
Abstract
Angiolymphoid hyperplasia (AH) was first described by Wells and Whimster in 1969 as a benign vasoproliferative pathology with a varied infiltrate of eosinophils, lymphocytes, and plasmatic cells. Clinical presentation has been described in the literature as small red-bluish nodules, less than 3 cm in diameter that can bleed in 25% of the cases and be pruritic and painful in 37% and 20% of the cases, respectively. Particularly, AH can appear in the ear; nevertheless, other regions have been affected, including the scalp, lips, tongue, orbit, muscle, and bone. Most of these cases have occurred in adults with an unknown etiology; however, an inflammatory process has been associated in approximately 20% with eosinophilia. No malignancy has been reported.
Case Report
This is an unusual case of a 24-year-old woman with multiple reddish nodules of 1 to 2 cm in diameter in the external auditory canal, specifically in the concha that extended to the cartilage, tragus, and posterior region of the earlobe, as seen in Figure 1. The resected area left a complex defect which was reconstructed with a retroauricular flap and a full thickness skin graft in the same surgery with preservation of the structure and function.
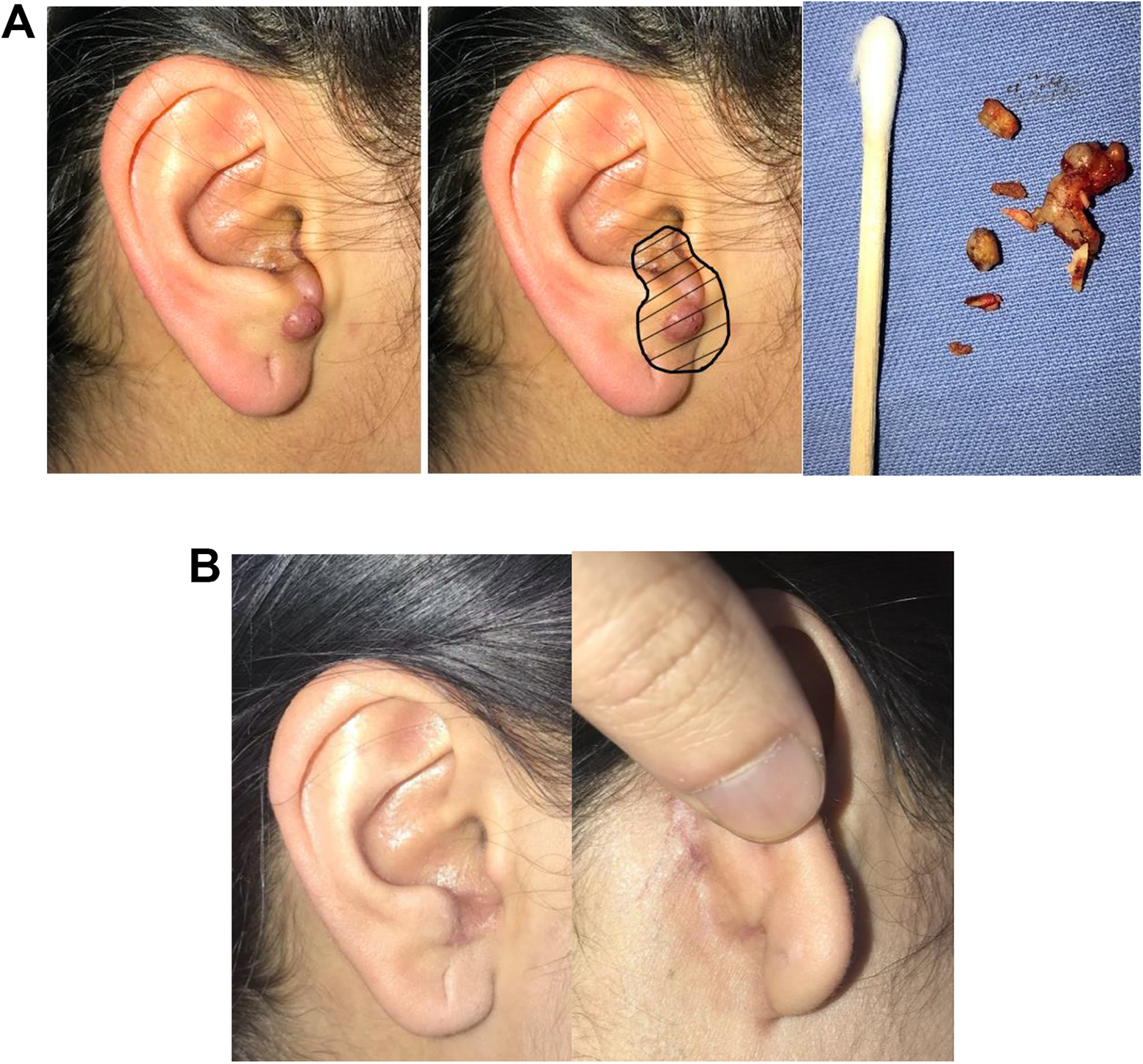
A, Reddish nodules in the external auditory canal with involvement of the concha and tragus. The resected lesions are marked in black with the tissue sent for pathology study as seen in the right picture. B, Reconstruction of the complex defect after 8 months of surgery with no new lesions.
Surgical Technique
A wide resection was made until macroscopically healthy tissue was visible, with partial cartilage surgical removal. The residual complex defect was reconstructed with a skin flap from the ipsilateral earlobe, specifically for coverage of the most distal portion, taking a retroauricular full-thickness skin graft that enabled us to restore the anatomy and function of the aesthetic unit. Healing of the patient was satisfactory. At 6 months postsurgery, she had a recurrent skin lesion handled with a simple resection and secondary healing of the affected area. One year after the first intervention, she has no new lesions.
Discussion
Angiolymphoid hyperplasia (AH), also known as epithelioid hemangioma, nodular angioblastic hyperplasia with eosinophilia, pseudopyogenic granuloma, or histiocytic hemangioma, 1,2 is an uncommon vascular proliferative disorder. Treating it becomes challenging for a number of reasons. Its growth is insidious in the submucous layer of the skin suggesting a benign neoplasia. 3 Microscopically, it is comprised of subcutaneous nodules with abnormal capillary vasculature growth near muscle arteries with increased reticulin formation and rare fibrosis 1,2,4,5,6 associated with an immature fibrovascular stroma with lymphocytic infiltrate, eosinophils with mastocytes, and mucinous deposits in the histologic sections. 3 Kempf mentioned this medical condition as a lymphoproliferative disorder of CD4T cells. 8 Endo et al, as well, described a high metabolic rate of the endothelial cells. 6 Trauma precedes the tumor in approximately 10% of the cases, reported by as a complication of ear piercing. 1 In almost two-third of the patients, it is present in the head and neck with no reports of lesions greater than 10 cm. 7 The ear is the most common aesthetic unit implicated, with the post auricular region affected in 13.8% of the cases and the preauricular and helix regions affected in 7.4% and 7.3% of cases, respectively. Young adults, from 33 to 45 years old, have the highest incidence of presentation. Confusion surrounding the etiology of AH has been linked it as an idiopathic disease. 1,2
Imaging studies, like tomography, magnetic resonance, and angiography, can determine the extension of the lesion; however, the gold standard for diagnosing AH with histological sections. 2 Differential diagnoses can be divided into benign etiologies, like atheroma, keloid scars, sarcoidosis, keratoacanthoma and hemangiomas, or vasoproliferative disorders, like retiform hemangioendothelioma, angioendothelioma, malignant endovascular papillary endothelioma, Kaposi sarcoma, and Kimura´s disease. The latter can be differentiated by the absence of endothelial and epithelioid cells with well distinguished lymphoid follicles. 1,2
There is a reported recurrence of 33% with surgical removal, from 50% to 55% with laser and CO2 therapy and the highest rate was with intralesional infiltration of corticosteroids (79.1%). 4
Conclusion
These uncommon lesions presenting as benign tumors require relatively aggressive treatments for achieving a complete resection because of their high rates of recurrence, with surgical excision having the lowest rate of all therapies. In this case, since there was a complex defect secondary to the resection of the lesion, the skills of the plastic surgeon were needed to reconstruct the ear with minimal scarring and deformity.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.