
Abstract

A 29-year-old lady presented with history of left ear block sensation and gradually progressing hearing loss for the past 2 years. She also complained of left-sided throat pain, radiating to the left side of the face and the left ear. The pain was spontaneous in onset and had no relation to chewing or swallowing. She had no breathing or swallowing difficulty, no voice change or speech difficulty, and no nasal complaints.
On examination, the left tympanic membrane was dull and she had a mild conductive hearing loss with a B type curve on tympanometry. There was a 2 × 3 cm smooth, mucosa covered, pedunculated mass arising from the left lateral wall of the oropharynx. The left side of the soft palate was hypoplastic, the left tonsillar pillar was absent and the left tonsil was located posterior to the tongue (Figure 1). A contrast-enhanced computed tomography (CT) scan of the neck showed a 1.8 × 1.6 cm partially calcified lesion with well-defined margins and areas of intralesional fat, probably developing marrow, seen in the nasopharynx (Figure 2A).
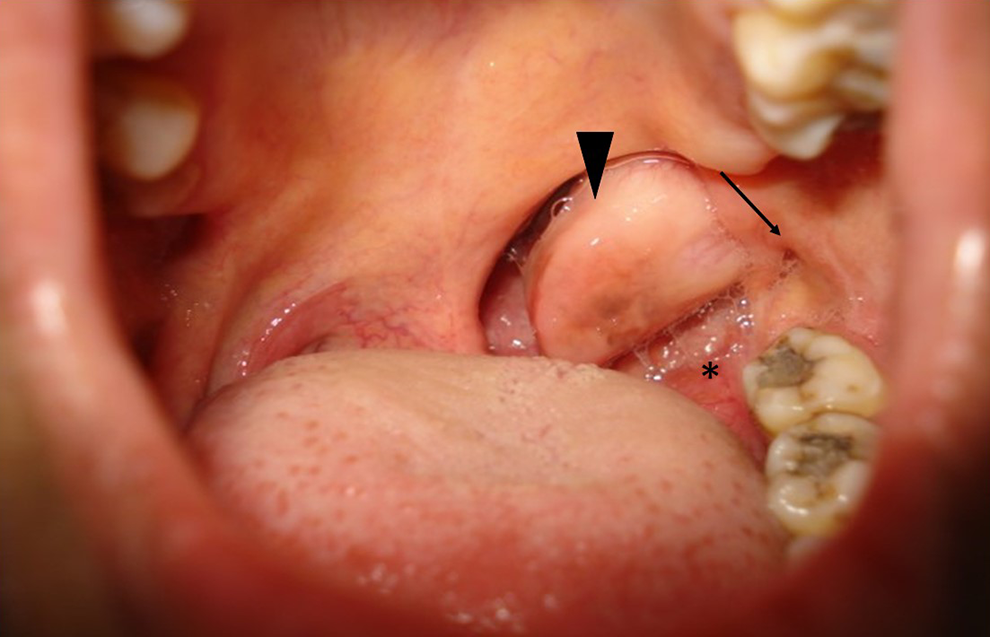
Preoperative picture of the sausage-shaped mass occupying the left side of the pharynx (black arrowhead points to the hairy polyp, black arrow points to the Eustachian tube orifice behind the last molar, the asterisk is on the displaced tonsil).
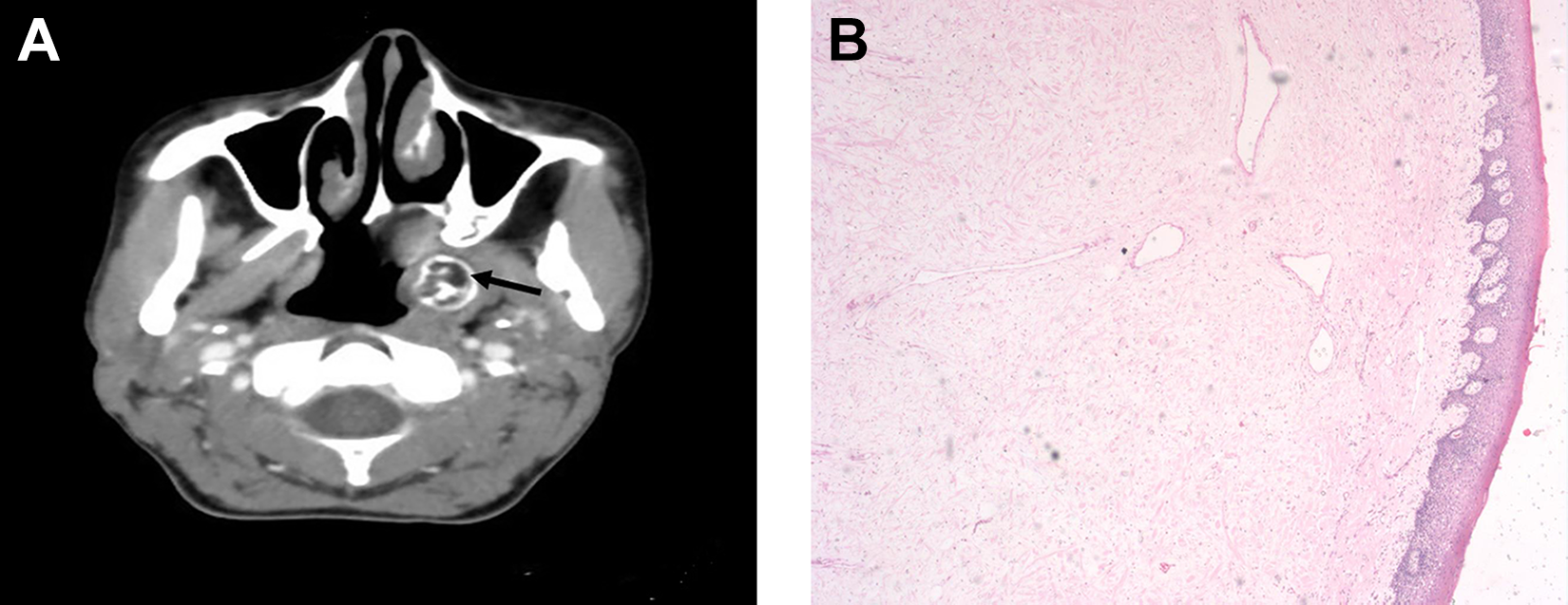
A, Contrast-enhanced computed tomography head and neck scan axial image showing the partially calcified mass arising in the nasopharynx (black arrow). B, Photomicrograph showing stratified squamous epithelium, vascular fibro adipose tissue, and bone trabeculae (hematoxylin and eosin 25×).
She was taken up for examination of the pharynx under general anesthesia and excision of the mass. A left myringotomy was done, which yielded no fluid from the ear. A hard, smooth surfaced mass was seen arising from just behind the Eustachian tube orifice which was seen lower than usual, behind the last upper left molar. The left half of the soft palate was hypoplastic and the left tonsil was located posterior to the tongue base. The tumor was excised in toto via a transoral approach after endoscopic assisted visualization and cauterization of the base.
Sectioning revealed a cavity filled with spongy bone, with an overlying cartilaginous surface. Microscopically, there was fibrocollagenous tissue covered by acanthotic stratified squamous epithelium which contained a lesion composed of mature bone trabeculae with intervening vascular fibro adipose tissue (Figure 2B). Postoperatively, the patient had relief from her symptoms of throat pain and ear block sensation. The Eustachian tube opening was normal. She did not have any aspiration or difficulty in speech, although her voice was hyper nasal in quality.
Dermoids are composed of mature tissue from the ectoderm and mesoderm and lack endoderm. They are also known as “Hairy polyps of the nasopharynx” because of the macroscopically visible fine hairs arising from the external covering of the skin and first reported by Brown-Kelly.1,2 Microscopically, in addition to skin and its appendages, the lesion may contain fat lobules, fibrovascular connective tissue, muscle, minor salivary glands, nerves, lymph nodes, cartilage, and bone. 3
Hairy polyps are usually single, pedunculated masses and are often confused with dermoid cysts which are composed of ectoderm with epidermal adenexae. 4 They may interfere with the palatal shelves and cause an associated cleft palate. Associated absence of the uvula, external auricles, ankyloglossia, and facial hemihypotrophy have been reported, all giving substance to the theory that they are malformative lesions originating from the first or second branchial arch or sequestrated first pharyngeal pouch.3,5,6
They are commonly diagnosed at birth or soon after. In about 20% to 30% of cases, they may be diagnosed prenatally, as a cause for polyhydramnios. 7 Approximately 60% of the lesions originate in the nasopharynx, and the others originate in the tonsillar region or the oropharynx. There is a female preponderance of 6-7:1. The symptoms depend on the age of presentation, size, and location of the lesion. The infant may present with dyspnea, cyanosis, difficulty in sucking, and swallowing. In partial obstruction of the nasopharynx, there may be excessive snoring, snuffling, and persistent mucoid discharge from the nose. The dermoids escaping early detection due to their small size and inconspicuous location may be detected accidently on routine examination at an older age for some unrelated disease. 3 Various similar polypoidal lesions of the oropharynx have been described; hamartomas, true teratomas, teratoid, dermoid, or epignathus. Lesions found in adults are rare; they are likely to be hamartomas or may be explained as delayed pluripotent cell morphogenesis or neoplasms.7,8
Irrespective of the age of presentation, dermoids are strictly benign lesions with limited growth potential. Management of hairy polyps traditionally involves airway management, physical examination, evaluation of the complete extent of the lesion by CT or magnetic resonance imaging, and surgical excision. As sonography improves, there is scope for improved prenatal diagnosis. Transoral endoscopic-assisted removal of the nasopharyngeal dermoid is associated with decreased morbidity from facial or Eustachian tube scarring, better excision and shorter operating time. 9
Footnotes
Authors’ Note
Suma Susan Mathews takes responsibility for the integrity of the content of the paper.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.