
Abstract
Objectives:
The purpose of this observational retrospective study was to evaluate, in patients with a severe acute respiratory syndrome coronavirus 2 infection, the association between the severity of coronavirus disease 2019 (COVID-19) respiratory illness and the risk of infected patients to develop obstructive sleep apnea (OSA).
Methods:
Ninety-six patients with confirmed COVID-19 infection were enrolled in the study. The STOP-BANG questionnaire to investigate the risk of the OSA syndrome was filled in by the patients at admission. The enrolled patients were divided into 2 groups according to the respiratory disease: group 1 (72 patients), hospitalized patients undergoing conventional oxygen therapy; group 2 (24 patients), patients requiring enhanced respiratory support. STOP-BANG results of these 2 groups were compared to observe whether patients with high OSA risk more frequently presented a severe form of COVID-19.
Results:
41.6% of the patients in group 2 had a STOP-BANG score between 5 and 8 (high risk of having apnea); in contrast, 20.8% of the patients in group 1 had a STOP-BANG score between 5 and 8, with a statistically significant difference between the 2 groups (P = .05). A complementary trend was observed regarding the proportion of patients in the range 0 to 2, which classifies patients at a low risk of OSA (48.6% vs 20.8% for groups 1 and 2, P = .01).
Conclusions:
According to our data, the chances of having a severe case of COVID-19 should be considered in patients at high risk of OSA.
Current Knowledge/Study Rationale:
Emerging research suggests that OSA could represent a potentially important risk factor for the severe forms of COVID-19. The purpose of this observational retrospective study was to evaluate the potential association between OSA and the severity of COVID-19 disease.
Study Impact:
According to our data, the likelihood of contracting a severe form of COVID-19 disease should be considered in patients at high risk of OSA.
Introduction
More than 120 million people have been infected with the novel severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) virus worldwide and over 2 million and 666.649 died as a result of coronavirus disease 2019 (COVID-19), with the death toll still rising. Mortality in patients is mostly determined by acute hypoxemic respiratory failure meeting the criteria for acute respiratory distress syndrome (ARDS). However, cardiovascular complications may also contribute. 1,2 Age and comorbidities play an important role in the prognosis, proven by several studies published over the past months. 3 -18
Obstructive sleep apnea (OSA) syndrome is a respiratory sleep disorder characterized by reduction (hypopnea) or complete cessation (apnea) of the airflow through the upper airways, in the presence of breathing effort, that occurs during the night. It is a common and undiagnosed disease, with an incidence rate between 5% and 17% among the middle-aged population and 20% to 60% in people older than 65 years. 19 -24
Emerging research suggests that OSA could represent a risk factor for the severe forms of COVID-19. More than the classic daytime sleepiness, this illness is characterized by a high incidence of systemic comorbidities such as cardiovascular problems, diabetes and metabolic disorders, neurocognitive dysfunction, overlap syndrome, systemic inflammation and altered immune response to infection, as well as an elevated risk of hospitalization. Therefore, severe COVID-19 infection and OSA patients share risk factors such as obesity, cardiovascular disease, hypertension, diabetes, age, and male sex. Studies investigating this presumed association have recently begun to appear in the literature. 7,8,19 -21
The purpose of this retrospective observational study has been to evaluate, in patients with a SARS-CoV-2 infection, the association between the severity of COVID-19 respiratory illness and the risk of infected patients of developing OSA.
Patients and Methods
We conducted this retrospective study in 2 tertiary health care referral centers: “G.B. Morgagni-L. Pierantoni” Hospital, Forlì, Italy, and “Vito Fazzi” Hospital of Lecce, Italy. Ninety-six patients consecutively admitted to the Hospitals from April 1 to May 30, 2020, were retrospectively included in the study if they met the following inclusion criteria: (1) confirmed COVID-19 infection, as determined by a positive reverse transcriptase polymerase chain reaction assay of a specimen collected on a nasopharyngeal swab, and (2) diagnosis of COVID-19 pneumonia. The medical records of each patient were retrospectively analyzed and, for each patient, the following information was extracted and recorded in a dedicated database: age, sex, body mass index, comorbidities (hypertension, diabetes, cardiovascular diseases, bronchial asthma, allergic rhinitis), known OSA diagnosis, PaO2/FiO2 ratio (P/F ratio) at admission.
In patients with a previous diagnosis of OSA, the last polysomnography (PSG) test performed by the patient was evaluated and the apnea/hypopnea index (AHI), which classifies the severity of OSA, was extrapolated.
The STOP-BANG questionnaire developed to investigate the risk of OSA syndrome was submitted to each of these patients on hospitalization. 25 -28 The STOP-BANG questionnaire issued to the patients referred to the period of time prior to the COVID-19 infection and hospitalization. The STOP-BANG is a validate questionnaire, 26,27 which produces a score that directly correlates with the risks of having an OSA diagnosis at PSG examination. Table 1 summarizes the STOP-BANG questionnaire as reported by Chung et al. 25 Based on the STOP-BANG results, patients were subdivided into high risk of OSA (values 5-8), intermediate risk of OSA (values 3-4), and low risk of OSA (values 0-2). 25 -28
STOP-BANG Sleep Apnea Questionnaire Chung et al. 21, a
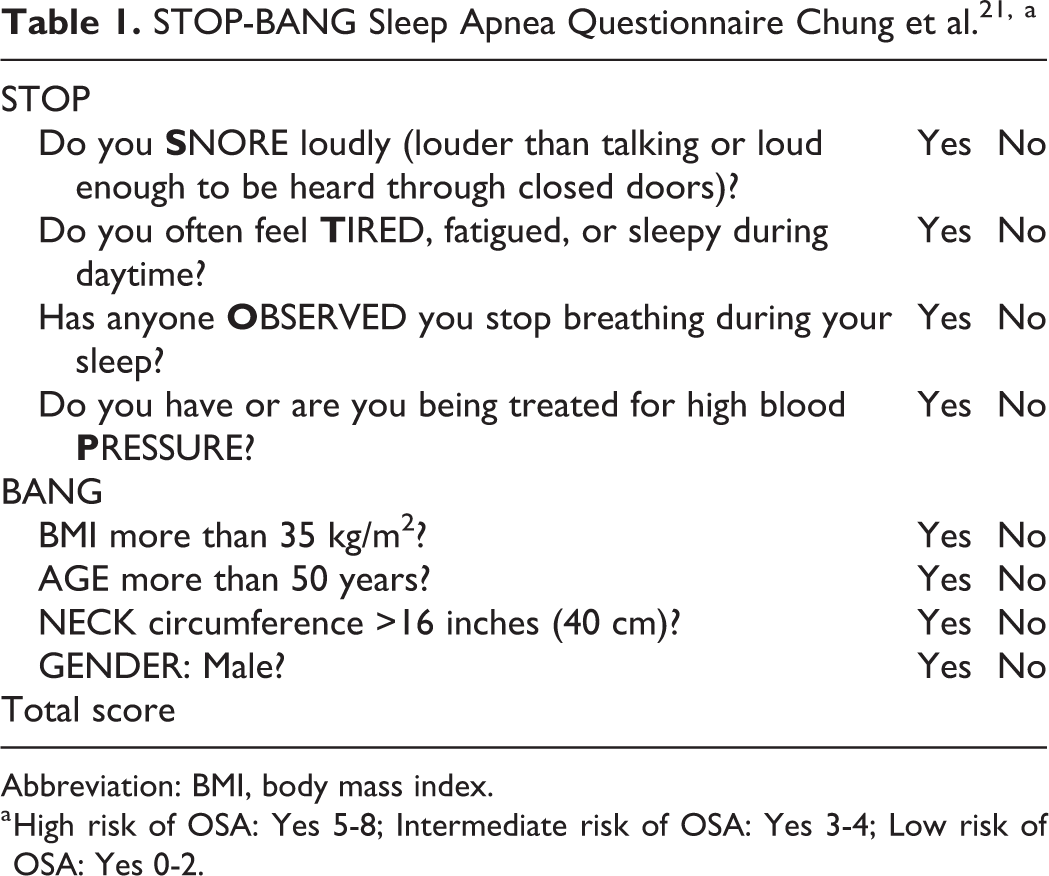
Abbreviation: BMI, body mass index.
a High risk of OSA: Yes 5-8; Intermediate risk of OSA: Yes 3-4; Low risk of OSA: Yes 0-2.
The enrolled patients were divided into 2 groups based on their COVID-19–related respiratory disease. Group 1 (72 patients), hospitalized patients undergoing conventional oxygen therapy Group 2 (24 patients), patients requiring enhanced respiratory support including high flow nasal cannula, noninvasive ventilation, tracheal intubation, or invasive mechanical ventilation
STOP-BANG results of these 2 groups were compared to observe whether patients with high risk of having OSA most frequently showed a severe respiratory disease related to the COVID-19 infection.
Finally, the P/F ratios measured on hospitalization were collected and compared with the results of the STOP-BANG questionnaire in order to compare the respiratory disease and the risk of developing OSA. The P/F ratio is the ratio of arterial oxygen partial pressure (PaO2 in mm Hg) to fractional inspired oxygen (FiO2 expressed as a fraction). 1 -5 Normal P/F ratio is ∼400 to 500 mm Hg, whereas an ARDS could be defined in the event of a P/F ratio <300 mm Hg. 1 -5 Therefore, in this study, a cutoff of <300 mm Hg was used to define patients with respiratory disease. In this correlation analysis, a cutoff >3 in the SOP-BANG results was adopted to define patients with high probability of having OSA. This cutoff demonstrated a high diagnostic accuracy, as well as ease of use, and clear thresholds for risk stratification, in different anesthesia studies and preliminary reports by Chung et al. 15,16,25
Given the retrospective nature of the study and anonymity, ethic committee approval was not required. 2
Statistical Analysis
To test the differences among groups, a χ2 test was used for analyzing categorical data differences. Linear regression analysis was used to evaluate a linear correlation between STOP-BANG results and P/F ratio. A P value <.05 was considered statistically significant. All analyses were performed using STATA version 12.1 software.
Results
The clinical characteristics and comorbidities of the 2 groups of patients evaluated are provided in Table 2.
Clinical Characteristics (Age, Sex, BMI), Comorbidities.
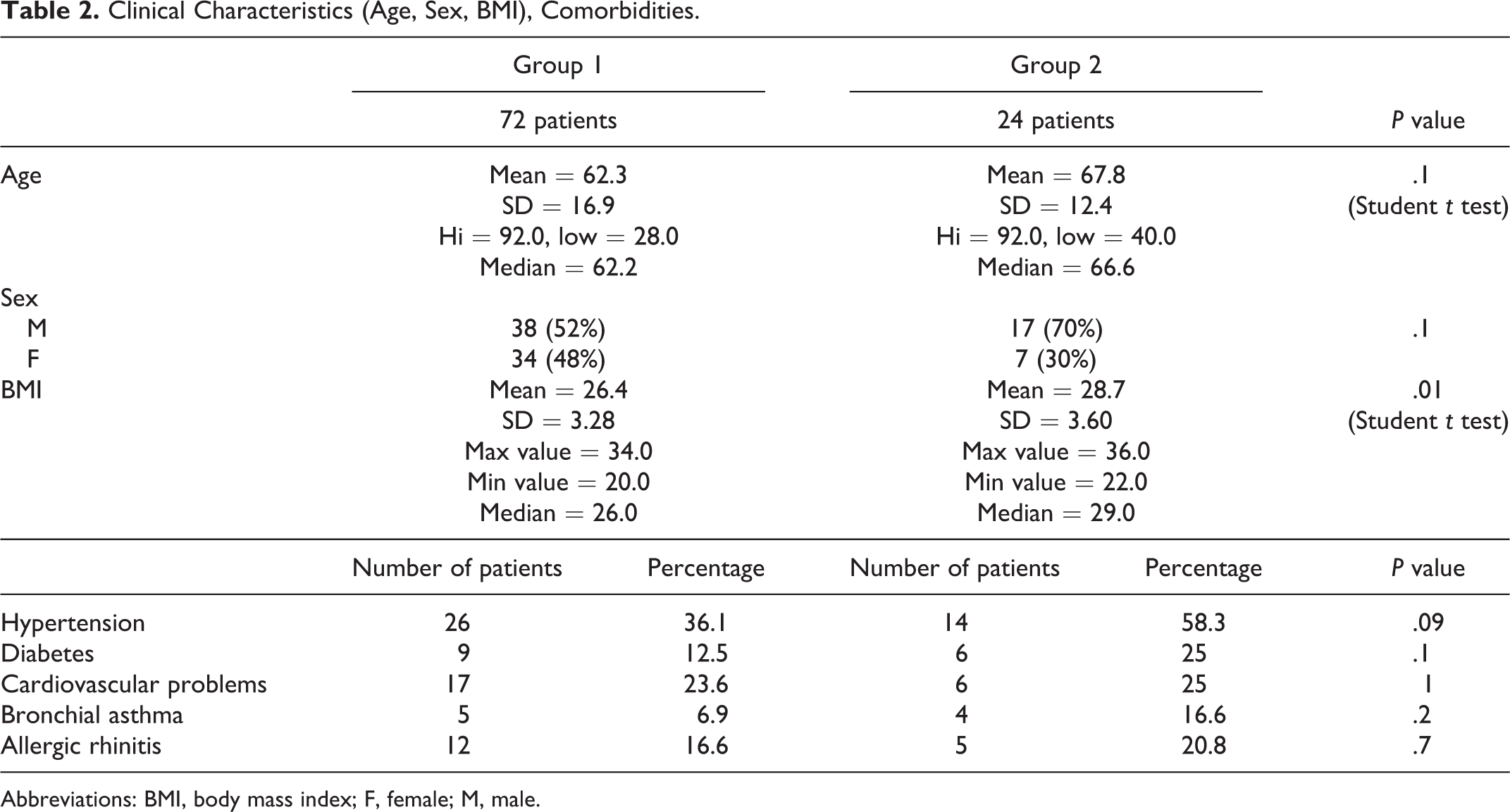
Abbreviations: BMI, body mass index; F, female; M, male.
A medical history of OSA was reported by 20.8% of group 1 patients and 29.1% of group 2 patients. All these patients had a score >3 at the STOP-BANG questionnaire. Despite a higher incidence of sleep apnea in patients who required ventilatory therapy, no statistical difference emerged between these 2 groups of patients (P= .4).
In Table 3, the distribution of patients with a previous anamnesis of OSA in according to the subclasses severity is reported. A statistical difference was emerged among patients diagnosed with severe OSA (AHI > 30) between the 2 groups of patients enrolled in the study (P = .05).
Differences Between Severity of COVID19 Disease and Risk of Having OSA.
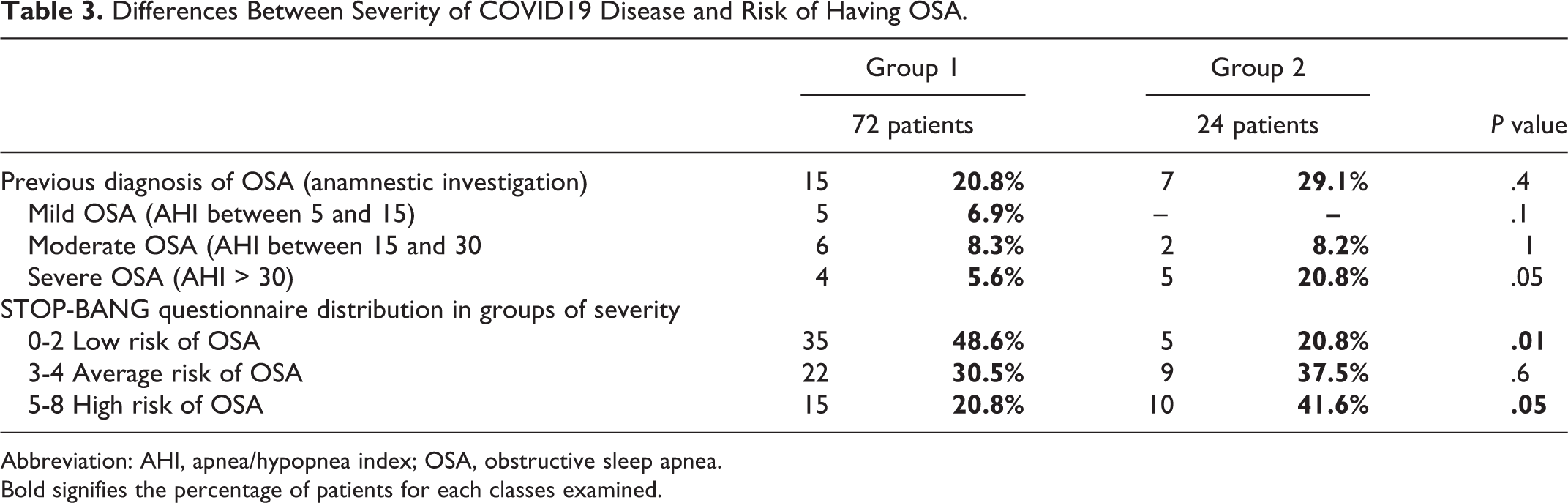
Abbreviation: AHI, apnea/hypopnea index; OSA, obstructive sleep apnea.
Bold signifies the percentage of patients for each classes examined.
By means of the STOP-BANG questionnaire, it emerged that 41.6% of patients in group 2 had a score between 5 and 8 (high risk of having apnea), while 20.8% of the patients in group 1 had a STOP-BANG score between 5 and 8, with a statistically significant difference between the 2 groups (P = .05).
A complementary trend was observed regarding the proportion of patients in the range 0 to 2, which classifies patients at a low risk of OSA (48.6% vs 20.8% for groups 1 and 2; P = .01).
No statistical difference emerged in the distribution between groups regarding the average risk of OSA (P = .6).
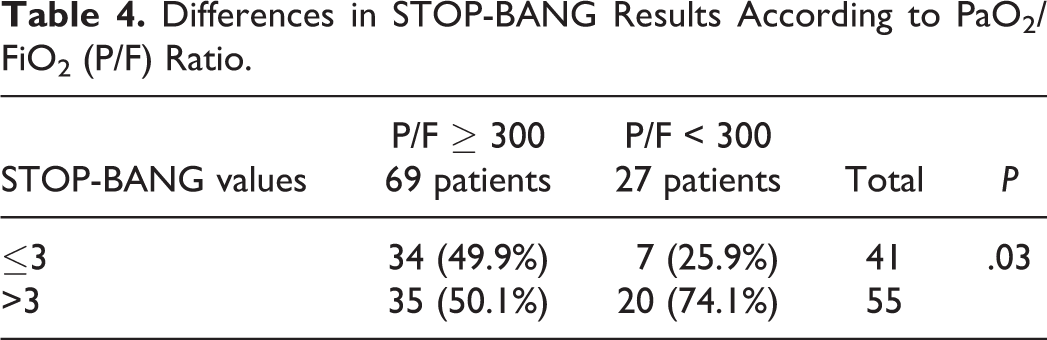
A linear correlation between lower values of P/F ratio and the severity of STOP-BANG questionnaire results emerged using a linear regression (P = .0001), as per Figure 1. In addition, considering patients with a P/F ratio <300 (27 patients), 74.1% showed a STOP-BANG value >3 and 24.9% a value <3 (Table 4). On the other hand, in patients with a P/F ratio >300 (69 patients), the STOP-BANG value was >3 in 49.9% of patients and <3 in 50.1% of cases. A statistical difference between classes of P/F ratio emerged regarding incidence in patients with a STOP-BANG value >3 (test χ2 = 4.3240, P value = .03).
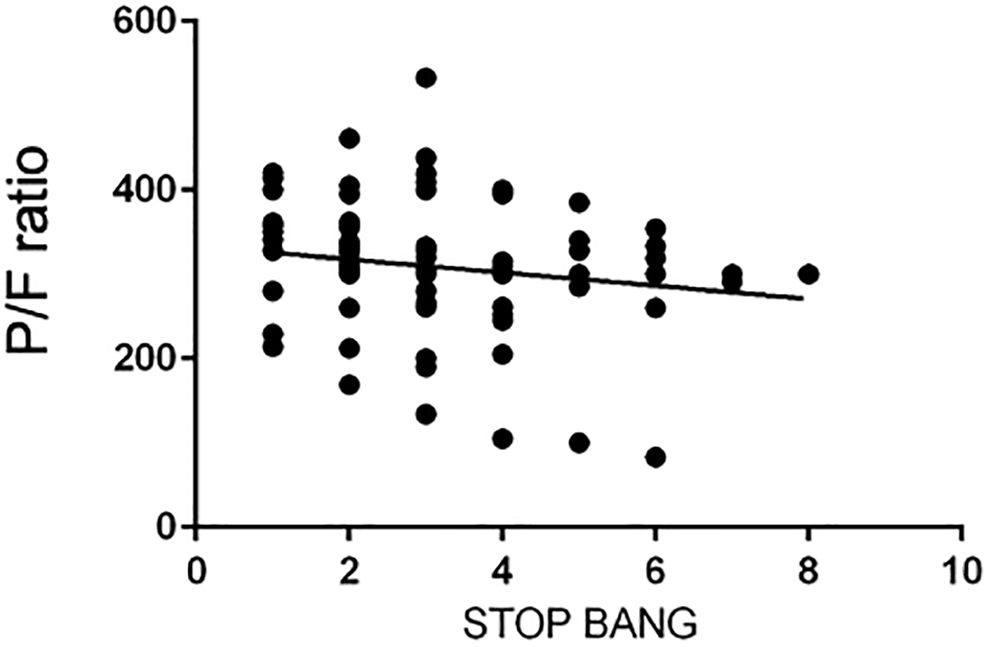
Linear correlation between STOP-BANG results and PaO2/FiO2 ratio (P value = .0001).
Differences in STOP-BANG Results According to PaO2/FiO2 (P/F) Ratio.
Discussion
Emerging research suggests that OSA could represent a risk factor for the severe forms of COVID-19. 7 -9 McSharry and Malhotra 8 have hypothesized the potential influence of OSA on COVID-19 infection severity, due to the known comorbidities that characterize this syndrome. In addition, the authors claimed that OSA (particularly with concurrent obesity) could potentially contribute to worsening hypoxemia and the cytokine storm that occurs in COVID patients. Subsequently, Memtsoudis et al 9 showed how an OSA diagnosis was present in 11.4% of critical COVID-19 patients with respiratory failure, receiving mechanical ventilation. They also stated that the high prevalence of undiagnosed OSA could potentially contribute to the high morbidity among obese patients with COVID-19 infection.
In a nationwide multicentric observational study comprising diabetic patients hospitalized for COVID-19, the treatment for OSA involved a risk of tracheal intubation for mechanical ventilation and death in 1.44% and 1.81% of patients, respectively. 10 At the same time, Maas et al 7 evaluating ICD-10-CM coding of OSA identified a higher prevalence of OSA diagnosis among patients requiring hospitalization for COVID-19 infection (15.3% vs 3.4%, P < .0001; OR 5.20, 95% CI, 4.43-6.12) and among those who progressed to respiratory failure (19.4% vs 4.5%, P < .0001; OR 5.16, 95% CI, 4.41-6.03). However, these preliminary observational studies used health administrative databases to identify patients with OSA. 11
Undiagnosed OSA is a well-known public health problem and an important contributor to negative postoperative outcomes in surgical patients. 15 Therefore, the number of patients with severe COVID-19 and OSA could be higher than reported in the literature until now. The STOP-BANG questionnaire was developed as a screening tool that correlates with the risk of having OSA. It consists of 4 self-reportable (STOP: snoring, tiredness, observed apnea, and high blood pressure) and 4 demographic (BANG: body mass index, age, neck circumference, and gender) items. In the initial validation study, at a score of at least 3, the STOP-BANG questionnaire demonstrated a high diagnostic accuracy, as well as being easy to use, and clear thresholds for risk stratification, justifying its adoption in preoperative screening. 16,25,27 -30 Further, we used the STOP-BANG as a triage tool in our hospital on a regular basis to identify a major number of patients with OSA. 25 -27
We have divided the enrolled patents into 2 groups (1 and 2) according to the disease severity. Previous personal history of OSA was reported by 20.8% and 29.1% of group 1 and group 2 patients, respectively. These data are very similar to those reported by Bhatraju et al 17 (21% of patients hospitalized for a severe COVID pneumonia showed a personal medical history of OSA) and data of Arentz et al, 18 which by evaluating clinical characteristics and outcomes of 21 critically/severe patients with COVID19 infection, showed as 28.6% of these patients had a personal history of snoring and sleep apnea. Besides, in our study, a greater prevalence of patients with an anamnesis of severe OSA (AHI > 30) was observed in the group 2 patients (severe respiratory disease) with a statistical difference (Table 3, P = .05).
Using the STOP-BANG questionnaire, it emerged that 41.6% of patients with severe COVID-19 infection presented a score between 5 and 8 (high risk of having apnea); in contrast, 20.8% of the patients in group 1 (mild COVID19 infection) had a STOP-BANG score between 5 and 8, with a statistically significant difference between the 2 groups (P = .05). A similar statistical difference emerged in the distribution of patients in the range 0 to 2 (48.6% vs 20.8%; P = .01). Furthermore, linear regression correlated a high value of STOP-BANG with lower values of P/F ratio. Finally, patients with a P/F ratio <300 more frequently showed a STOP-BANG value >3 (P = .03).
These findings suggest that patients at risk of OSA could develop a more severe respiratory COVID-19–related disease. Besides, this study confirms, as previously suggested by Maas et al, 7 that OSA screening may be helpful in guiding management decisions in COVID-19 patients.
This study, whose aim was to evaluate the risk of patients to develop OSA, does present some limitations. The PSG examination of sleep, the gold standard for performing an OSA diagnosis, was not performed. Unfortunately, it was not possible to perform PSG testing to obtain an OSA diagnosis, because it would have implied a higher risk of spreading COVID-19 virus among health care personnel and in the hospital.
We measured the risk of OSA in each patient affected by COVID-19 infection, employing the validated STOP-BANG questionnaire. Its score directly correlates with the likelihood of obtaining an OSA diagnosis at PSG examination. 25-26 Moreover, the questionnaire has demonstrated a high sensitivity using a cutoff score of ≥3 with 84% sensitivity in detecting any sleep apnea (AHI > 5 events per hour), 93% sensitivity in detecting moderate-to-severe sleep apnea (AHI > 15 events per hour), and 100% sensitivity in detecting severe sleep apnea (AHI > 30 events per hour). 25 -27 However, the possibility of false-positive results, due to the presence of a respiratory disease, should be considered.
In addition, dead and asymptomatic COVID-19 patients have not been included in this study. Probably, further differences between the 2 groups of patients would have emerged. A further study is under way to compare the risk of OSA between asymptomatic and hospitalized patients. The small sample used in the study and the retrospective analysis are limitations related to the evaluation of patients with an infectious disease and common to many of the studies published so far on COVID-19. 27,31
Conclusions
Our data suggest that the likelihood of a severe case of COVID-19 increases in patients at high risk of OSA. Multicenter studies on a larger population of patients will be necessary to confirm these preliminary findings.
Footnotes
Authors’ Note
All procedures performed in this study involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.