
Abstract
The most common cause of cerebrospinal fluid (CSF) rhinorrhoea is damage to the skull base with a dura mater’s rupture due to an accident or an iatrogenic injury. This applies to over 96% of cases. Other possibilities that can lead to CSF leakage are neoplasms of the nasal cavity, paranasal sinuses, and nasopharynx. Although prostate cancer spreads to bones, cranial metastases to paranasal sinuses are extremely rare. We present a case of an 83-year-old patient with CSF leakage due to infiltrating metastatic prostate cancer. Cerebrospinal fluid rhinorrhea turned out to be the first symptom of prostate cancer metastasis. Diagnostic and treatment strategies are presented in the discussion.
Introduction
Cerebrospinal fluid (CSF) rhinorrhea is defined as a leakage of cerebrospinal fluid into the nasal cavity. The mechanism is based on the skull base’s damage with the dura mater’s simultaneous rupture. Consequently, this leads to a CSF leak between the subarachnoid space and the nasal cavity. 1 According to the mechanism, we divide CSF rhinorrhea into 2 main groups: traumatic and nontraumatic. The most common cause of CSF rhinorrhea is trauma, which accounts for 96% of all rhinorrheas. The vast majority of this is due to accidents (80%). The rest of rhinorrheas usually appear as complications after functional endoscopic sinuses surgeries or neurosurgical interventions. 2 On the contrary, nontraumatic causes may be secondary to increased intracranial pressure (ICP), which account for 55% of nontraumatic rhinorrhea, while the remaining 45% of cases are associated with normal ICP values. Nontraumatic rhinorrhea can occur with other underlying conditions such as empty saddle syndrome, meningocele, osteitis after radiotherapy, or idiopathic rhinorrhea. Tumors located in the skull base area may also lead to the CSF leakage due to a direct infiltration and damage to bone structures or indirectly through increased ICP. 3 Metastases to the nasal cavity and paranasal sinuses are much less common than primary neoplasms in this area. In specific, most common metastatic tumors originate from the kidney, thyroid, breast, lung, and prostate. 4
Case Report
An 83-year-old patient was referred to the Otolaryngology Department with persistent clear, watery nasal discharge. A few days earlier, he was admitted to the Neurological Department due to persistent headaches. On admission to the Otolaryngology Department, he reported pain localized in the forehead and base of the nose. Leakage of a colorless, transparent fluid from both nasal cavities was observed. It occurred primarily when the head was tilted forward. There were no previous injuries or surgeries of the head or neck region in the patient’s history. The patient was previously diagnosed with an advanced, poorly differentiated adenocarcinoma of the prostate: Gleason Score 9 (4 + 5). The pathological slide is presented in Figure 1.
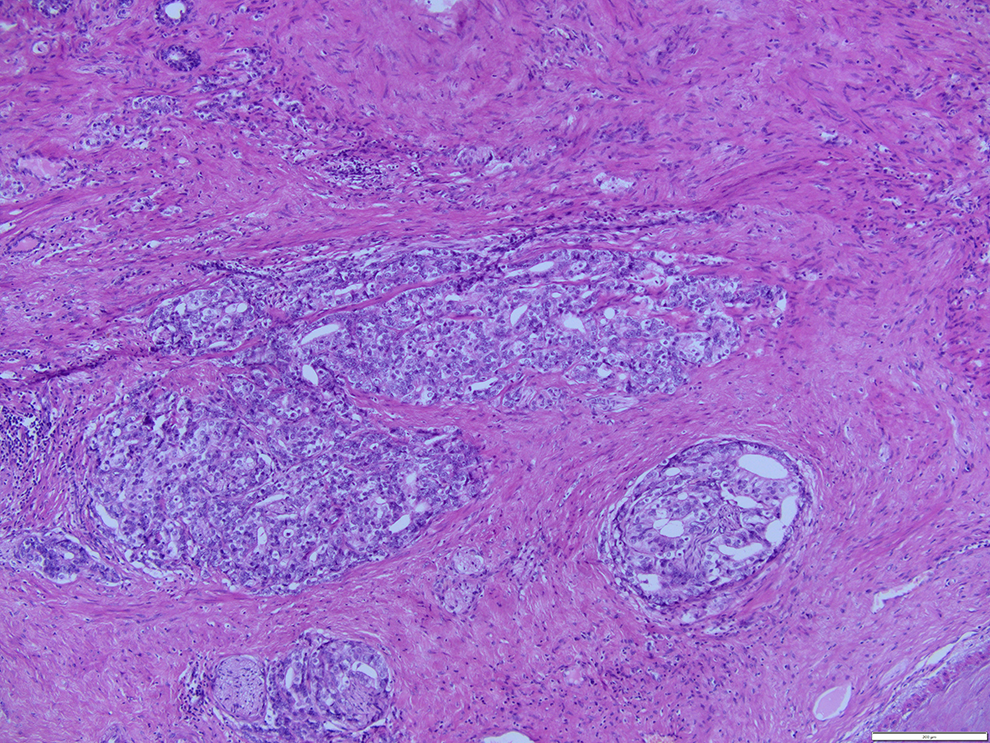
Histopathological examination revealed a poorly differentiated adenocarcinoma of the prostate gland—Gleason Score 9 (4+5)/risk grade group V.
Nevertheless, the course of the neoplastic disease had been asymptomatic. Based on the medical history and physical examination, there was a suspicion of CSF leakage due to infiltrating metastatic prostate cancer. To determine leakage localization, the patient had a computed tomography (CT) and magnetic resonance imaging (MRI) of the head and neck. The radiological examinations confirmed a bone lesion (defect measuring 26 × 12 × 15 mm affecting the clivus, the vault of the pharynx, and the posterior wall of the left sphenoid sinus). The changes mentioned above are shown in Figures 2 and 3. Nasal endoscopy was performed, and no pathological lesions were found. The picture from the procedure is presented in Figure 4. Even though we eventually found multiple bone metastases (shown in Figure 5), metastases to the head were the only ones to give symptoms.
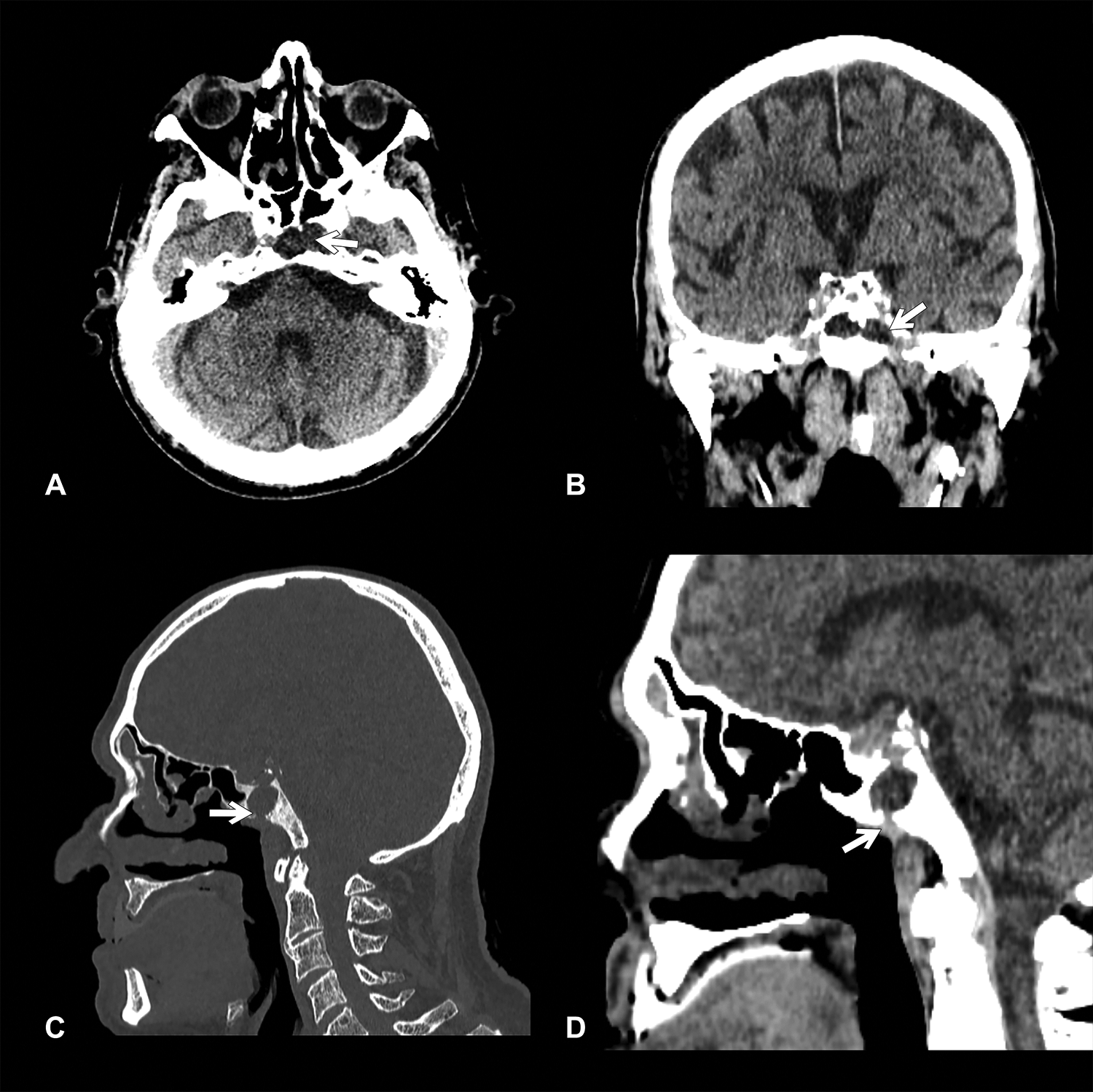
Computed tomography (CT) scans of the head presenting destruction of bones (A) axial plane in tissue frame; (B) coronal plane in tissue frame; (C) sagittal plane in bone window; (D) sagittal plane in tissue window.
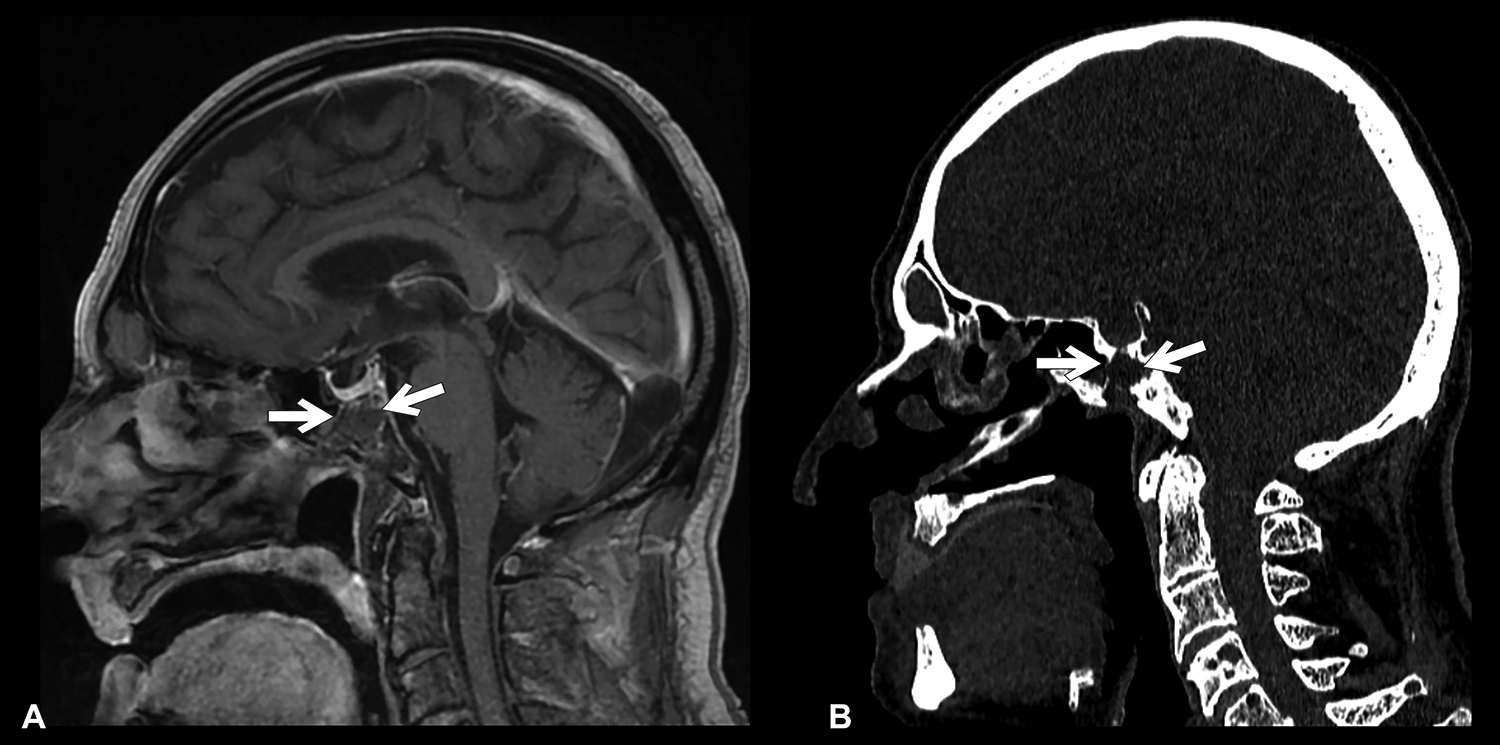
(A) Magnetic resonance imaging (MRI) T1 sagittal plane showing metastatic mass to the sphenoid sinus; (B) computed tomography (CT) scan showing bone lesion.
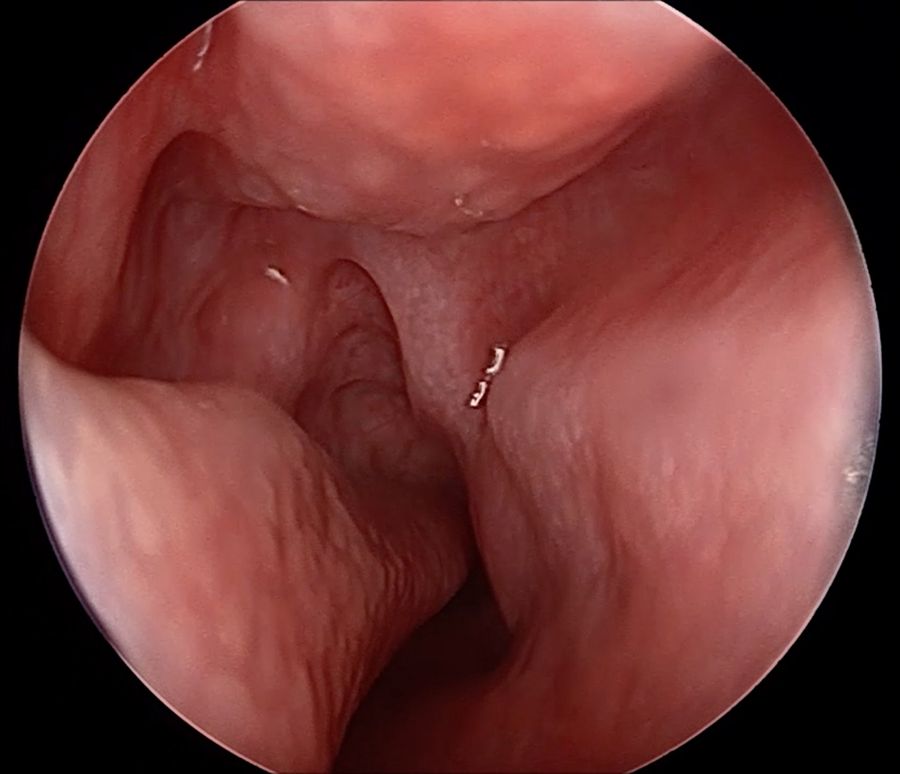
Endoscopic examination of the sphenopalatine recess with a visible shining spot of cerebrospinal fluid leakage.
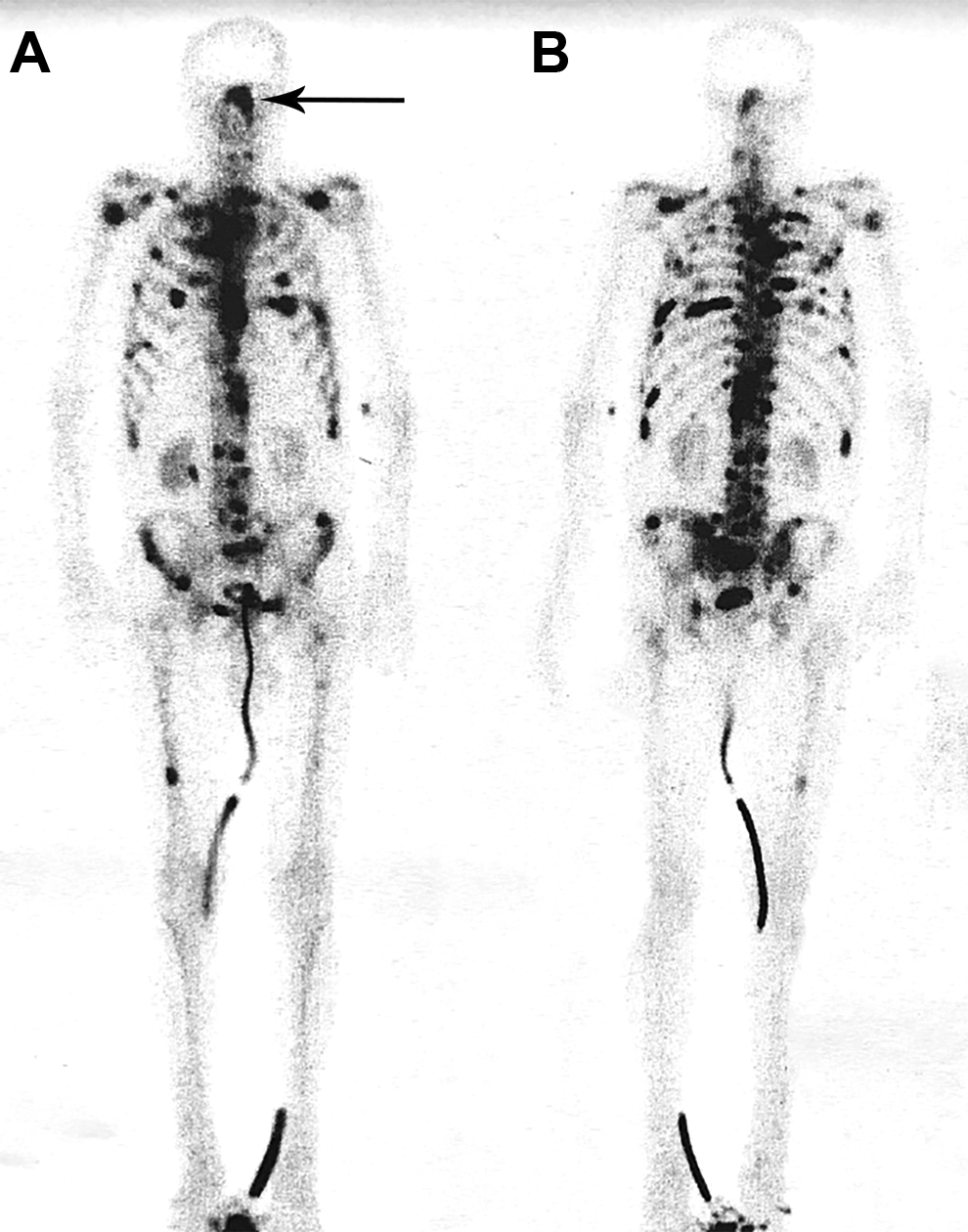
Bone scintigraphy showing multiple metastases, including to the head. Arrow is pointing to the metastasis to the sphenoid sinus. A-anterior, B - posterior.
Due to the case’s complexity, a senior staff meeting was appointed, including a neurosurgeon, oncologist, otorhinolaryngologist, and urologist. Consequently, it was decided to introduce a conservative treatment. Prophylactic antibiotic therapy with cefuroxime (1.5 g three times a day, intravenously) was implemented. The patient received advice to lay down with his head elevated at an angle of 30 degrees. He was also advised to avoid activities that may increase ICP, such as sneezing, coughing. After spontaneous cessation of rhinorrhea, the patient was discharged on the 10th day. The oncological council decided to continue hormonal therapy and symptomatic treatment under the palliative care teams’ control. The patient was followed up for 6 months—during this time, there was no CSF leak recurrence.
Discussion
The golden standard in the diagnosis of CSF is the detection of β2-transferrin. This substance is detected almost exclusively in the cerebrospinal fluid, and its determination is characterized by high sensitivity and specificity. 1,5 In the diagnostic process, it is necessary to determine the leakages’ exact location. Nowadays, CT and MRI examinations are adequate for this purpose. 1 The former, in the case of osteoclastic lesions, will be manifested by a bone defect. The latter allows identifying the soft tissue mass itself. Chan and coauthors investigated that in every case in which CT showed an evident bone loss, β2-transferrin was also positive. 5 Thus, in the case of limited availability of β2-transferrin testing, it is worth performing a CT scan at an early stage, as immediate diagnosis and treatment of cerebrospinal fluid leakage significantly reduce the risk of meningitis. 6 Changes in CT appear in approximately 80% of patients with positive β2-transferrin. 5 The differential diagnosis of lesions in the paranasal sinuses is complex. Nowadays, when neoplastic diseases are one of the dominant causes of death globally, we should carefully focus on the patients’ oncological history. In the review of 82 cases of patients with metastases to the paranasal sinuses’ bones, the maxillary sinus was the most frequently affected area. On the contrary, the rarest metastatic destination was the sphenoid sinus. The most common metastasizing cancer (65% of cases) was kidney cancer. 4
Prostate cancer cells show a strong predilection to spread to the bones and usually metastasize to the spine. In the presented case, the defect in the sphenoid sinus wall that leads to rhinorrhea was caused by the osteolytic nature of the specific tumor. It is believed that the primary mechanism of bone destruction is an increased level of PTHrP (parathyroid hormone-related peptide), which induces bone resorption by RANKL (receptor activator of nuclear factor-kappa B ligand). 7 In most prostate cancer cases, metastases usually have an osteoblastic character, even though an osteoclastic component accompanies it. However, in patients with poorly differentiated cancer, the osteoclastic feature may be dominant—as in the described case. When metastatic, poorly differentiated prostate cancer is diagnosed, management is usually palliative. It focuses on reducing tumor mass, preventing further metastases, and relieving symptoms associated with metastases such as pain or pathological bone fractures. 8 Treatment of nasal rhinorrhea depends on the CSF leak cause and the location and extent of the bone loss. In most cases of limited lesions, conservative treatment is implemented. 9,10 In such a case, patients are administered antibiotic prophylaxis. The patient’s head is positioned at an angle of 30 degrees, and activities that increase ICP, such as sneezing or coughing, are avoided. The expected improvement occurs within 7 to 10 days. The risk of meningitis is increased significantly with fluid discharge lasting more than 7 days. 9 The analysis of Yilmazlar and coauthors found that conservative treatment is most often effective. However, surgical intervention was required in approximately 9% of patients. It concerned traumatic patients with the most significant neurological deficits. 10 In such a case, endoscopic techniques are preferred—they are more effective and less invasive than open procedures. 3,9 Currently, only extensive injuries related to fracture of the anterior skull bones indicate open procedures. 3
Conclusion
According to the presented case, in rhinorrhea (not only nasal), rare causes such as cancer should also be considered. As the incidence of oncological diseases increases, we should look at the patient even more holistically. Low-differentiated neoplasms often have an unusual and less characteristic manifestation. In the case mentioned above, CSF rhinorrhea turned out to be the first symptom of prostate cancer metastasis.
Footnotes
Authors’ Note
Informed consent was obtained for experimentation with human subjects. Work was conducted according to the World Medical Association Declaration of Helsinki. Collegium Medicum Ethics Committee in Bydgoszcz proved approval (document’s number: KB 88/2020).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.