial nerve XI and internal jugular vein were preserved. Histopathologically, the final result was adenoid cystic carcinoma, with adjunctive muscle and fat tissue involvement, and there was no metastatic node.
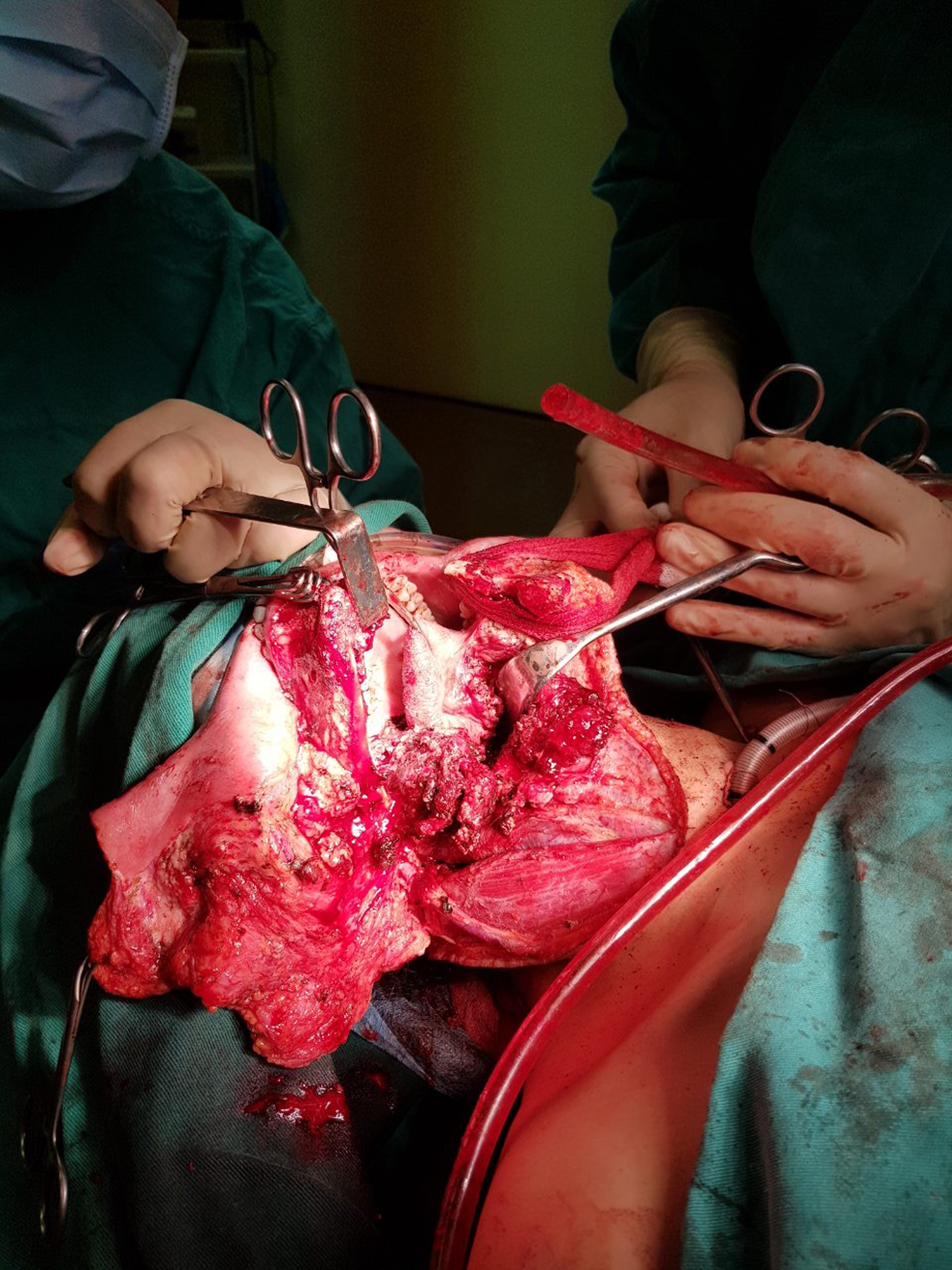
Revealing the tumor during surgery.
The postoperative assessment consisted with a diagnosis of stage pT3N0M0 minor salivary gland carcinoma. Due to the risk of local recurrence, we decided to treat with adjuvant radiation therapy by a dose of 66 Gy to the tumor bed and 60 Gy to high-risk regions. During the treatment course, she tolerated well to irradiation with no interruption, acute complications included dermatitis, pharyngitis, and dry mouth, all at grade I and completely responded to local therapy, and grade III trismus. One-month reassessment after treatment completion, cervicofacial CT scan revealed a 25-mm contrast-enhanced lesion in the base of tongue that presumed radiation-induced tissue fibrosis. Other clinical and laboratory assessments showed no abnormality. The patient was then discharged from our hospital and underwent periodic surveillance. At present, after a 3-year follow-up, she shows no signs of recurrence.
Discussion
Cancer of the salivary glands is a relatively rare disease that accounts for about 10% to 15% of all salivary gland tumors. In contrast to parotid neoplasms, of which 75% are benign, 50% to 75% of tumors originated from minor salivary glands are malignant. 2,4 There are approximately 450 to 700 minor salivary glands, occurring from the nasal cavity, sinus systems, the pharynx to the tracheal. 3 According to Hay AJ et al, the oral cavity is the most common site deriving this kind of cancer, accounting for 70% of cases; other sites are the oropharynx and nasal cavity (21% and 8%, respectively). 5 In the oral cavity, particularly, the palate is the most frequent location of malignant neoplasm. 11,12 Furthermore, 1% left of minor salivary gland carcinomas may occur in unexpected sites as lymph node, thyroid capsule, pituitary gland, and facial bone structure. 3,13 -15
Clinical manifestation of minor salivary gland neoplasms varies and reflects tumor original location and extension to adjunctive organs. Typically, patients present with a painless submucosa mass or a long-lasting ulcer of palate, lips, or buccal mucosa. Symptoms of more locally advanced disease include nasal obstruction, congestion, visual disorder, or cranial nerve dysfunction. 4,12,14,16 The lymphatic and systemic extension is rare for this disease; based on up-to-date medical literature, less than 10% of cases appear with positive node and 1% with distal metastasis. 5,12
Primary salivary gland neoplasms are histologically typed according to the 2017 WHO classification, including various types of benign and malignant tumors. By the published data, most of the minor salivary gland cancer are mucoepidermoid carcinoma (40%-54%) and adenoid cystic carcinoma (14%-31%). 5,11,17 Other types of carcinoma are less common, include low-grade pleomorphic adenocarcinoma (12%), adenocarcinoma (6%), myoepithelial carcinoma, cystadenocarcinoma, and so on. Histological typing and grading affect considerably patient survival and relapsing rate. Adverse pathologies include mucoepidermoid, adenoid cystic, small cell histological types, and undifferentiated adenocarcinoma; patients with these types are more likely to recur and have a poorer survival significantly. 4,5
Due to disease rarity and lack of prospective studies, there is no consensus guidance for standard treatment of minor salivary gland cancer. The current approach is mainly based on guidelines for major salivary gland neoplasms. For operable diseases without systemic metastasis, surgical resection is the mainstay of management. Ideally, radical surgery requires a free margin of 1 cm; immediate intraoperative biopsy is recommended if feasible. Reconstruction with local flaps or free flaps is suggested for significant skin or soft tissue defects. 14,16
Patients had clinically apparent neck node at presentation should be treated with lymph node dissection of involved area (generally, level I-III, with consideration of level II, IV removing). Cervical management of clinically negative neck node is still controversial. Some experts prefer regular elective node dissection for all patients. The others reserve this procedure for patients with suspect features for occult metastatic node: high-grade or bulky tumor (T2b tumors or larger). 5,14 According to Hay AJ et al, histologically, at least one positive node was found in 51% of cases that underwent neck dissection, of which the majority was N2 lymph node metastases. 5
Postoperative radiotherapy is suggested for patients at high risk of locoregional relapse: T3, T4 tumors, high-grade histology, peripheral nervous and vascular invasion, positive or close resection margin, or involved neck node. Definitive radiation therapy is indicated for patients with unresectable tumors or medical comorbidities that could not tolerate surgery. Unresectable disease, either by the extent of primary tumor of special location that surgical would cause considerable functional or cosmetic deficit, should be carefully evaluated by experienced surgeons. 9,18 Retrospective data have failed to prove that adjuvant chemoradiation, concurrently or subsequently, is more effective than adjuvant radiotherapy (RT) alone. An analysis of over 2000 patients from the National Cancer Database demonstrated no statistical survival benefit with the addition of chemotherapy to RT compared with RT alone. 19 The clinical benefit of this approach should be confirmed by large, well-established trials before being used routinely. An ongoing phase II/III clinical randomized trial of RTOG 1008 evaluates the benefit of adjuvant chemoradiotherapy compared to RT alone in high-risk, resected salivary gland cancer.
Patients with malignant tumors of minor salivary glands, treated by complete resection, with or without radiotherapy, present a significant survival outcome. In literature, the largest study of cancer of minor salivary gland cancer we found is a retrospective study of 450 patients from the United States. 5 All these patients were treated with surgical resection; the neck dissection and adjuvant radiation rates are 29% and 37%, respectively. The 5-year predictive overall survival rate is 86%. Estimated recurrence-free survival rates of 5-year and 10-year are 79% and 70%, respectively. On multivariate analysis, the pathological type and disease stage were significantly variable for both overall survival and recurrence-free survival. The survival and locoregional control benefit of adjuvant radiation therapy were not significant.
Conclusion
Minor salivary gland carcinoma is a rare neoplasm with variable clinical presentation and no consensus treatment guideline. Surgical resection is the choice of treatment for most cases with locoregional disease; postoperative irradiation is indicated for high-risk patients. By these approaches, the treatment outcome of minor salivary gland cancer is promising with long survival and improving quality of life. Further studies should be conducted in order to establish an optimal treatment for this malignancy.
Footnotes
Author’s Note
The study was approved by our research committee, Hanoi Medical University, Hanoi, Vietnam, and Vietnam National Cancer Hospital, Hanoi, Vietnam. The publication of this study has been consented by patient.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.