
Abstract
Extraganglionic Burkitt’s lymphoma is rare. Primary thyroid localization accounts for 1% to 5% of malignant tumors of the thyroid gland. The association of Burkitt’s lymphoma and pregnancy is even rarer. Our patient was pregnant at 36 weeks. She was brought to the emergency department with anterior cervical swelling, rapidly increasing in volume and becoming compressive for 15 days, in addition to dysphonia and inspiratory dyspnea. Cervical ultrasound and computed tomography scan revealed a compressive and plunging goiter. Surgery attempted after fetal extraction proved impossible due to massive tumor infiltration into adjacent structures shielding the cervical region. Accordingly, the act was limited to a glandular biopsy. The newborn was healthy. Histological examination confirmed the diagnosis of Burkitt’s lymphoma. Given the poor general condition of the patient, chemotherapy was not administered and the patient died after 15 days of stay in intensive care unit.
Introduction
Burkitt’s lymphoma of the thyroid gland is an extremely rare entity. It constitutes 1% to 5% of thyroid cancers. This pathology affects mainly the elderly patients with a striking female predominance (sex ratio = 0.33). 1
Burkitt’s lymphoma is endemic in Africa while it is sporadic elsewhere. This is due to the strong association with infections by Epstein-Barr virus (EBV). It is more common in immunocompromised patients and those with Hashimoto lymphocyte thyroiditis. 2
The incidence of thyroid lymphoma in a pregnant woman is estimated at 1/6000 women per year. 3 The association of Burkitt’s lymphoma with pregnancy is even rarer. This leads us to discuss, based on our observation and the related literature, the different diagnostic and therapeutic difficulties with respect to this case.
Case Report
It was a 31-year-old patient with no history of illness and pregnant at 36 weeks. She was brought to the emergency department with anterior cervical swelling, which had increased quickly in volume for 2 months and had become compressive for 15 days, as well with worsening dysphonia and inspiratory dyspnea. The patient’s condition became steadily worse. This mass was not associated with dysphagia or signs of dysthyroidism or any infectious syndrome.
The physical examination revealed an indurated voluminous basicervical swelling of 12 cm size, whose lower limit was not palpable. There was no cervical lymphadenopathy. The patient was polypneustic. Oxygen saturation ranged from 85% to 92%. Indirect laryngoscopy was not performed for fear of increasing respiratory distress (Figure 1).

Picture of the patient showing a large cervical swelling in a pregnant woman.
Cervical ultrasound showed a large compressive pseudonodular thyroid goiter invading the right isthmolobar and whose lower edges are ill defined. Since the patient was at 36 weeks and in emergency situation, additional exploration by cervico-mediastinal computed tomography (CT) was performed, which revealed the presence of a large mass of the thyroid compartment of 13 × 8 cm, more marked development of right side, lobulated contours, and extention to the retrosternal space and pre-aortico-cave. It exerted a mass effect on the aerodigestive axis, pushing the latter toward the left side. Tracheal light was reduced by 70%, from C7 to D3 (Figure 2). The hormonal assessment was correct. Antithyroid antibodies and EBV serologies were negative.
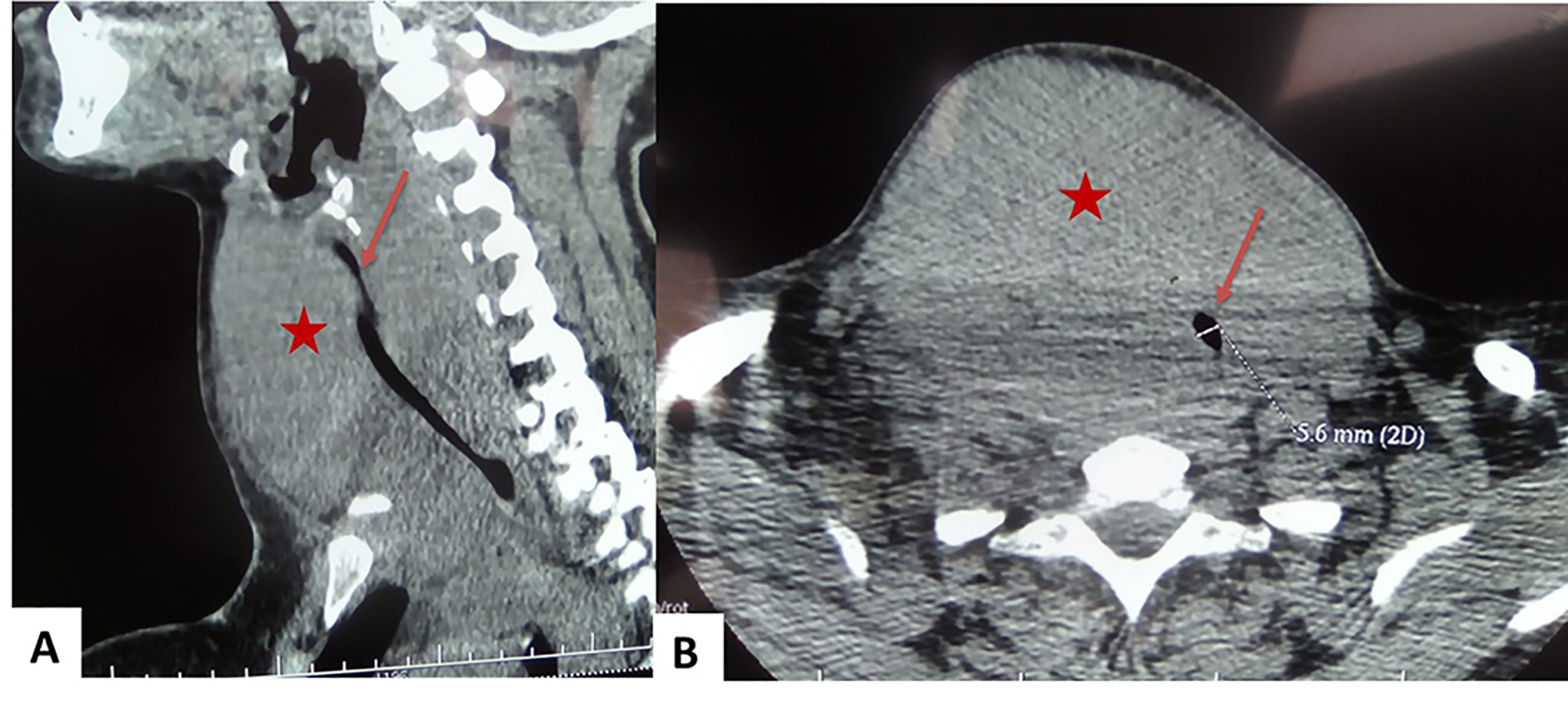
(A) Sagittal view of cervical computed tomography (CT) scan: large thyroid mass (star)reducing tracheal light(arrow) by 70% from C7 to D3. (B) Coronal view of cervical CT scan: large homogeneous thyroid mass (star)reducing tracheal light (arrow), plunging into the mediastinum.
The patient was operated in collaboration with the Gynecology-Obstetrics team. Fetal extraction was performed in parallel with thyroid gland exploration. As soon as incision was made, induration of the entire thyroid gland and surrounding muscles were observed. The dissection was very difficult or even impossible. The patient was kept intubated and then transferred to the intensive care unit. The newborn was healthy.
Histological examination showed diffuse lymphomatous proliferation of medium-sized cells and countless macrophages with tangible bodies giving the appearance of the starry sky. The cells had reduced cytoplasm and granular chromatin nuclei. Mitoses and apoptotic bodies were numerous. The immunohistochemical study have shown the positivity of the markers CD20, CD10, and C-Myc. The CD3 marker was negative. The K67 factor was positive with a 95% proliferation index (Figure 3). The diagnosis of Burkitt’s lymphoma was retained. Abdominal CT was normal.
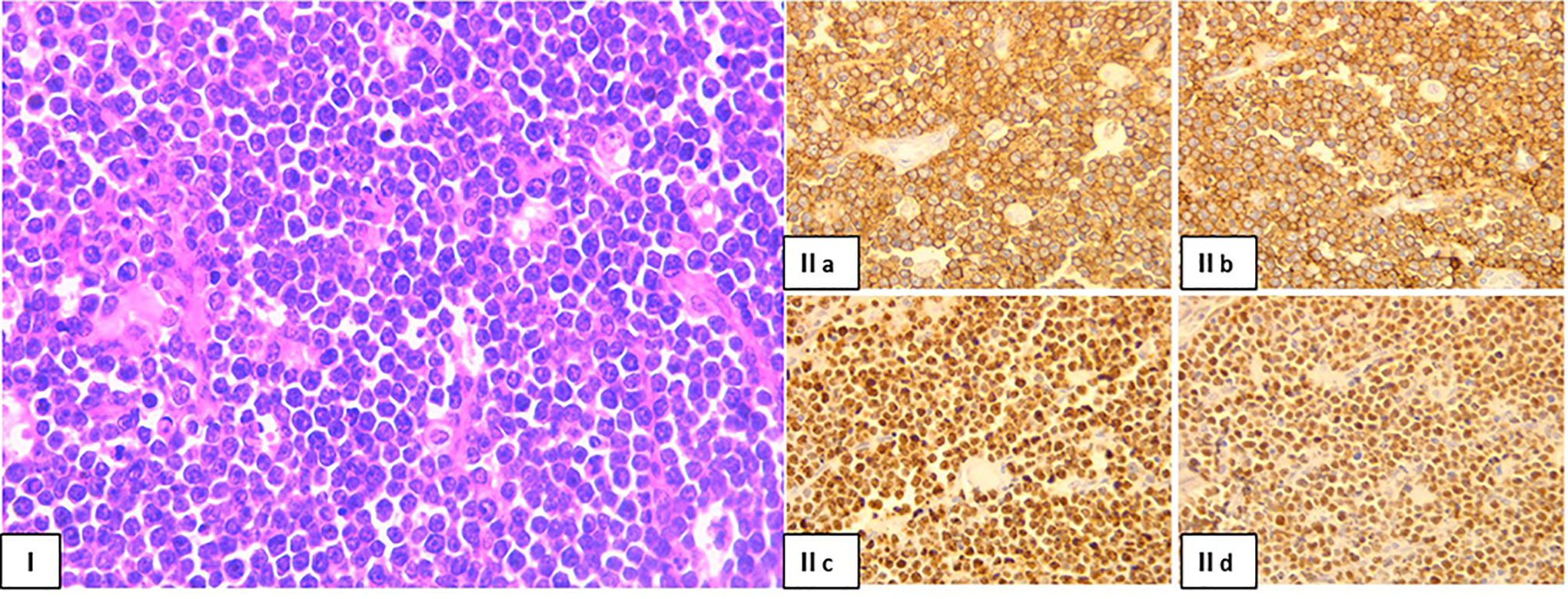
I, Sheets of monotonous intermediate size cells with starry sky appearance (hematoxylin and eosin staining) ×400. II, Immunohistochemistry (II a) CD20 is strongly and diffusely positive; (II b) CD10 is strongly positive; (II c): Ki67 positivity is approaching 100%; (II d) BCL6 stain is strongly and diffusely positive (×400).
In view of the deterioration of the patient’s general condition, chemotherapy was not done. Tracheotomy was performed in transtumoral to extubate the patient. It was made easy by introducing a fiberoptic through an intubation tube, which helped us locate the trachea by transillumination. The patient then developed a cesarean delivery skin infection followed by sepsis and multiple organ failure. She died after 9 days of stay in intensive care unit.
Discussion
Burkitt’s lymphoma of the thyroid gland is exceptional. There are only 23 cases reported in the literature. 4 It predominantly affects elderly female patients (3 women for a man). 5,6 Our case is peculiar in that it concerns a young and pregnant woman. In fact, the incidence of lymphoma during pregnancy is estimated at 1 in 6000 women per year. 3 This tumor develops from B lymphocytes and is endowed with a highly locally aggressive power reminiscent of anaplastic thyroid carcinoma.
The clinical presentation of thyroid Burkitt’s lymphomas is nonspecific. They manifest as enlarged anterior cervical swelling associated with a compressive syndrome and occasionally with a tumor lysis syndrome. Most often patients are in clinical and biological euthyroidism.
The first radiological examination recommended is cervical ultrasound. Thyroid lymphoma was suspected on the basis of the highly hypoechoic nature, posterior reinforcement, hypervascular character, and absence of calcifications. All these criteria are nonspecific. 7 The use of CT may be necessary to better assess locoregional extent. Given that irradiation is teratogenic in the first and second trimester of pregnancy, investigations in pregnant woman should be limited to cervical ultrasound and fine needle aspiration. 3,8
Although fine needle aspiration is the first examination to be requested after ultrasound, its diagnostic contribution to thyroid lymphoma is very limited. Most often, it can demonstrate the presence of an intermediate-sized B lymphocyte, basophilic cytoplasm, and cytoplasmic vacuoles. The nuclei are rounded with a dense chromatin, site of several nucleoli. The cytoplasm is rich in macrophages, which is indicative of cell proliferation and significant apoptosis. However, this is rarely seen owing to the paucicellular nature of the sample. Therefore, the test has low sensitivity. In addition, it is a little specific examination in cases of thyroid lymphomas since it can be found in lymphocytic thyroiditis especially Hashimoto’s thyroiditis. The sample size is usually insufficient to perform immunohistochemistry study, hence the need for an open glandular biopsy supplement. 4,8 -10
Recently, several studies have demonstrated the superiority of glandular needle biopsy, allowing sufficient sampling to achieve accurate diagnosis and avoid unnecessary and not risk-free surgery. 11,12 Our patient immediately underwent an open biopsy as she had respiratory distress and the maternal–fetal prognosis was at stake.
The treatment of thyroid lymphoma is based on the combination of chemotherapy and radiotherapy according to the histological subtype. The contribution of surgery is limited because they are radio-tumors and chemosensitive and whose surgery is very difficult and not without risk.
In case of Burkitt’s lymphoma, given its significantly locally aggressive potential, chemotherapy must be intensive, close and started as soon as possible. The prescribed protocol is CHOP (cyclophosphamide, doxorubicin, vincristine, and prednisone) or R-CHOP (rituximab, cyclophosphamide, doxorubicin, vincristine, and prednisone) associated with methotrexate. 1,8
In pregnant women, the prescription of chemotherapy for the other histological types of lymphoma is possible, irrespective of the duration of pregnancy, with the adaptation of molecules and their doses while preserving the fetal and maternal prognosis. It was proved that the benefit of adequate cancer treatment outweigh its teratogenic risk. As for highly aggressive Burkitt-type lymphomas, their behavior requires prompt initiation of treatment with a chemotherapeutic regimen that is similar to the treatment of leukemias. These are contraindicated because of the high methotrexate dose they contain (risk of malformation and deep myelosuppression). Therapeutic abortion should be recommended, especially in early pregnancy. 3 The advantage our patient had is that she was full-term pregnant, thereby enabling to save the fetus before starting the therapeutic protocol.
The prognosis for Burkitt’s lymphoma depends on the stage and speed treatment initiation. Other prognostic factors described are large tumor size, mediastinal extension, rapid increase in tumor size, the presence of tumor lysis syndrome, and extension to the aerodigestive axis. 7 Our patient had died before she started chemotherapy because of sepsis and multi-organ failure.
Conclusion
The clinical presentation of thyroid Burkitt’s lymphomas is nonspecific. They manifest as an enlarged anterior cervical swelling associated with a compressive syndrome.
In pregnant women, investigations should be limited to ultrasound and fine needle aspiration. Several studies have demonstrated the superiority of glandular needle biopsy which provides sufficient sample to confirm diagnosis. Their behavior requires prompt initiation of treatment with a chemotherapeutic regimen. Therapeutic abortion should be recommended, especially in early pregnancy.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.