
Abstract
Malignancy of hematopoietic origin comprises a large portion of all pediatric malignancies; however, it is uncommon for patients with this condition to present only with symptoms related to temporal bone involvement. Here, we report a case of Burkitt Lymphoma of the temporal bone in an 8-year-old patient who initially presented with symptoms of acute otitis media. Additionally, we review the current literature on pediatric hematopoietic malignancy with primary temporal bone involvement and discuss the clinical presentation, management, and outcomes of these rare cases.
Introduction
Hematopoietic malignancies are the most common subtype of pediatric malignancy, accounting for 41.3% of all new cancer diagnoses in pediatric patients between 2003 and 2014. 1 Involvement of the temporal bone in hematopoietic malignancies has been well documented2,3 though disease found in the head and neck is most commonly a metastasis from a distant primary.4,5 Normally, temporal bone involvement is asymptomatic at presentation or becomes symptomatic after the initial diagnosis has been made. 4 As a result, physicians rarely encounter pediatric patients with this condition who are experiencing symptoms solely related to temporal bone involvement at initial presentation. Given the lack of familiarity with this condition, it is easy to attribute signs and symptoms of hematopoietic malignancies of the temporal bone to more common benign conditions, such as acute otitis media (AOM) and mastoiditis.
In this article, we report a rare case of pediatric stage IV sporadic Burkitt Lymphoma (BL) with primary mastoid infiltration and central nervous system (CNS) involvement initially presenting as a benign ear infection. Due to the rarity of reports on this subject, we also performed a review of the literature on hematopoietic malignancy presenting primarily in the temporal bone of pediatric patients.
Case Report
A previously healthy 8-year-old male presented to an urgent care facility with left-sided otalgia and postauricular pain. He received a 10-day course of oral amoxicillin and topical ciprofloxacin/dexamethasone drops for presumed AOM and otitis externa with no improvement.
He was admitted for inpatient management 3 weeks after his initial presentation for new-onset ipsilateral facial weakness. He was started on broad-spectrum intravenous antibiotics and topical ciprofloxacin/dexamethasone drops were continued. Otolaryngology consultation was obtained. Physical examination at this time was notable for mastoid tenderness without edema or erythema. The external auditory canal (EAC) was markedly edematous with granulation tissue medially obscuring the tympanic membrane (TM). Ipsilateral facial nerve function was House-Brackmann (H-B) grade V.
Laboratory values upon admission included a white blood cell count of 8100 per microliter with neutrophils elevated at 70% and lymphocytes low at 20%. Hemoglobin/hematocrit was low at 8.8/28. Erythrocyte sedimentation rate and C-reactive protein were elevated at 38 and 1.8, respectively. Computed tomography (CT) of the temporal bones demonstrated left EAC, mastoid and middle ear opacification with possible dehiscence of the sigmoid plate but no clear evidence of other bony erosion or coalescence, and no identifiable abnormality or dehiscence of the facial nerve (Figures 1 and 2). Ear examination under anesthesia revealed granulation tissue in the EAC with possible extrusion through the TM. The granulation tissue was debrided, and myringotomy was deferred due to lack of landmarks. Prednisone 30 mg orally twice daily was started to address his facial nerve dysfunction; however, he progressed to H-B VI dysfunction and 2 days later returned to the operating room for tympanomastoidectomy and possible facial nerve decompression. Findings included an edematous EAC with normal appearing underlying bone as well as soft tissue filling the mesotympanum. A cortical mastoidectomy was performed with thickened, rubbery tissue identified filling the mastoid air cells. Similar soft tissue was removed from the epitympanum and sent for culture and pathologic analysis. No bony erosion or cholesteatoma was seen.
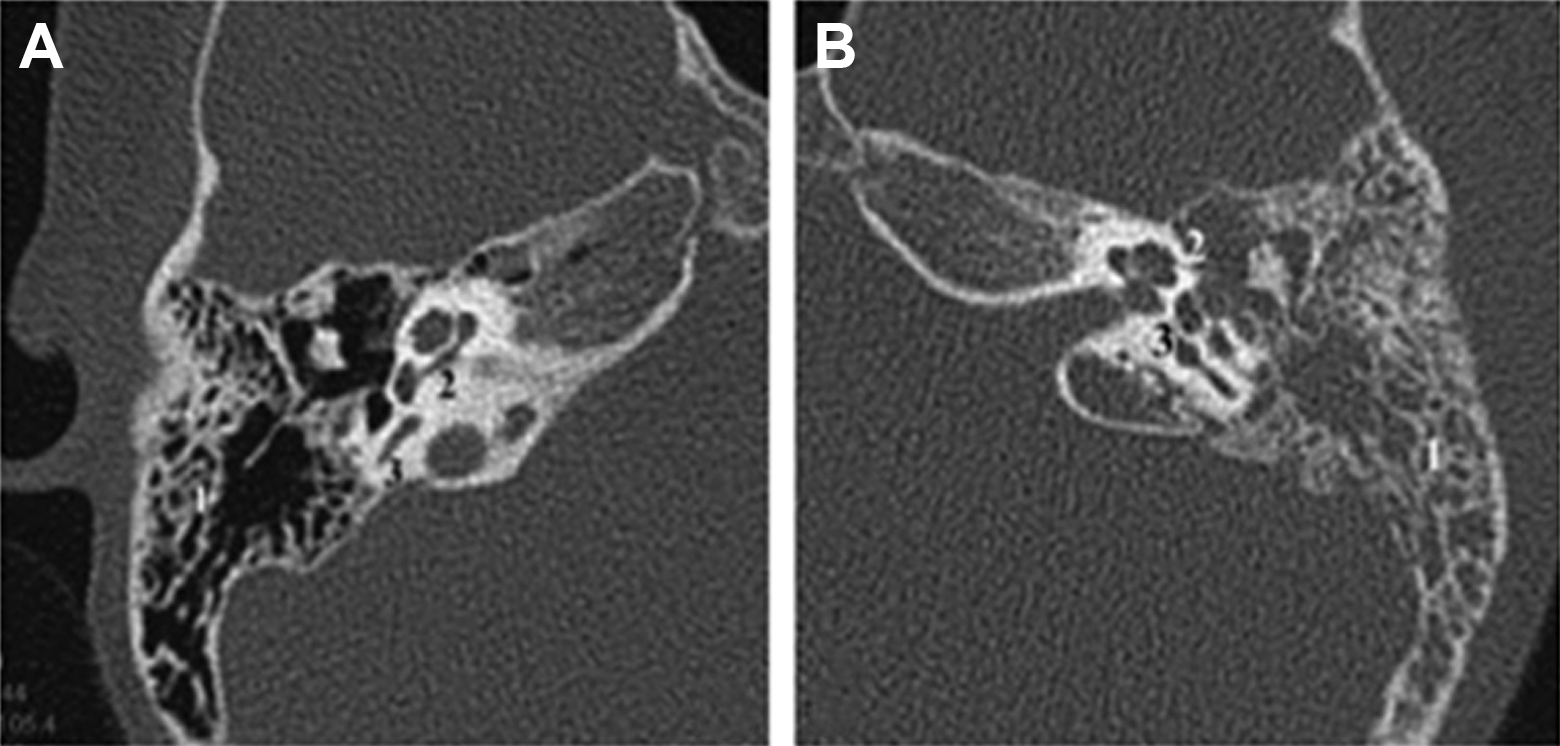
Preoperative computed tomography noncontrast computed tomography of the right (A) and left (B) temporal bones, axial images: Soft tissue density is seen in the left temporal bone with no erosion of mastoid septations (1), cochlea (2) or semicircular canals (3). There is a similar pneumatization pattern between the right and left sides.
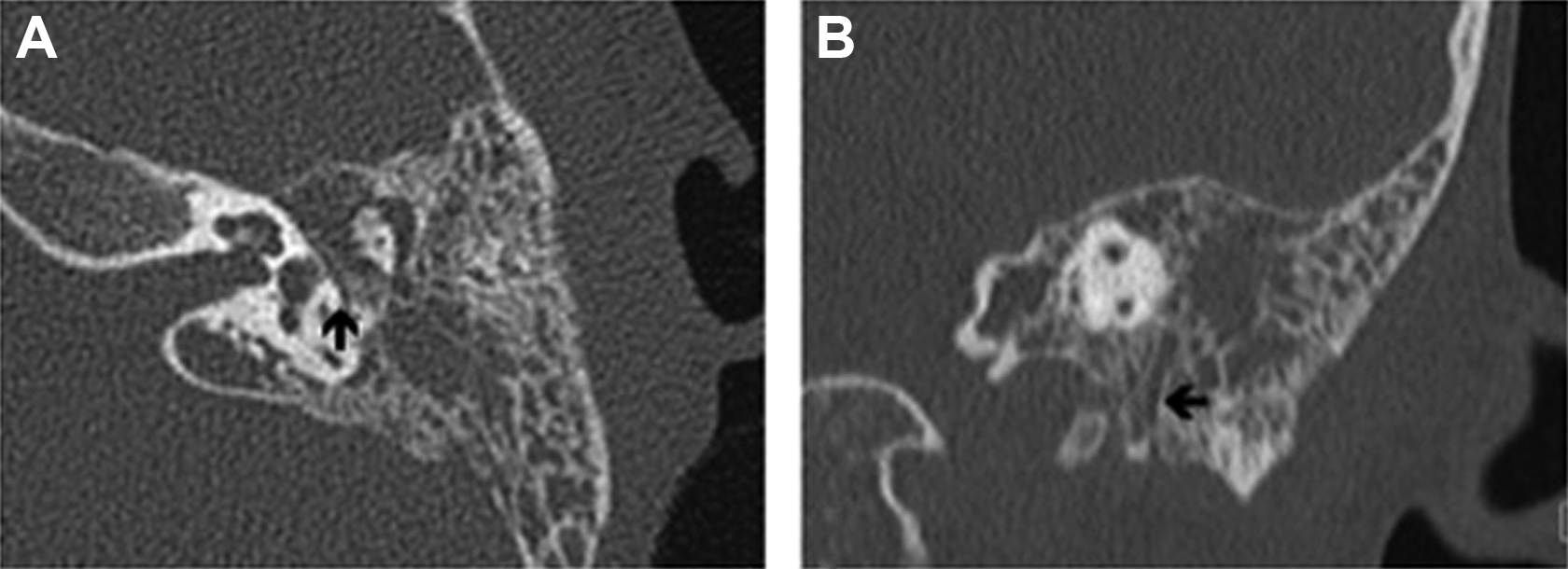
Preoperative computed tomography noncontrast computed tomography of the left temporal bone, axial (A) and coronal (B) images: The course of the left facial nerve through the fallopian canal appears unremarkable, including in the tympanic segment (A, arrow) and mastoid segment (B, arrow)
Postoperatively the patient remained afebrile and stable with unchanged facial paralysis. He was continued on systemic and topical antibiotics and prednisone until postoperative day 7, when histopathologic examination of the mastoid biopsy tissue confirmed BL based on a fluorescence in situ hybridization assay, in addition to morphologic and immunophenotypic correlation (Figures 3 and 4). Of note, immunohistochemical staining was negative for BCL2, TdT, CD34, which is consistent with BL.
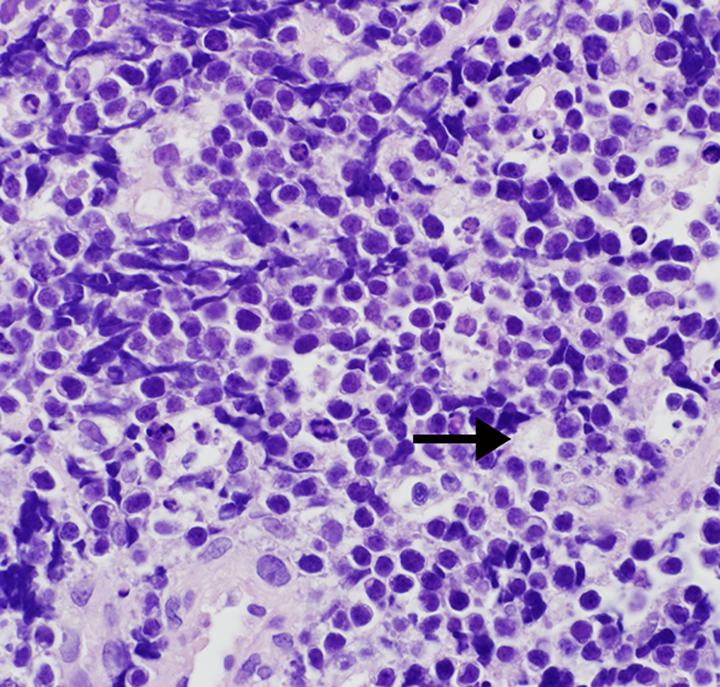
Representative hematoxylin and eosin stain of biopsy tissue demonstrating extensive submucosal infiltrate of monotonous partially viable small lymphoid cells with a high nuclear to cytoplasmic ratio, abundant mitoses, and some admixed tingible body macrophages (see arrow), which are also partially necrotic (image at ×600 magnification).
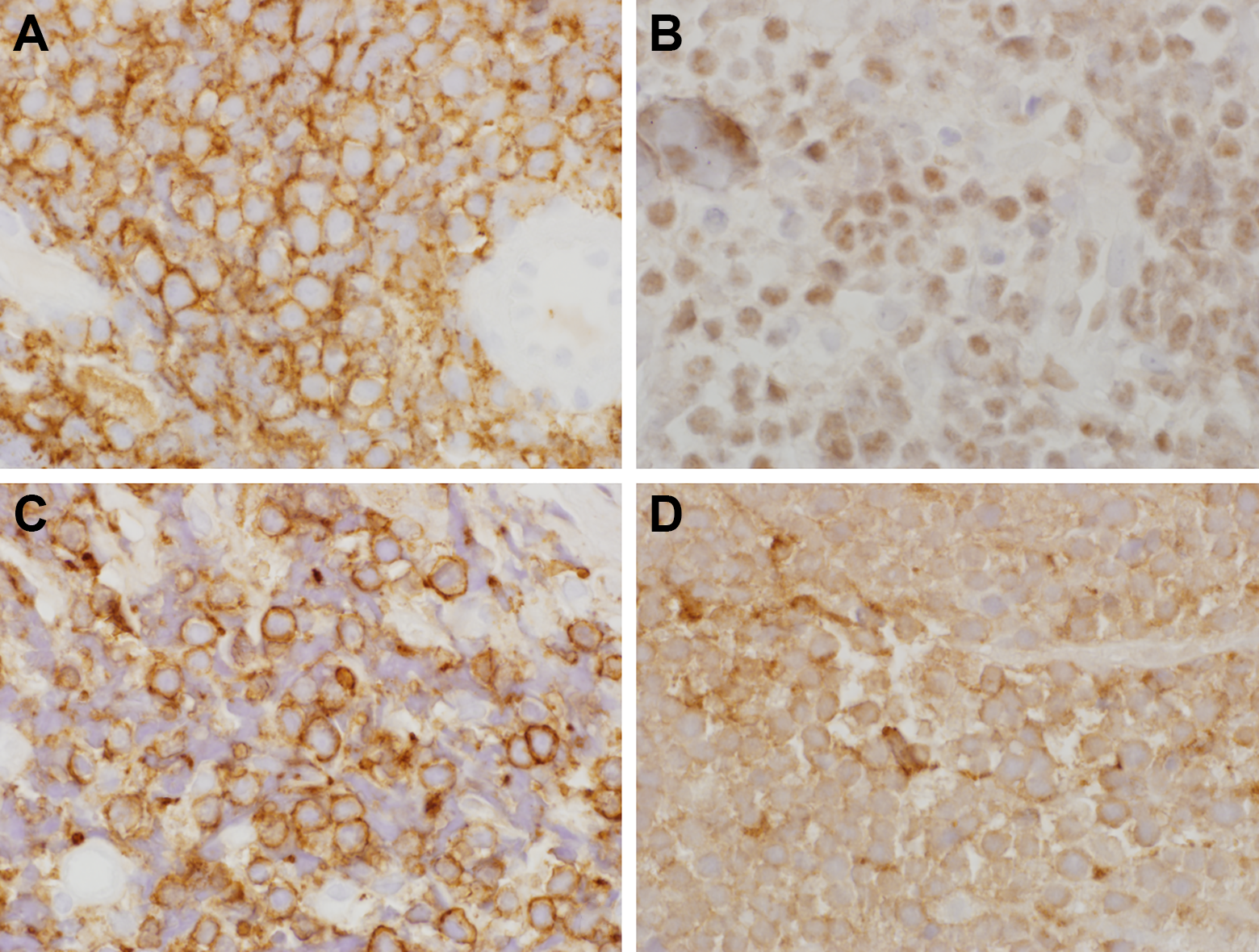
Immunohistochemical (IHC) stains of biopsy tissue. A, Positive cytoplasmic and cell staining for CD20, immunoperoxidase stain. B, Weak to moderate positive nuclear staining for MYC, IHC stain. C, Strong positive cytoplasmic and surface staining for CD43, immunoperoxidase stain. D, Weak positive cytoplasmic staining for CD10, IHC stain. Intensity of stains was variable secondary to substantial amount of necrotic tissue within the sample, a common feature of Burkitt Lymphoma (BL; images at ×960 magnification).
Subsequent oncologic work-up including positron emission tomography-CT demonstrated malignant involvement of the left periauricular lymph nodes, gastric and transverse duodenal walls, retroperitoneal para-aortic soft tissue, bilateral cervical lymph nodes, right paratracheal lymph nodes, and diaphragmatic lymph nodes, though on his previous contrasted CT, the lymph nodes of the head and neck were within normal limits. The patient developed ascites, bilateral pleural effusions, and pericardial effusions secondary to metastasis. Furthermore, he was found to have CNS-positive disease with initial lumbar puncture. Bone marrow was negative for tumor. Based on these evaluations, the patient’s diagnosis was consistent with stage IV, CNS-positive, metastatic BL of the temporal bone. He was Epstein-Barr virus negative.
Chemotherapy was initiated, including 6 courses of intensive intrathecal therapy with hydrocortisone, arabinosylcytosine, and methotrexate. Initially, the BL cells were cleared from the cerebrospinal fluid (CSF); however, CSF collected at the beginning of the third course of treatment was positive for lymphoma cells, raising concern for a suboptimal response to therapy. The patient demonstrated no evidence of disease after the sixth course of treatment but remained at high risk of refractory disease given evidence of persistent CNS lymphoblasts during his chemotherapy. He subsequently underwent allogenic bone marrow transplant incorporating cranial radiation for treatment consolidation.
His treatment course was complicated by iatrogenic hypofunction of the hypothalamic–pituitary axis, which required treatment with corticosteroid supplementation. He regained partial function of the superior division of the facial nerve and underwent facial reanimation surgery with hypoglossal nerve grafting to the lower division of the facial nerve performed at an outside institution. His most recent audiogram performed for ototoxicity monitoring during his chemotherapy demonstrated normal hearing below 8000 Hz bilaterally with some mild to moderate hearing loss bilaterally at frequencies greater than 10 kHz. At the time of this report, he was negative for recurrent or residual disease at approximately 2 years after initiation of chemotherapy.
Literature Review
PubMed, Web of Science, Google Scholar, and The Cochrane Library were searched from inception through December 2018 for the following MeSH terms: “lymphoma + temporal bone,” “leukemia + temporal bone,” “lymphoma + ear,” “leukemia + ear,” “ear + (leukemia OR lymphoma OR hematopoietic malignancy OR hematopoietic malignan*),” and “temporal Bone + (leukemia OR lymphoma OR hematopoietic malignancy OR hematopoietic malignan*).” Inclusion criteria were symptoms at primary presentation arising specifically from involvement of the temporal bone, patient age less than 18 years, and no other prior sites of disease. Exclusion criteria were studies not available in the English language, cadaveric or nonhuman studies, patients 18 years or older, and patients with a prior history of hematopoietic malignancy. Preferred Reporting Items for Systematic Reviews and Meta-Analyses 2009 guidelines were applied whenever possible. The search returned 929 unique references, 20 of which met inclusion criteria. All included studies were case reports or case series and comprised reports of 24 individual cases. Although several articles did reference the related literature at their time of publication, none included a systematic review or meta-analysis.
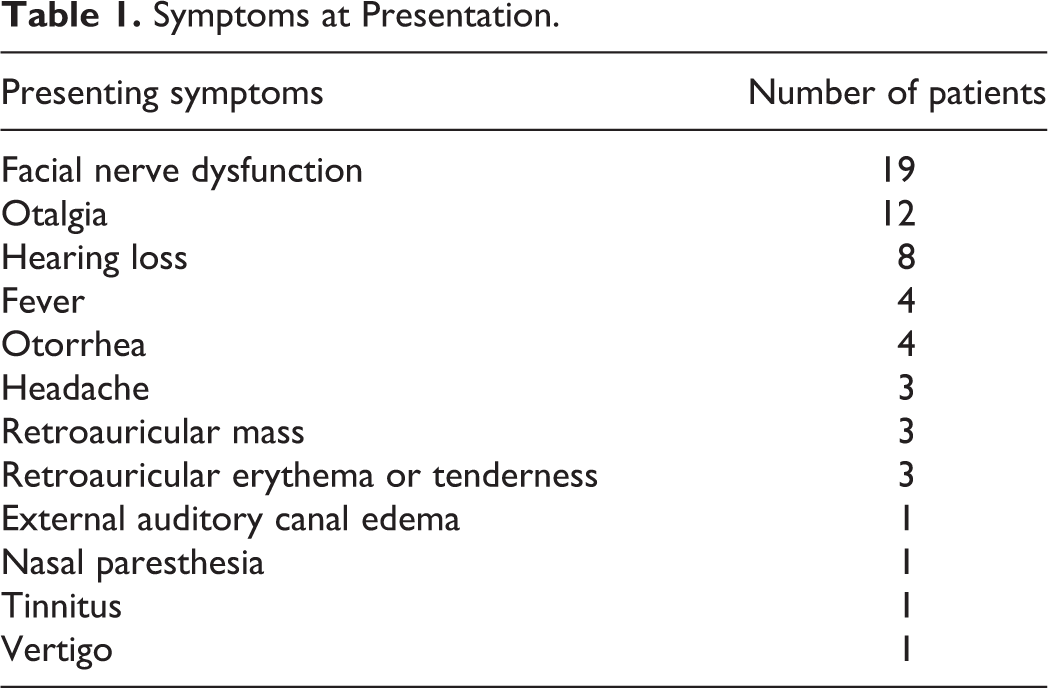
When the 24 literature cases were combined with our case, 4 classifications of lymphoid neoplasms associated with the temporal bone were noted, including 7 cases of B cell lymphoma,6-12 4 T cell lymphomas,13-16 4 BLs,17-19 and 10 leukemias.20-25 17 of 25 patients were male. Patient ages ranged from 8 months to 16 years old. All patients were described as otherwise healthy prior to presentation. There were a variety of signs and symptoms at presentation, and 16 patients were initially diagnosed with benign conditions (Tables 1 and 2). Though studies reported the presence of facial nerve dysfunction at initial presentation, the extent of function using the H-B grading scale was inconsistently reported. Five patients, including ours, received systemic corticosteroid for treatment of facial nerve dysfunction before the definitive diagnosis of malignancy.9,14,16,19 Of the 22 cases reporting laboratory results, 10 were notable for leukocytosis and 1 for thrombocytosis. Twelve cases reported abnormal findings on diagnostic imaging. The most common imaging findings included opacification of mastoid air cells (52%), the presence of a soft tissue or solid mass within the temporal bone (36%), and bony erosion (32%); opacification of the middle ear was inconsistently reported. Time to definitive diagnosis of malignancy varied greatly, ranging from 2 days 17 to 6 months, 13 after initial presentation, with a mean of approximately 6 weeks.
Symptoms at Presentation.
Initial Diagnoses.
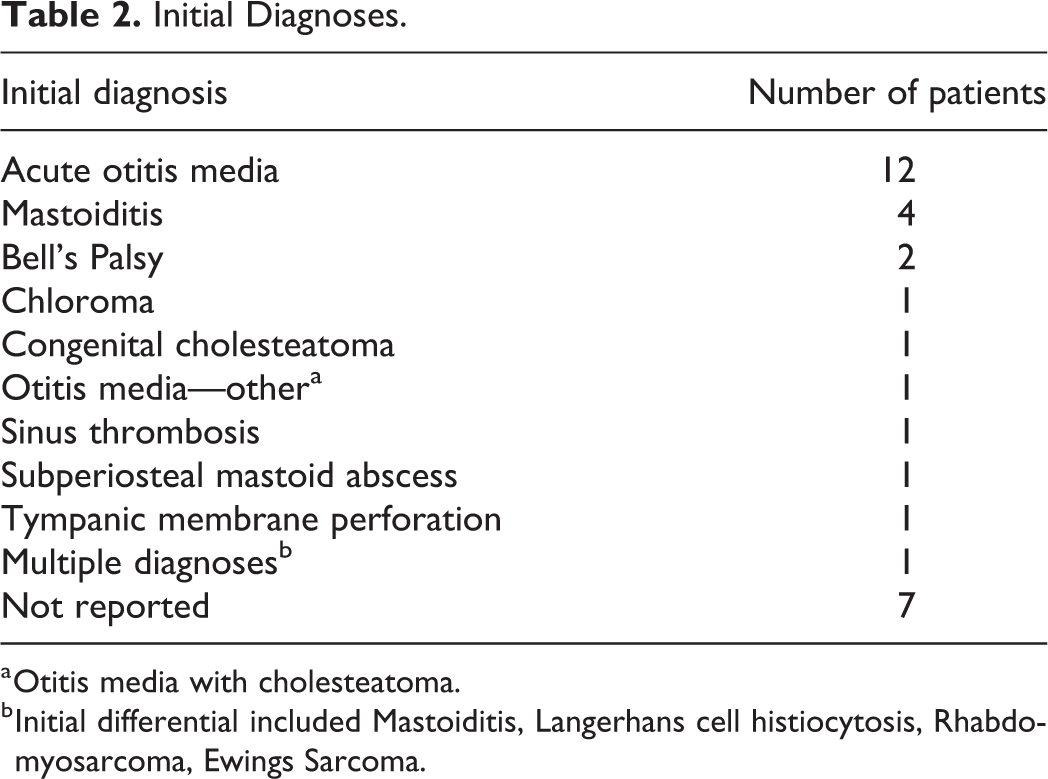
a Otitis media with cholesteatoma.
b Initial differential included Mastoiditis, Langerhans cell histiocytosis, Rhabdomyosarcoma, Ewings Sarcoma.
Prognosis and outcomes were variable. Two articles reported death at 1 month of leukemia 20 and 4 months secondary to BL. 17 The remainder of cases report varying lengths of survival and follow-up. One article did not report survival as the patient was referred to an outside institution; however, this patient was in remission at the time of referral. 22 Long-term hearing outcomes and the status of facial nerve function after definitive treatment were not consistently reported in the literature.
Discussion
Hematopoietic malignancies account for a substantial portion of pediatric malignancies. 1 When encountered in the head and neck, disease is typically found in the lymph nodes and much less commonly in bony anatomy.2-4 Interestingly, temporal bone involvement of these malignancies is often asymptomatic, even in cases where there is extensive destruction of the bone and other middle ear structures.2,3 When there are clinically significant symptoms from temporal bone involvement, most patients experience a triad of otalgia, periauricular swelling, and facial paresis. 4
Although dissemination of hematopoietic malignancies to the ear and mastoid is not uncommon, primary presentation of pediatric hematopoietic malignancies in the ear and mastoid is rarely reported in the literature. In general, primary malignancies arising in the temporal bone only account for 0.2% of all head and neck tumors. 13 Due to the paucity of reports and the rarity of the condition, the exact incidence of primary pediatric hematopoietic malignancy presenting with symptoms solely related to the involvement of the temporal bone is unknown.
Overall, the most common initial diagnoses for patients in this data set were AOM and/or mastoiditis. This is mostly likely due to the common presenting symptom of otalgia. It is notable that only a third were reported with subjective hearing loss as a presenting symptom, only 3 of which had audiometric data reported. In addition, some abnormal findings on CT imaging may be nonspecific for malignancy, such as mastoid opacification and even bony erosion. Unlike typical AOM/mastoiditis, however, facial nerve paralysis was the most common presenting symptom in our cohort of patients. Due to the small number of cases and variability in data reporting, we do not draw strong conclusions regarding prognosis, or outcomes of facial nerve function and hearing.
The high rate of misdiagnosis in these cases has implications for clinical practice, both for delayed diagnosis and treatment of malignancy, but also to avoid potentially risky interventions. Most notably, systemic corticosteroid often is administered for inflammatory temporal bone conditions causing facial nerve dysfunction; however, in hematopoietic malignancy, steroid may further delay diagnosis by temporarily relieving symptoms or even precipitate an adverse event such as tumor lysis syndrome.
With these limited data, it is difficult to draw definitive conclusions for practice. Specifically, we recognize that obtaining definitive tissue for diagnosis may not be possible or practical in all cases prior to administering treatment for presumed infectious/inflammatory conditions. Based on the results in this series, we recommend strong consideration of malignancy in the differential diagnosis prior to administering systemic corticosteroid in cases where facial nerve dysfunction is present without subjective hearing loss, or when imaging is not entirely consistent with benign disease, particularly given the paucity of data supporting improved outcomes with administration of steroid for facial nerve dysfunction.26,27
Conclusion
Our literature review and case report demonstrate frequent initial misdiagnosis of hematopoietic malignancy with primary presentation in the temporal bone, often with normal laboratory values and/or imaging consistent with infectious or inflammatory disease. Facial nerve dysfunction, abnormalities on imaging, and normal hearing are frequent in these cases and should increase clinical suspicion for malignancy. Malignancy should be considered in the differential diagnosis prior to administering systemic corticosteroid therapy for facial nerve dysfunction, due to the risk of tumor lysis syndrome and the potential for delaying appropriate therapy.
Footnotes
Acknowledgments
The authors gratefully acknowledge the contributions of Dr. Nathan Boyd, Dr. John Kuttesch, and Dr. Kathryn Foucar for their participation in the care of this patient and intellectual contribution to the manuscript.
Authors’ Note
BSH, JHH, and DAM performed chart review and data extraction. All authors contributed to preparation and review of the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.