
Abstract

Intranasal corticosteroids are first-line treatment for allergic rhinitis (AR) and part of the treatment algorithm in patients with chronic rhinosinusitis (CRS), especially for medical management after endoscopic sinus surgery. Corticosteroids bind to the glucocorticoid receptor causing reduction in circulating T-lymphocytes, mast cells, eosinophils, and decrease IL-2, IL-4, and IL-5 production. 1 -3 The primary function of corticosteroids in patient with AR and CRS is to decrease inflammation within the lining of the sinonasal mucosa.
Intranasal steroids (INS) have advantages over conventional oral steroid therapy, especially for long-term medical management. Oral steroids are effective in improving sinonasal inflammation, but due to complications such as hyperglycemia, decreased bone density, avascular necrosis of the femoral head and peptic ulcers, they are discouraged for use as maintenance therapy. 4 Intranasal steroids have a minimal side effect profile; therefore, INS have become the part of the preferred maintenance therapy in patients with AR and CRS. There have been proven benefits in control of symptoms in both patients with AR and CRS as well as improved endoscopy scores, reduction of polyp size, and prevention of polyp recurrence in nasal polyp patients. 3,5,6
The first studies investigating the use of steroids locally involved the intranasal injection of corticosteroids in the 1950s. 1 This then evolved to the use of topical nasal formulations of corticosteroids, which have been available since 1970s, beclomethasone dipropionate being the first reported in the literature. 1 Since then, trends have included variation in the types of available corticosteroids, the over-the-counter sale of select intranasal corticosteroid sprays in 2013, 7 and updated delivery methods.
The most commonly used delivery system for INS are intranasal corticosteroid sprays, which are considered to be low volume, high pressure delivery systems. In the United States, there are currently 9 different corticosteroids approved for intranasal spray use (Table 1), with different commercial formulations. 3,8 These are generally well tolerated by patients, with the most common side effects being epistaxis, nasal irritation, and/or dryness. Such issues can usually be managed by reviewing proper application technique and/or altering the INS spray used, as the carrier solutions in the INS sprays can contribute to these side effects. Intranasal steroid sprays tend to be convenient with simple administration and fast application, leading to improved patient compliance. In 2006, a new delivery system was created (Xhance, Optinose US) in which a nasal steroid spray reservoir (fluticasone propionate) is connected to a mouthpiece used for patient breath actuation (exhalation) as the motive force for administration. This is associated with soft palate elevation and concentration of the steroid spray in the sinonasal cavity, with enhanced delivery to areas such as the middle and superior meatuses and sphenoethmoidal recess, which are not conventionally well treated with standard INS sprays. 2,6
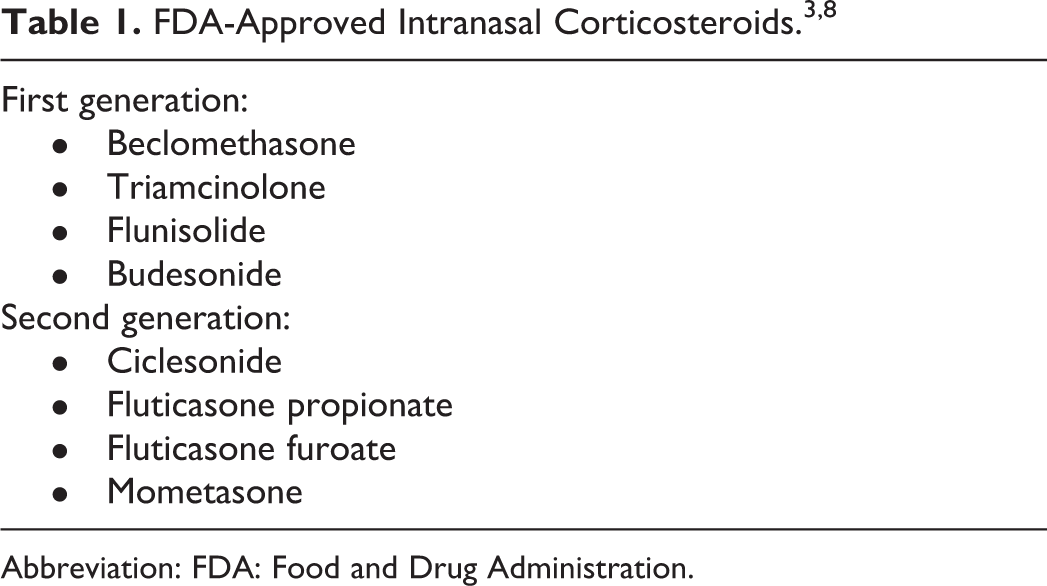
Abbreviation: FDA: Food and Drug Administration.
The approved use of INS sprays by the Food and Drug Administration (FDA) in the 1970s allowed for development of novel delivery methods of other steroid formulations, particularly the off-label use of corticosteroids in nasal saline rinses and as topical nasal drops. The use of INS drops is a low volume, low pressure delivery system with a higher concentration of corticosteroid compared to INS sprays. In this application technique drops, generally from a respule, are directly placed in the nasal cavity. The delivery of the medication can be altered by patient position during and after the drop placement, with popular positioning being the Mygind and Ragand positions. 6 Drops can also be placed in a mucosal atomization device to cause atomization of the particles to 30 to 100 ηm, allowing increased surface area for absorption. 4
Nasal steroid irrigations have also become increasingly common, particularly in postoperative patients with CRS. The addition of a respule or compounded corticosteroid to nasal saline irrigations allows for a high volume, high pressure delivery system which has been shown to allow for greater steroid penetration in the sinuses compared to INS sprays, especially postoperatively. 6 Additionally, steroid irrigations allow for a higher concentration of steroid to be delivered. For example, a budesonide repulse added to a standard saline rinse bottle allows delivery of up to 2 mg per 240 mL bottle, compared to budesonide spray which provides 64 to 400 µg per spray. 9 The increased steroid concentration and sinus penetration allows for improvement in patient symptoms as well as improved endoscopic scores in patients with CRS. 5
There has also more recently been development of steroid-impregnated packing techniques and steroid-eluting stents to allow for sustained topical delivery of corticosteroids over a period of time. For example, the addition of corticosteroid, such as triamcinolone, to bioabsorbable and dissolvable nasal packing material has been described. This has been shown to improve local inflammation and decrease postoperative synechiae formation. 10 Another form of targeted steroid delivery includes resorbable steroid-eluting stents such as Propel and Sinuva (Intersect ENT). Propel stents contain 370 µg of mometasone furoate in a polylactide-co-glycolide scaffold which slowly releases steroid locally over 30 days. These are typically placed intraoperatively so the effect is present in the postoperative setting. Sinuva stents contain the same material with 1350 µg of mometasone furoate that allows for drug elution over 90 days. Sinuva is approved for the use in recurrent nasal polyp patients. 10
There have been significant advancements in the formulations and delivery methods for INS in the last 50 years. The use of INS has been proven to have an integral role in the treatment of the AR and CRS, allowing for effective local control of sinonasal inflammation while consistently providing a minimal side effect profile. Future advancements and innovations can likely be expected to improve treatment for this complex patient population.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr Chandra is a member of the Clinical Trials Steering Committee for Optinose.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.