
Abstract
Background:
Cerebrospinal fluid rhinorrhea in the sphenoid sinus lateral recess is a rare occurrence and poses unique challenges due to limited surgical access for surgical repair.
Objective:
To report our experience of surgical repair of cerebrospinal fluid rhinorrhea in the sphenoid sinus lateral recess through an endoscopic endonasal transpterygoid approach with obliteration of the lateral recess. To evaluate the efficiency of this surgical procedure.
Methods:
A retrospective study. Twelve cases with cerebrospinal fluid rhinorrhea in the sphenoid sinus lateral recess were reviewed. Assisted by image-guided navigation, cerebrospinal fluid rhinorrhea was repaired through an endoscopic endonasal transpterygoid approach, with obliteration of the lateral recess. Complications and recurrence were recorded. Medical photographs were used.
Results:
This surgical approach provided a relatively spacious corridor to dissect the sphenoid sinus lateral recess and do postoperative surveillance. The repair area completely healed in 3 months after surgery. Cerebrospinal fluid rhinorrhea in the sphenoid sinus lateral recess was successfully repaired on the first attempt in all cases (100%). No main complications or recurrence was observed during a mean follow-up time of 40.3 months.
Conclusion:
The endoscopic endonasal transpterygoid approach gives appropriate access for the treatment of spontaneous cerebrospinal fluid rhinorrhea in the sphenoid sinus lateral recess. Multilayer reconstruction of a skull base defect with obliteration of the lateral recess is a reliable and simple method.
Keywords
Introduction
The sphenoid sinus lateral recess (SSLR) is defined as a measurable indentation caused by pneumatization of the pterygoid process lateral to the Vidian canal to foramen rotundum line (V-R line). 1 Complete bony dehiscence of the SSLR may be associated with cerebrospinal fluid (CSF) rhinorrhea with or without meningoencephalocele. 2 Cerebrospinal fluid rhinorrhea originating from the SSLR is a rare entity, with a frequency of 7.7% among all skull base CSF leaks. 3 The management of a CSF rhinorrhea in the SSLR through an endoscopic approach faces various challenges due to its relatively difficult angled intranasal access, poor exposure, and intricate neurovascular relationships. 4
The endoscopic endosnasal transpterygoid approach (EETPA) provides access to the SSLR through the posterior wall of the maxillary sinus and the pterygopalatine fossa (PPF), and lesions could be sufficiently exposed even in a well-pneumatized lateral recess. Therefore, it is possible to repair the CSF rhinorrhea in the SSLR through this approach with a wide surgical field of view and high success rate.5-7 On the other hand, multilayer reconstruction of a skull base defect is currently an accepted method. However, reports about repair of CSF rhinorrhea in the SSLR through EETPA with obliteration of the lateral recess are still rare.
This study aimed to describe our experience over a 5-year period in surgical repair of CSF rhinorrhea originating from the SSLR through an EETPA with obliteration of the lateral recess aided by image-guided navigation, with special focus on the surgical approach, reconstruction techniques, surgical outcomes, and complications.
Patients and Methods
Clinical Data
This is a retrospective study. The medical records of 12 cases with CSF rhinorrhea originating from the SSLR were reviewed from November 2014 to December 2019 at the Department of Otolaryngology–Head and Neck Surgery, Tongji Hospital, Tongji Medical College, Huazhong University of Science and Technology. The patients were sorted by admission time.
Diagnosis was based on history and clinical and imaging findings. All patients presented with rhinorrhea, and fluid samples collected were analyzed to confirm the presence of an active CSF rhinorrhea. High-resolution computerized tomography and magnetic resonance imaging (MRI) were used to identify the defect in the skull base (Figures 1 and 2).
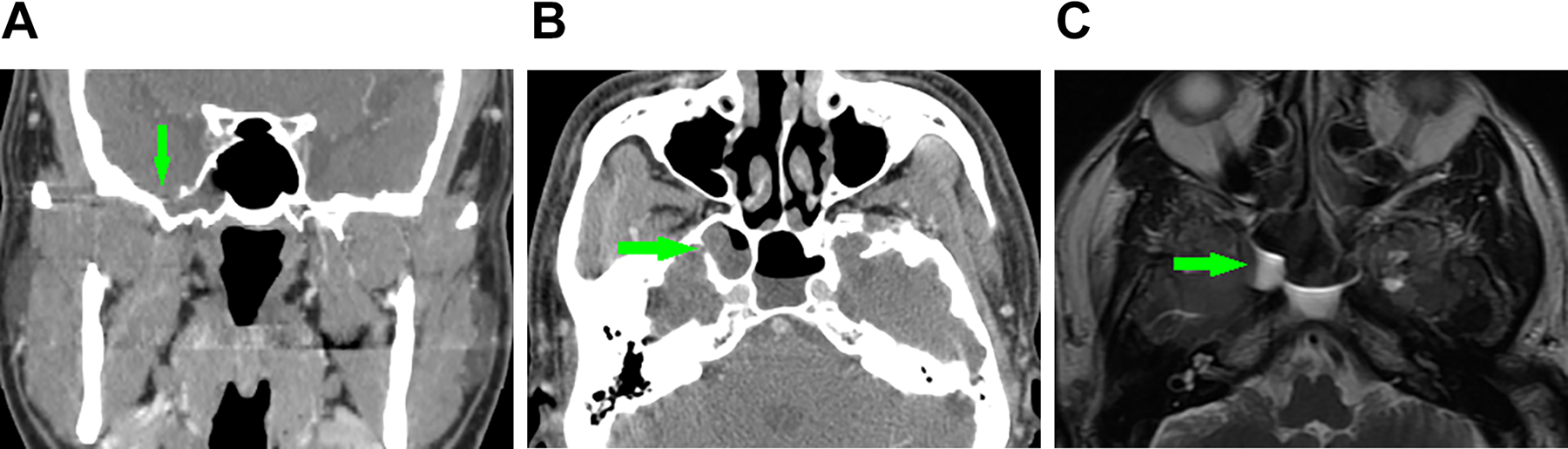
Preoperative images of case 9. (A) Coronal computed tomography (CT) images showing a defect (arrow) in the right sphenoid sinus lateral recess (SSLR). (B) Axial CT images showing a defect (arrow) in the right SSLR. (C) Axial T2-weighted (T2WI) magnetic resonance imaging (MRI) showing a cerebrospinal fluid (CSF) leak (arrow) in the sphenoid sinus.
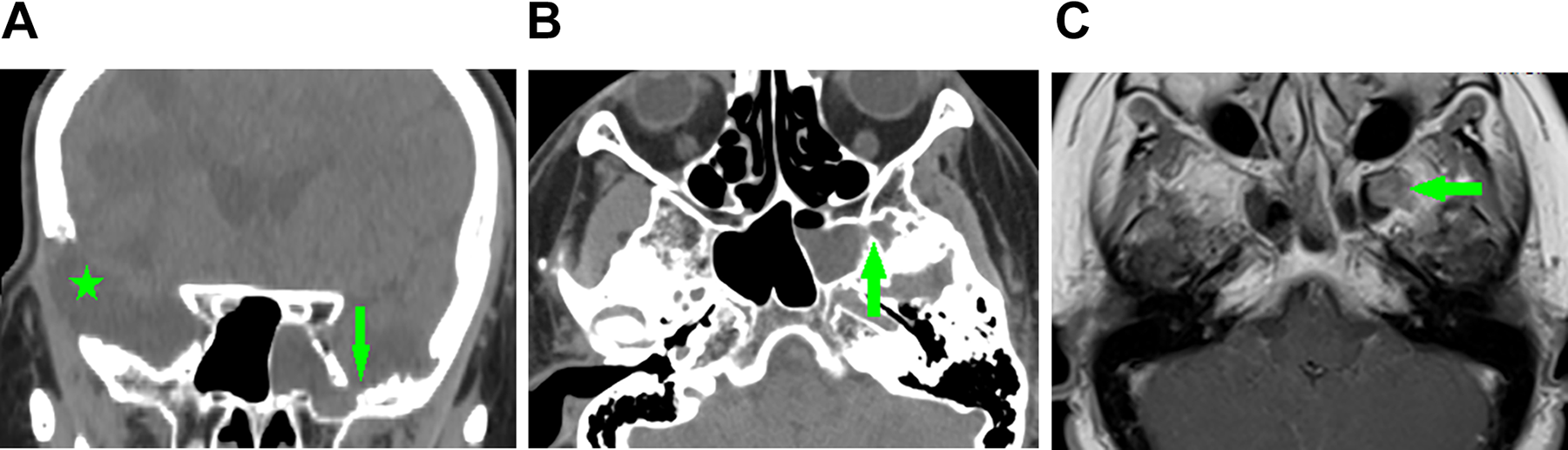
Preoperative images of case 12, who previously had a resected meningioma in the right frontal lobe. (A) Coronal computed tomography (CT) images showing a defect (arrow) in the left sphenoid sinus lateral recess (SSLR), and a previous craniotomy for meningioma resection (star). (B) Axial CT images showing a defect (arrow). (C) Axial T1-weighted (T1WI) magnetic resonance imaging (MRI) showing meningoencephalocele (MEC) in the left SSLR (arrow).
The clinical data were collected from operative reports, hospital charts, preoperative examination, and postoperative follow-up. This study was approved by the Ethical Committee of our hospital.
Surgical Procedure
Each patient was supine with the head in a neutral position and a 10° to 15° adduction to the patient’s right. A tracheal tube was fixed on the patient’s left. The nasal cavity mucosa was sterilized with 0.5% povidone-iodine solution. Then, the nose was packed with cotton pledgets soaked in 0.05% xylometazoline solution. The image guidance (Medtronic Navigation, Inc) was used. Abdominal subcutaneous fat was resected with a skin incision from the right lower abdominal quadrant.
All patients received the surgery to repair the CSF rhinorrhea in the SSLR through an EETPA aided with image-guided navigation. The procedure began with an uncinectomy, followed by a wide maxillary antrostomy and a complete ethmoidectomy. A wide sphenoidotomy was extended laterally to the V-R line until the SSLR could be observed with an angled endoscope (Figure 3A). Then, the posterior maxillary wall was removed outward to expose the PPF. The PPF fat was cauterized with a bipolar posteriorly toward the pterygoid plates. The base of the pterygoid process was drilled off and extended laterally until a complete direct exposure of the SSLR was obtained.4,7,8 The defect localization was confirmed with navigation (Figure 3B).
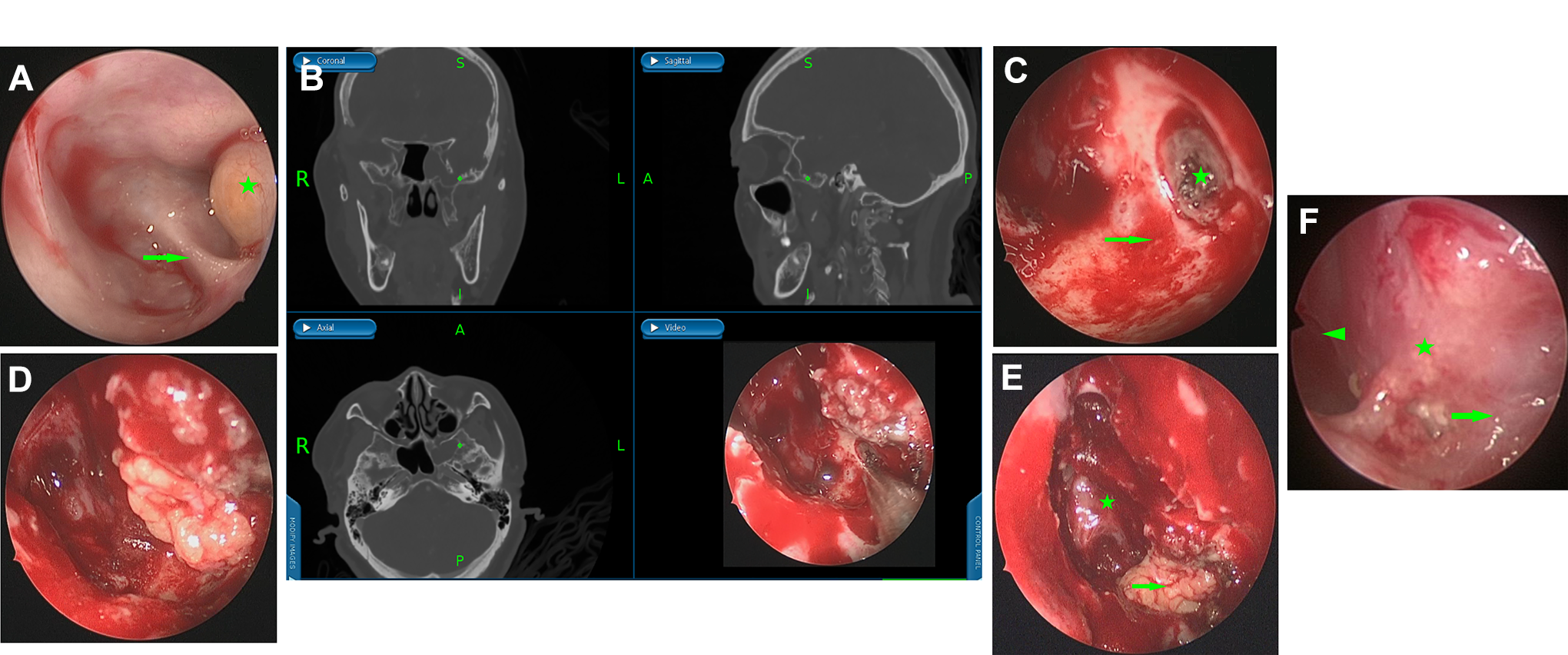
Intraoperative and postoperative endoscopic views of case 12. (A) MEC (star) in the left sphenoid sinus lateral recess (SSLR) and Vidian canal (arrow). (B) The lesion site was pointed out by navigation. (C) MEC and the mucosa around the defect were removed (arrow), and the skull base defect was revealed (star). (D) A piece of fat was inserted in the epidural space. (E) The SSLR was obliterated with fat (arrow) and the medial sphenoid sinus (star) was left open. (F) Sphenoid sinus (triangle), obliterated SSLR (star), and maxillary sinus (arrow) 3 months after surgery.
If a meningocele or meningoencephalocele was present, the prolapsed soft tissue was removed to the level of the bony defect. For all patients, the mucosa of the SSLR was completely stripped. The bone should be smoothed with a diamond burr around the defect to help nourishment and stability (Figure 3C). Then, a procedure of multilayer reconstruction with obliteration of the SSLR with fat was performed. Firstly, a small fat graft, custom-shaped to fit the defect was placed in the epidural space (Figure 3D). Then, the SSLR was obliterated with residual fatty tissue, with the medial sphenoid sinus remaining open (Figure 3E). Lastly, fatty tissue and the PPF were covered by the free nasal mucosa and the posterior maxillary wall mucosal flap, respectively. Iodoform gauze was used to hold all the grafts in place.
Postoperatively, all patients were confined to bed rest for the first 24 hours and received antibiotics for 7 to 10 days and 20% mannitol solution for 3 to 5 days. Patients were also instructed to avoid blowing their nose and strenuous physical activity for a month. The iodoform gauze was removed 7 to 10 days after surgery.
Efficacy Evaluation
Throughout the follow-up period, postoperative endoscopic surveillances were performed routinely. Complications (eg, hemorrhage, infection) and recurrence were recorded.
Results
This study consisted of 4 (33.3%) male and 8 (66.7%) female patients, with a mean age of 56.7 years (range: 45-69 years). Patients’ mean body mass index (BMI) was 28.81 kg/m2 (range: 19.5-38.4 kg/m2). By Chinese standards, 9 (75.0%) of 12 patients were overweight (BMI ≧ 24 kg/m2), and 7 (58.3%) patients were obese (BMI ≧ 28 kg/m2).
All patients presented CSF rhinorrhea, with a history of meningitis. All patients underwent the repair operation after the active meningitis was controlled. Cerebrospinal fluid rhinorrhea developed spontaneously in all patients. Two of 12 cases in this study were recurrent patients who each had undergone 2 repair operations through a transethmoidal sphenoid approach (Figure 4). And case 12 had previously undergone a resection of a meningioma in the right frontal lobe (Figure 2).
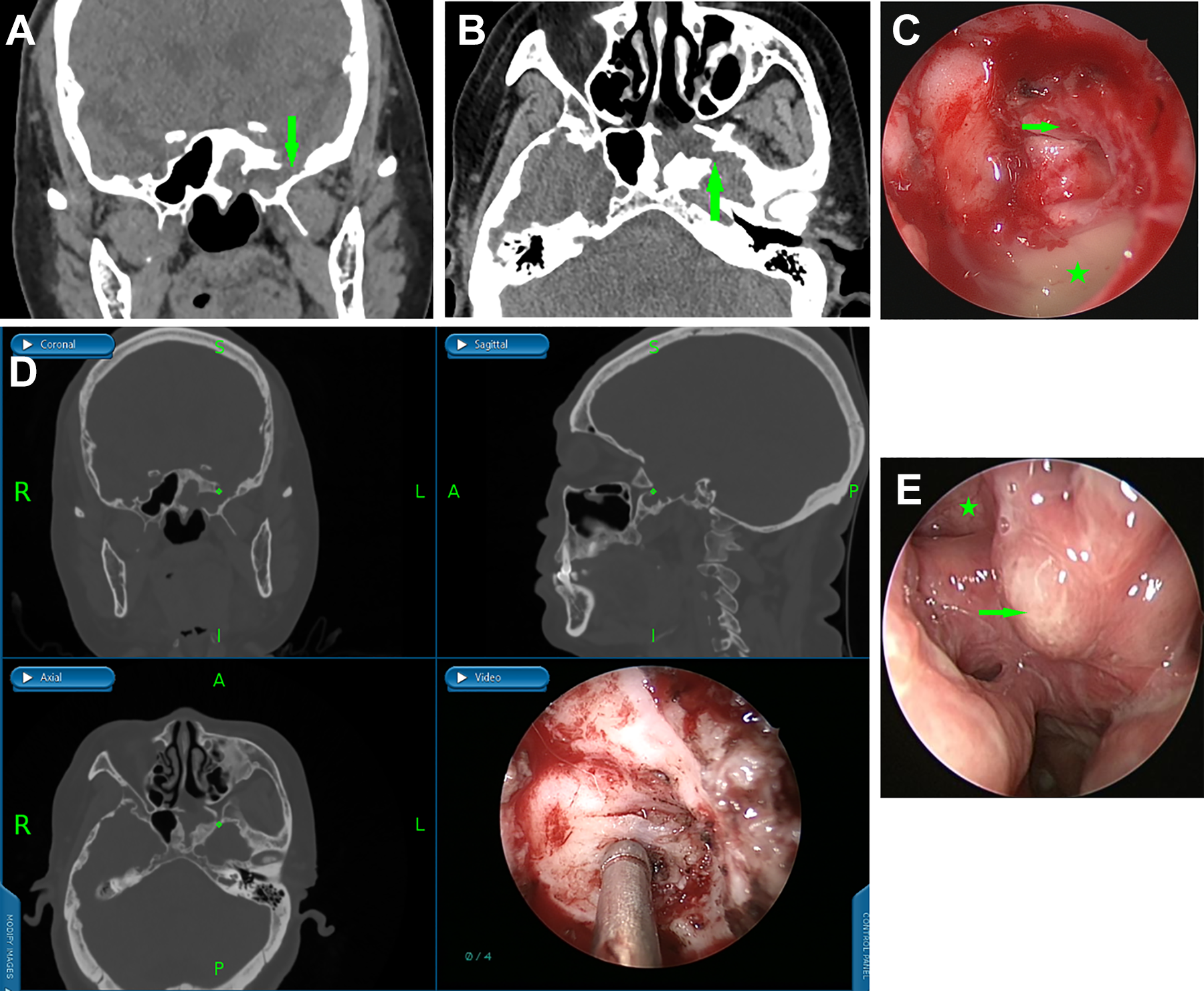
Clinical photographs of case 7 with recurrent cerebrospinal fluid (CSF) rhinorrhea in the sphenoid sinus lateral recess (SSLR) after transethmoidal–sphenoidal approach surgery. (A) Preoperative coronal computed tomography (CT) images showing a defect (arrow) in the left SSLR. (B) Axial CT images showing a defect (arrow) in left SSLR, anteroinferior wall of sphenoid sinus had been removed in a previous surgery. (C) Abscess (star) and swollen mucosa (arrow) in the left SSLR. (D) The defect was pointed out by navigation. (E) The sphenoid sinus (star) and obliterated SSLR (arrow) on the 6 months after surgery.
Each SSLR, left and right, had 6 cases of CSF rhinorrhea. The mean defect width was 3.75 mm (range: 3-6 mm). Six of 12 cases had a meningocele and 2 cases had a meningoencephalocele.
With the aid of image guidance, the defect in the skull base was pinpointed precisely. Through an EEPTA with obliteration of the lateral recess, CSF rhinorrhea was successfully repaired on the first attempt in all cases, with no intraoperative complications. In all patients, the repair area got complete epithelialization about 3 months after surgery (Figure 3F). No postoperative complications, such as meningitis or pneumocephalus, were observed in any case. All patients were followed up for a mean time of 40.3 months (range: 6-65 months) without recurrence. Table 1 presented patients’ demographic and surgical data.
Demographic and Surgical Data of Patients With CSF Rhinorrhea in SSLR.a
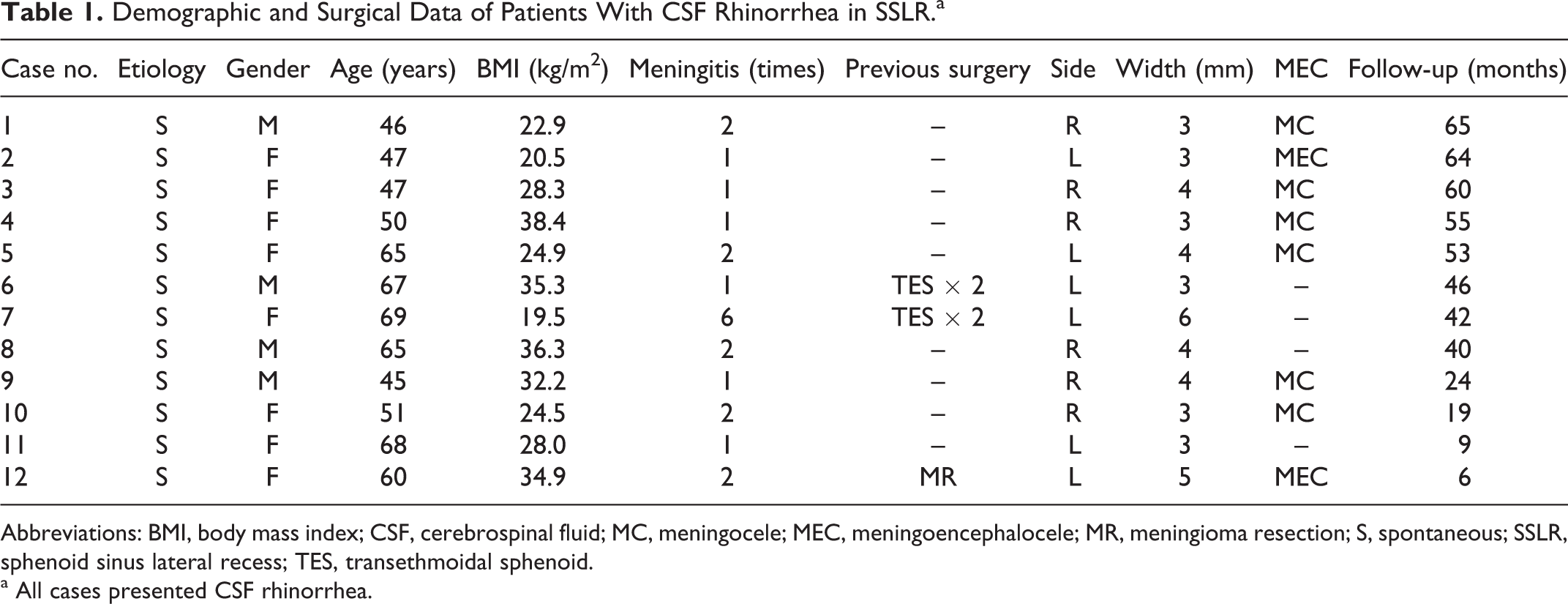
Abbreviations: BMI, body mass index; CSF, cerebrospinal fluid; MC, meningocele; MEC, meningoencephalocele; MR, meningioma resection; S, spontaneous; SSLR, sphenoid sinus lateral recess; TES, transethmoidal sphenoid.
a All cases presented CSF rhinorrhea.
Discussion
The EETPA can provide relatively wide access to dissect the SSLR under a 0° endoscope. Management of CSF rhinorrhea in the SSLR presents a major surgical challenge to a surgeon, due to the high rate of recurrence and difficult anatomy.9,10 The endoscopic endonasal approach to repair CSF rhinorrhea is increasingly replacing transcranial or extracranial techniques due to its advantages, including excellent visualization, minimal invasiveness, and limited morbidity. 6 Several endoscopic endonasal approaches have been described: the transseptal sphenoidotomy, the transethmoidal sphenoid approach and the transpterygoid approach.11-13 Transseptal sphenoidotomy did not provide an adequate visualization of the SSLR. The transethmoidal sphenoid approach permitted removal of the pterygoid process medial to the Vidian canal but was not wide enough to repair the CSF rhinorrhea in the SSLR. 14 Additionally, the endoscopic lateral transorbital approach and the contralateral precaruncular approach were described as shorter surgical pathways to the SSLR with no neurovascular structures in the trajectory.15,16 However, in addition to the absence of drainage and a postoperative endoscopic examination corridor, these surgical pathways may cause orbital injury or injury of the superior heads of the lateral pterygoid muscle, which may be avoided through a transpterygoid approach. 7 The EETPA has been the most common endoscopic endonasal access for the management of the SSLR since it was first described by Bolger in 1999.5,7 Pasquini et al 14 reported a successful outcome in 4 patients with CSF rhinorrhea in the SSLR repaired through an EETPA. Ulu et al 3 also reported their successful experience of repairing CSF leaks in the SSLR through EETPA in 13 patients, and the 100% success rate was obtained in spite of lacking treatment for reducing intracranial pressure (ICP). In this study series, there were 2 recurrent patients (case 6 and 7) who twice had undergone transethmoidal sphenoid approach operations in other hospitals. All 12 patients in this series underwent the EETPA to fully expose the SSLR and successfully complete skull base reconstruction. Through EETPA, most of the anterior wall of the sphenoid sinus, including the anterior wall of the SSLR, can be removed to fully expose the SSLR. Combined with a complete anterior and posterior ethmoidectomy and a wide maxillary antrostomy, a direct and relatively spacious corridor was gained to facilitate surgical manipulation in the SSLR and reconstruction of the defect in the skull base under the 0° nasal endoscope.
Meanwhile, the EETPA can also provide a wide and direct outflow pathway of sphenoid and maxillary sinuses to preserve the functions of paranasal sinuses and to do postoperative surveillance. Regular endoscopic examination and postoperative minimal debridement were needed after surgery. The wide antrostomy of the maxillary sinus and sphenoid sinus in this procedure ensured convenient endoscopic examination and debridement, which was helpful for epithelization of the repair area and recovery of functional mucociliary clearance. All these were essential for the long-term treatment of CSF rhinorrhea.
Multilayer reconstruction of skull base defects and obliteration of the SSLR with fat is a reliable method. Treatment of CSF rhinorrhea must achieve 2 primary goals: prevention of CSF leaks and permanent closure of the osteodural defect to diminish the risk of ascending infection.11,17,18 Complete obliteration of the sphenoid sinus to stop CSF rhinorrhea, regardless of the size and location of the defect, was reported previously. 19 However, obliterative technique alone can cure the CSF rhinorrhea but cannot eliminate the defects. 20 There are many other disadvantages of obliteration of a sphenoid sinus, such as a secondary mucocele, risk of vascular and nerve damage, and so on. It was easy to operate and reliable to obliterate the SSLR instead of the whole sphenoid sinus. The outflow pathway of the sphenoid sinus was reserved to facilitate postoperative examination, and the chance of infection and mucocele formation was greatly reduced. Despite the multiple options for skull base reconstruction, there is no consensus within the literature regarding the best treatment option. 21 In this study, multilayer reconstruction of skull base defects and obliteration of the SSLR with abdominal subcutaneous fat were adopted. All the patients were successfully treated on the first attempt, and the overall success rate was 100%. No postoperative complications and recurrence were observed during follow-up.
Intraoperative navigation is helpful for locating the important anatomic landmarks. 22 In the wide sphenoidotomy procedure, the optic nerve and internal carotid artery may be at risk of damage. During the transpterygoid procedure, the Vidian nerve, sphenopalatine ganglion, and the maxillary division (V2) of the trigeminal nerve were at risk of iatrogenic injury, which may result in reduction in tear secretion and facial numbness.15,23 Intraoperative navigation was used in various aspects of the procedure. It allowed us to pinpoint the important anatomical positions, and to successfully repair the defect in the skull base without damage to the important structures mentioned above, that is, without intraoperative complications.
Spontaneous CSF rhinorrhea may be associated with increased ICP.18,21 In this study, the patients were predominantly obese, middle aged and female, which in the literature are also reported to be the predominant factors for patients with spontaneous CSF rhinorrhea and increased ICP.21,24 Although the literature reports that postoperative ICP management, such as acetazolamide or CSF shunts, should be considered in patients with spontaneous CSF rhinorrhea, 21 several authors reported their excellent outcomes of repairing CSF rhinorrhea in the SSLR without postoperative ICP management.3,12,25 In the series, ICP monitoring was not performed, and the postoperative ICP management was not administered either. Despite this, our 100% success rate of primary repair presents a hypothesis that spontaneous CSF rhinorrhea in the SSLR can be treated with the surgery procedure through an EEPTA with obliteration of the lateral recess, without additional postoperative ICP management. In addition, the good outcome may also be partially attributed to the relatively lower average BMI (28.81 kg/m2) of the patients in our study, compared to that (>30 kg/m2) in western series,24,26 suggesting that the ICP of these patients may not be so high. However, a longer follow-up and a larger number of patients are still needed to prove the superiority of this procedure.
Conclusion
The EEPTA provides direct and relatively spacious access to the SSLR. Multilayer reconstruction of skull base defects and obliteration of the SSLR with abdominal subcutaneous fat is a reliable and easily implemented method. Image-guided navigation is helpful for locating the important anatomic landmarks to avoid intraoperative complications.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.