
Abstract
Alveolar soft part sarcoma (ASPS) is an aggressive soft-tissue malignancy, notorious for its metastasis to other tissues. A considerable number of cases in the head and neck have been reported but not in the hypopharynx. We describe a 31-year-old man with an incidental finding of a hypopharyngeal mass. Flexible laryngoscopy revealed a fleshy mass 2 × 2 cm2 originating from the left hypopharynx and overlying the epiglottis. Computed tomography scan demonstrated a soft tissue mass in the left wall of the oropharynx measuring about 2.2 × 1.8 cm2, projecting into the hypopharyngeal air space. Magnetic resonance imaging showed a significant thickening of the left hypopharyngeal wall forming a mass lesion occupying the left pyriform sinus and abutting the left aryepiglottic fold. Histopathology indicated that tumor cells were polygonal and epithelioid, with abundant eosinophilic to clear flocculent cytoplasm, eccentric nuclei, and prominent nucleoli. The tumor was positive for smooth muscle actin with rare cells staining for Human Melanoma Black (HMB45). Fluorescence in situ hybridization for transcription factor E3 was also performed and supported the above diagnosis. Our study reports the first case of ASPS in the hypopharynx.
Background
Alveolar soft part sarcoma (ASPS) is a severe and rapidly growing soft tissue tumor that infrequently occurs in the head and neck. It appears insidiously as a soft tissue tumor that grows slowly, mainly occurs among children and young adults, and is notorious for its metastasis to other tissues. 1 The prevalence of soft tissue sarcomas is 1% of all types of cancers. 2 The ASPS comprises 0.2% to 1% of all soft tissue sarcomas.
Despite being a rare type of sarcoma that mainly occurs in the limbs, a number of cases in the head and neck region have been previously reported; about 25% of ASPS cases occur in the head and neck.2,3 Patients with ASPS in the head and neck region present with symptoms ranging from difficulty in swallowing, hoarseness of voice, or bleeding. The tumor is less aggressive than those in other locations. 4
Alveolar soft part sarcoma has been documented in the literature to occur in the larynx,5-7 false vocal cord, 8 parotid gland, 8 sinonasal region, 9 tongue,2,10-22 oral cavity, 23 mandible, 3 parapharyngeal space, 24 nasal tissue, 25 cheek,26,27 buccal space, 2 gingiva, 28 paravertebral space, 2 and pharynx 28 but not the hypopharynx. To the best of our knowledge, this is the first case of hypopharyngeal ASPS reported in English literature.
Case Report
History
A 31-year-old Indian man was referred from the pulmonary unit for an incidental finding of hypopharyngeal mass. The patient had first presented in August 2019, with a complaint of hemoptysis. He denied any history of fever, weight loss, dysphagia, or any other symptoms.
On further inquiry, he had been working as an unskilled labor for 3 years in United Arab Emirates. He was a social alcohol drinker, nonsmoker, and not taking any medication for chronic disease. His family history was negative for any similar illness or other sarcomas.
The patient was investigated at the pulmonary unit for his initial complaint of hemoptysis. Incidentally, a mass in the left hypopharynx was noticed using flexible bronchoscopy. Bronchoscopy itself was negative.
The patient was then referred to the ENT department for follow-up. At the ENT department, the patient underwent diagnostic flexible laryngoscopy. The flexible laryngoscopy showed a fleshy mass 2 × 2 cm2 arising from the left hypopharynx and lying over the epiglottis, but the glottis and vocal cords were both free with bleeding points toward the medial part. Direct rigid laryngoscopy and biopsy was performed under general anesthesia. His chest X-ray, complete blood count, and the international normalized ratio were all normal.
Investigations
In addition to the above, blood tests, renal profile, and liver function tests were within normal range.
Computed Tomography Scan
Computed tomography (CT) scan demonstrated a soft tissue mass in the left wall of the hypopharynx that measured about 2.2 × 1.8 cm2 projecting into the hypopharyngeal air space. It touched the epiglottis and showed heterogeneous, mainly peripheral, enhancement with central necrosis, suggestive of a malignant process. No pathologically enlarged lymph nodes were seen. Computed tomography scan of the thorax and abdomen were normal.
Magnetic Resonance Imaging
Magnetic resonance imaging (MRI) showed a significant wall thickening of the left hypopharyngeal wall (the site of the previously described mass lesion in the CT scan), forming a mass lesion occupying the left pyriform sinus and abutting the left aryepiglottic fold (Figure 1). It measured about 1.4 × 1.1 mm, exerting high T2 and low T1 signal intensity with post-contrast enhancement. Normal appearance of the scanned neck structures, including neck musculature, carotid sheath, nasopharynx, and larynx vocal cords, was observed. No significant pathological lymphadenopathy was noted.

MRI with contrast showed the small mass T2 high signals. MRI indicates magnetic resonance imaging.
Histopathology
Grossly, the biopsy revealed a fleshy mass with a bleeding point from the left hypopharynx. The hypopharyngeal biopsies showed subepithelial hemorrhagic neoplasm arranged in sheets and cords. Tumor cells were polygonal and epithelioid appearance with abundant eosinophilic to clear flocculent cytoplasm, eccentric nuclei, and prominent nucleoli. The surface epithelium appeared uninvolved. Mitoses were not readily identified (Figure 2).
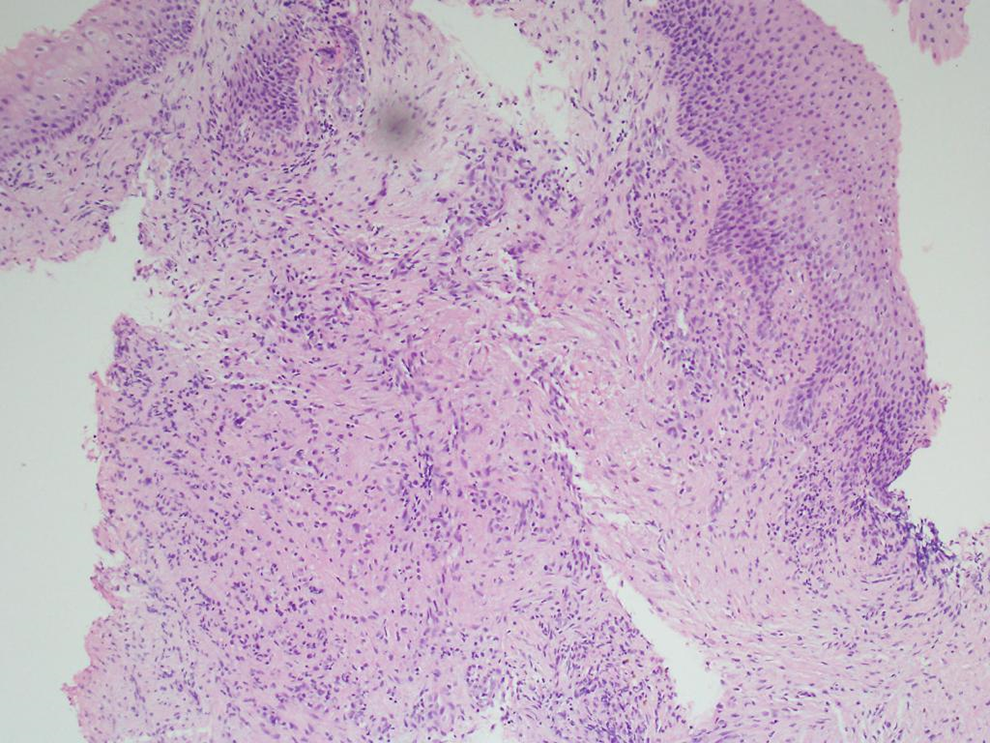
Histophotomicrographic appearance of the tissue showing squamous mucosa with submucosal tumor cell infiltrate.
Immunohistochemical Stain
Immunohistochemical staining for smooth muscle actin (SMA; myogenic), Cytokeratin OSCAR (epithelial origin), HMB45 (malignant melanoma), anaplastic lymphoma kinase ALK (lymphoma), and desmin (myogenic tissue) were performed. The tumor was positive for SMA with rare cells staining for HMB45 and negative for Cytokeratin OSCAR, ALK, and desmin. These findings were suggestive of ASPS.
Cytogenetics
Fluorescence in situ hybridization (FISH) for transcription factor E3 (TFE3) was also performed and supported the above diagnosis. The result is abnormal and indicates a rearrangement involving the TFE3 gene region in 78% of nuclei.
Discussion
Alveolar soft part sarcoma is a tumor of young age-group with a predilection to trunk and extremities. It tends to occur in the head and neck region in children. The double female to male ratio is reversed after the third decade of age.29,30
Alveolar soft part sarcoma is known for its poor prognosis among adults owing to its high metastatic potential. When this tumor is diagnosed in the upper or lower limbs, metastases occur at about 20% to 40% of cases at the time of diagnosis. Diagnosis of ASPA in the head and neck area is usually associated with better prognosis as the tumor does not reach the advanced stage by the time of diagnosis. This is thought to be due to the anatomy of the head and neck that hamper the growth of these sarcomas. Early diagnosis and treatment are crucial for such a rare malignancy.28,31,32
The involvement of pharynx with ASPS is uncommon compared to other organs (tissues) at the head and neck. In the larynx, cases occur in the false vocal cord5,8 and true vocal cord. 2
A case of large ASPS occupying the hemilarynx was also reported in a 23-year-old male. 6 Similarly, a large mass occupying the left part of the supraglottic compartment reported in a 33-year-old female. The mass was extending from the inferior border of the epiglottis to the left vocal cord. 7 The cardinal presenting feature of ASPS involving larynx was hoarseness of the voice. A prestyloid parapharyngeal space ASPS was reported with an initial complaint of painful mass and increasing dysphagia. 24 Wang et al 28 reported 18 cases of ASPS, among which one is occurring in the pharynx without a further account on presenting symptoms. This current case is unusual in that the patient did not report any symptoms related to the pharynx like cough, dysphagia, mass, or hoarseness of voice.
The differential diagnosis of ASPS comprises various benign and malignant soft tissue tumors, such as rhabdomyoma, hibernoma, clear cell sarcoma of soft tissue, perivascular epithelioid cell tumor (PEComa), paraganglioma, and granular cell tumor. Secondary malignant deposits of tumors with similar cytological characteristics may resemble ASPS. This is seen in clear cell renal cell carcinoma, hepatocellular carcinoma, adrenocortical carcinoma, and non-melanotic melanoma.
It is relevant to indicate that PEComa may resemble ASPS as it might include cytoplasmic eosinophilic granules positive for periodic acid–Schiff stain, and it stains positive for Transcription Factor Binding to Immunoglobulin Heavy Constant Mu (IGHM Enhancer 3; TFE3). The pathological findings of a positive result for SMA and FISH for TFE3 were among the supporting evidence of ASPS diagnosis.
The radiological findings of our case support a malignant process. Due to the vascular composition of ASPS, it is contrast-enhancing. 33 This hypopharyngeal ASPS demonstrated a high density during the relaxation time of the MRI sequencing pulse. 29 Surgery remains as the main treatment modality. The extent of tumor resection determines the future outcome, the possibility of recurrence, and patient survival. On this basis, radiological modalities, mainly CT and MRI, remain crucial to aid surgical resection of the tumor.
Surgical removal of the tumor was planned to be followed by radiotherapy. However, the patient opted to receive treatment at his country of origin (India), and he was lost to follow up. In conclusion, our study reports a case of head and neck ASPS in an extremely rare location, the left hypopharynx. When arising in a rare location, diagnosis can be difficult, and analysis of the histopathologic, immunohistochemical, and molecular genetic features is beneficial for confirmation.
Footnotes
Acknowledgment
Authors would like to thank Omar Emad Ibrahim from department of pathology, faculty of dentistry, Universiti Teknologi MARA for critically reviewing the manuscript and confirming the diagnosis. Authors also thank Associate Professor Dr Halyna Lugova from community medicine unit, National defence university of Malaysia for proof-reading and editing the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.