
Abstract
This report aimed to introduce a very rare presentation of congenital aural fistula and its treatment. A 13-year-old girl presented with a mass on the right temporal region with protrusion of the helix. She noticed a mass a month previously, and the mass gradually swelled with pain. Pus discharged from the pit behind the helix. Mastoiditis was suspected; however, the tympanic membrane was normal. Magnetic resonance imaging revealed a cystic mass in the temporal region. The surgical removal of the mass was performed using a postauricular incision. The mass was cystic and had a stem connected to the pit. Insertion of a probe into the pit showed a connection to the mass. The mass was totally removed with the skin around the pit. Histologically, the cyst connected to the fistula and its lumen was covered with squamous cells. A diagnosis of a congenital aural fistula developed posterior to the helix was made. Considering its location, the fistula had been formed between the third and fourth hillocks of the embryonal helix. Aural fistula developed posteriorly is very rare, and it mimicked a temporal tumor or mastoiditis with a protruding auricle. Careful observation of the skin and consideration from developmental aspects are needed for an accurate diagnosis.
Introduction
Congenital aural fistula is commonly encountered in Ear, Nose, and Throat (ENT) clinics. Fistula contains wet dirt and sometimes occurs due to bacterial infection. Usually, it develops on the face anterior to the ascending limb of the helix, followed by the inferior portion of the ascending limb itself. Because it is a remnant of the embryonic fusion of the 6 embryonic hillocks that develop from the first and second branchial arches, it may be found anywhere around the external ear. However, it usually develops on the face anterior to the ascending limb of the helix, followed by the inferior portion of the ascending limb itself. Aural fistulas that develop in other portions are very rare. Especially, a case developed superior to the helix has never been reported. This report introduces an aural fistula that developed behind the helix and presented a temporal mass.
Case Report
A 13-year-old girl was referred to our department, presenting a large mass on the right temporal region. She noticed a temporal mass a month previously. No other symptoms, such as pain, were shown; however, the mass suddenly swelled with pain, so she visited another ENT clinic. The right temporal region was swollen. Small fistulas were detected above the right ear, and purulent discharge leaked from the fistula. The administration of antibiotics was started; nevertheless, symptoms did not cease. She underwent a puncture; however, no liquid content was suctioned. For further treatment, she was referred to our department.
At presentation, the right temporal area was swollen with skin rubor. The auricle was protruded, and purulent discharge was observed from the small pit behind the helix. Mastoiditis was suspected at first; however, the tympanic membrane was normal, and the hearing test proved normal hearing. Magnetic resonance imaging revealed a cystic and well-encapsulated mass in the temporal area (Figure 1A). The mass was located between the skin and temporal muscle and measured 50 mm on the longest diameter. The mass showed a heterogeneous signal and might contain liquid contents inside. The surgical removal of the mass was planned.

T2-weighted coronal MR image (A). Skin incision was designed posterosuperiorly to the helix (B). The mass (*) was removed with a pit (arrow) and the surrounding skin (C). MR indicates magnetic resonance.
Under general anesthesia, temporal to postauricular skin was incised, and the skin flap was elevated, leaving it around the fistula (Figure 1B). The probe inserted from the fistula revealed a connection to the inside of the mass. The mass was carefully separated from the adjacent soft tissue; then, the mass was totally removed with the fistula and adjacent skin (Figures 1C and 2A). The mass contained sticky purulent retention. Histologically, the cyst communicated with the fistula and was surrounded by cartilages and sebaceous glands. Its lumen was covered with squamous cells, and granulation tissue with inflammatory change was observed inside (Figure 2B and C). A diagnosis of a congenital aural fistula was made. Considering its location, the aural fistula developed between the third and fourth hillocks during aural development. The postoperative course was uneventful. She was free of the disorder 3 months after surgery.
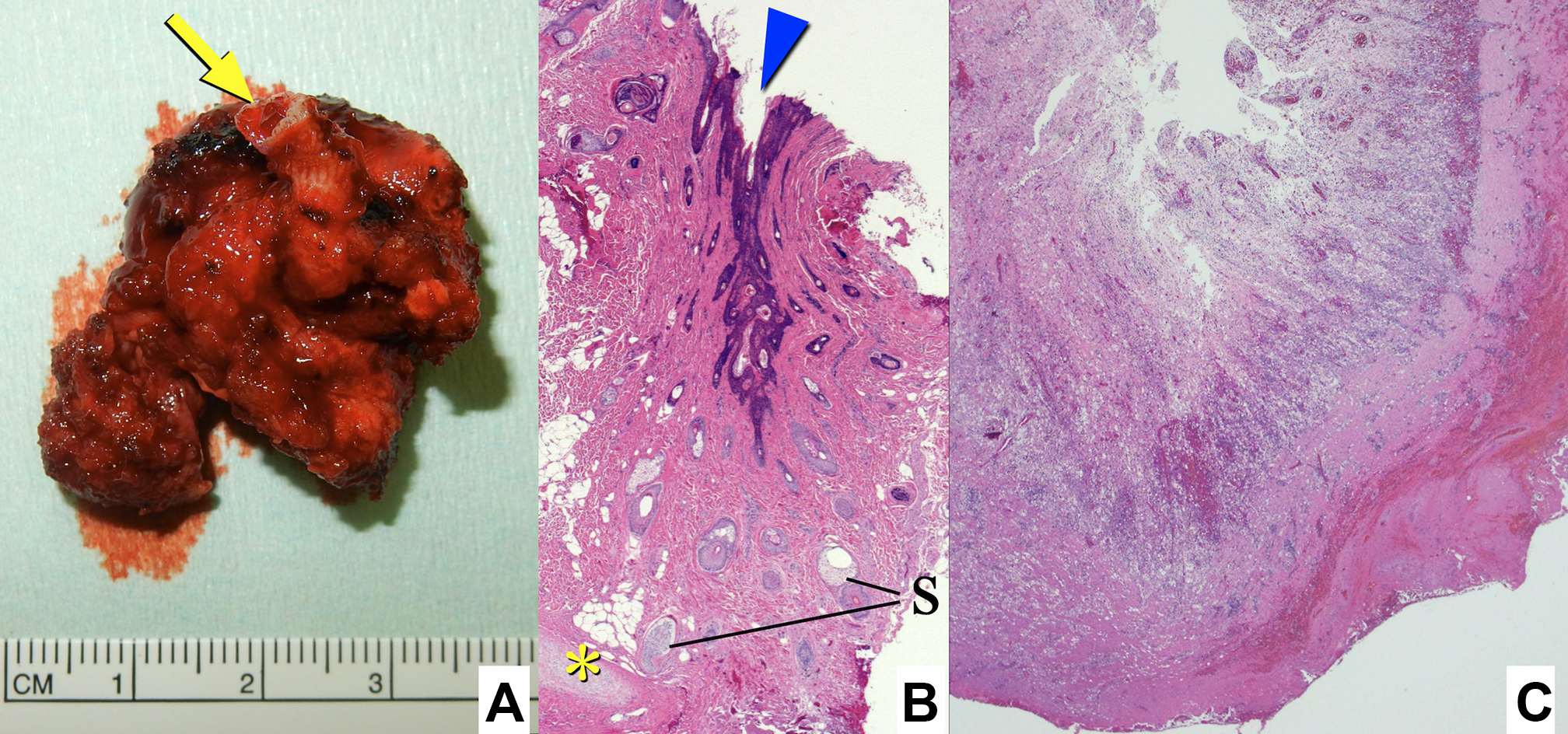
Cystic mass with tract and pit (A; arrow, pit). Histopathology of the tract (B; arrowhead, pit and tract; *, cartilages; S, sebaceous glands). The cyst contains granulation with inflammatory cell infiltration (C).
Conclusion
Congenital aural fistula is a commonly encountered disorder in ENT clinics. During embryogenesis, the auricle arises from the first and second branchial arches and develops 3 hillocks each. 1 These 6 hillocks adhere to each other and form a helix later. Various theories have been proposed on the embryological development of the human auricle; however, the aural fistula is thought to occur as a result of the incomplete fusion of these hillocks.2,3
In most cases, the fissures are located near the front of the helix and therefore described as preauricular sinuses, cysts, pits, or fissures. 4 However, various patterns are reported as they might be formed between 6 hillocks.5-8 The fistula has an entrance to the sinus tract that goes under the skin around or in the helix. The sinus tract is lined with squamous epithelium and may accumulate dirt and then produce epithelium-lined subcutaneous cysts and sometimes become infected, leading to cellulitis or abscess.
Shokan reported various types of aural fistulas. 5 Based on the location and developmental anatomy, aural fistulas are classified into 8 types: marginal helicine, preauricular, crural, infratragal, central lobular, postauricular, helicolobular, and posthelicine. Fistulas showing superoposterior developments are helicolobular and posthelicine. Congdon stated that a posthelicine fistula develops between hillocks 4 and 5, and a helicolobular fistula develops between hillocks 5 and 6. 2 Choi et al classified this pathology as classic and variant. 6 They also classified the variant type into 3 different types. However, the present case did not match their classification. According to the location of the fistula, the authors believed that the fistula was formed between the third and fourth hillocks of the embryonal helix.9-11
Choi et al noted that the preauricular sinus can occur in the postauricular area. 6 They named such cases as the variant type of auricular sinuses. Most fistular tracts of the variant type were directed in the posterior–middle direction from the pits. In the present case, the cyst was situated in the posterior direction, superior to the helix, and mimicked abscess from mastoiditis. No lesions were detected in the middle ear and small pit situated just behind the helix. The fistula tract was directed in the posterosuperior direction. Therefore, this case was assumed to be a rare variant of the aural fistula.
In this report, we diagnosed this pathology as the aural fistula developed between 3 and 4 hillocks; however, this might be a type of the first branchial cleft fistula because the first branchial cleft fistula contributes to the external ear canal and the first pharyngeal pouch contributes to the development of the Eustachian tube, tympanic cavity, and mastoid air cells. The first branchial cleft fistula develops around the ear canal and has an intimate relationship to the facial nerve. 12 Like the present case, the first branchial cleft fistula also occurs near the helix.12,13 However, the cyst and the fistula did not present near the external ear canal but above and far-off the canal. In addition, the first branchial cleft fistula usually occurs in the infero-anterior aspect of the helix, such as the external ear canal and parotid gland. 13 Therefore, we thought that this fistula developed between the third and fourth hillocks during the development of the helix. If this case was originally developed from the first branchial cleft fistula, it was also a very rare presentation.
The complete surgical excision of a congenital aural fistula is necessary for avoiding recurrent or persistent infection. 6 A temporal skin incision was applied in the present case. Under sufficient surgical view, the cystic lesion was completely removed with tracts and pit on the skin. This case has never been reported previously; therefore, the surgery was also exceptional. Anatomical recognition and careful observation of skin lesions are essential for the treatment of atypical congenital fistulas.
Footnotes
Authors’ Note
Written informed consent was obtained from the patient who participated in this study. SK and AT contributed to conception, design, data collection and/or processing, writing manuscript and literature review; TA and FM contributed to supervision. AT, AY, TM contributed to analysis and/or interpretation; AY, TM, TA, FM contributed to critical review.
Acknowledgments
The authors acknowledge Dr Hotchi, MD, at Department of pathology for thorough pathological assessments.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.