
Abstract
Introduction:
Resection of carotid body tumor (CBT) in patients of advanced ages has not been appreciated.
Objectives:
This study aims to assess the clinical characteristics and perioperative comorbidities for CBT resection in patients of advanced age and to validate the application of an “isolated island” technique for extirpation of CBT.
Methods:
Eight patients of advanced age (≥60 years) who underwent CBT resection were enrolled as the study group (SG). Another 29 patients of younger age (<45 years old) underwent CBT extirpation were assigned as the control group (CG). The perioperative issues were compared between these 2 groups.
Results:
The “isolated island” technique was successfully applied for resection of CBT in all 37 patients. The prevalence of Shamblin classification I, II, and III tumors in the SG was 12.5%, 62.5%, and 25%; whereas in the CG was 10.3%, 55.2%, and 34.5%, respectively. Bilateral CBT was observed in 7 patients of the CG and none in the SG. Vascular reconstruction was required for 1 (12.5%) patient in the SG, while it was required for 8 (27.6%) patients in the CG. Postoperative vocal cord palsy occurred in 37.5% of patients in SG, whereas the vocal cord palsy (34.5%) and dysphagia (6.9%) were commonly encountered in CG. In addition to postoperative length of stay (P = .004), no significant difference for operative time, intraoperative blood loss, or mortality were observed between these 2 groups (P > .05).
Conclusion:
Extirpation of CBT in patients of advanced age is rationale in appropriately selected patients. The “isolated island” technique is safe for CBT resection with seemingly low complication rates.
Introduction
Head and neck paragangliomas are uncommon tumors which mainly include carotid body tumor (CBT), vagal paraganglioma, and glomus jugular tumors.1,2 These may be located in a variety of locations including some rarely reported sites (eg, sinonasal cavity, larynx, and thyroid gland). 3 Given the complex neurovascular anatomic relationships associated with head and neck (or cervical) paragangliomas, surgical extirpation remains challenging, especially for those tumors intimately adherent to the great vessels or lower cranial nerves.4,5
The CBT is the most common type of paraganglioma observed in the head and neck region. 3 Its diagnosis, technical nuances, postoperative comorbidities, and long-term follow-up have been detailed by previous reports.6,7 Surgical extirpation remains a preferred method for treatment of many CBTs. 8 For younger patients, total surgical extirpation has achieved satisfactory outcomes and the safety of the procedures is well described, although injury to the lower cranial nerves is devastating. 9 However, for patients with advanced age (≥60 years), the potential for perioperative complications and morbidities is generally thought to be increased. Given this, careful observation or radiotherapy may become the appropriate strategy more commonly used in patients of advanced age.9,10
For those patients whose tumor closely adheres or envelops the common or internal carotid artery (ICA), the strategy to separate and preserve the ICA is of critical importance during management of these tumors. Various recommendations have been discussed and implemented to avoid catastrophic comorbidities (eg, ICA rupture) and enhance the safety of these procedures. These include strategies such as preoperative stenting of the ICA, intraoperative vascular reconstruction, or ICA sacrifice when warranted.8,11 Consequently, the overall occurrence of postoperative complications that are associated with ICA injury or occlusion were acceptable. 12 To the best of the authors’ knowledge, however, literatures regarding the treatment efficacy and management of the ICA in patients with CBT with an emphasis on patients of advanced age are sparse. The perioperative neurovascular complications in patients of advanced age are a major concern; but so are other indices including combined systemic disease, and increased fragility of the great vessels. This may discourage attempts at surgical extirpation of CBT for patients of advanced ages. 13
In this retrospective case series, we summarized our 16-year experience of patients with resection of CBT in a single tertiary center. The goal of this study was to assess the clinical characteristics and perioperative complications for CBT resection with an emphasis in patients of advanced age and to validate the application of the “isolated island” technique for extirpation of CBT in this patient cohort.
Materials and Methods
Clinical Data
Seventy-nine patients with head and neck paragangliomas were retrospectively analyzed from January 1, 2003, to December 31, 2018, at Beijing Tongren Hospital, Capital Medical University in China. Sixty-four of these patients accepted surgical extirpation as the treatment strategy, and the remaining 15 patients selected observation or radiotherapy. Of these, 15 patients preferring nonsurgical treatment, 3 patients harbored heart failure, 1 patient had a history of stroke, and the remaining 11 patients did not demonstrate coexisting comorbidities. Among those 64 patients who underwent surgical extirpation, 52 patients were eventually diagnosed with CBT; whereas 12 patients who had paragangliomas arising from the jugular foramen region (n = 8) or the vagal nerve (n = 4) were excluded from the current study. Among these 52 patients with CBT, 8 patients of advanced age (60 years old or older) were enrolled as study group (SG). To compare treatment efficacy and morbidity between an advanced (≥60 years old) and a younger age surgical patient group, 29 patients younger than 45 years old were assigned as the control group (CG). Those patients with the ages ranging from 46 to 60 years old (n = 15) were excluded from this study. Informed consent was obtained from these patients upon admission, and the study protocol was approved by the Ethics Committee of Beijing Tongren Hospital, Capital Medical University, China.
Preoperative contrast-enhanced computed tomography and gadolinium contrast magnetic resonance imaging scans were performed to evaluate the relationship of the tumor body with the adjacent great vessels. Preoperative digital subtraction angiography (DSA) examination was also routinely performed for each patient with CBT who underwent surgical extirpation to assess the blood supply of the tumor body, opening of the anterior and posterior vascular communications, the reflux systolic pressure, and to be able to complete any necessary embolization.
In addition to demographic characteristics, indices including preoperative symptoms, unilateral or bilateral occurrence, clinical Shamblin classification, dominant nurturing vessels, maximum tumor size, intraoperative blood loss, operative time, necessity of vascular reconstruction, postoperative length of stay, postoperative comorbidity and mortality, and recurrence were compared between the SG and the CG.
“Isolated island” technique
All 37 patients underwent an “isolated island” technique for resection of CBTs. This technique is not new, and a similar technique has been previously described.14,15 There were 4 critical steps involved to facilitate the application of “isolated island” technique as listed below: Separation and preservation of the lower cranial nerves, including the highest priority of vagal, hypoglossal, and accessory nerves, in addition to others such as sympathetic nerve fibers, ansa hypoglossal, and superior laryngeal nerves (Figure 1A). Exposure of the superior and inferior borders of the tumor, which subsequently form into the “isolated island” (Figure 1B). Dissection of the tumor commences from the weakest point, which typically lies between the dorsal aspect of ICA and the vagal nerve (Figure 1C). A subadventitial dissection and careful separation was subsequently performed to facilitate complete extirpation (Figure 1D).
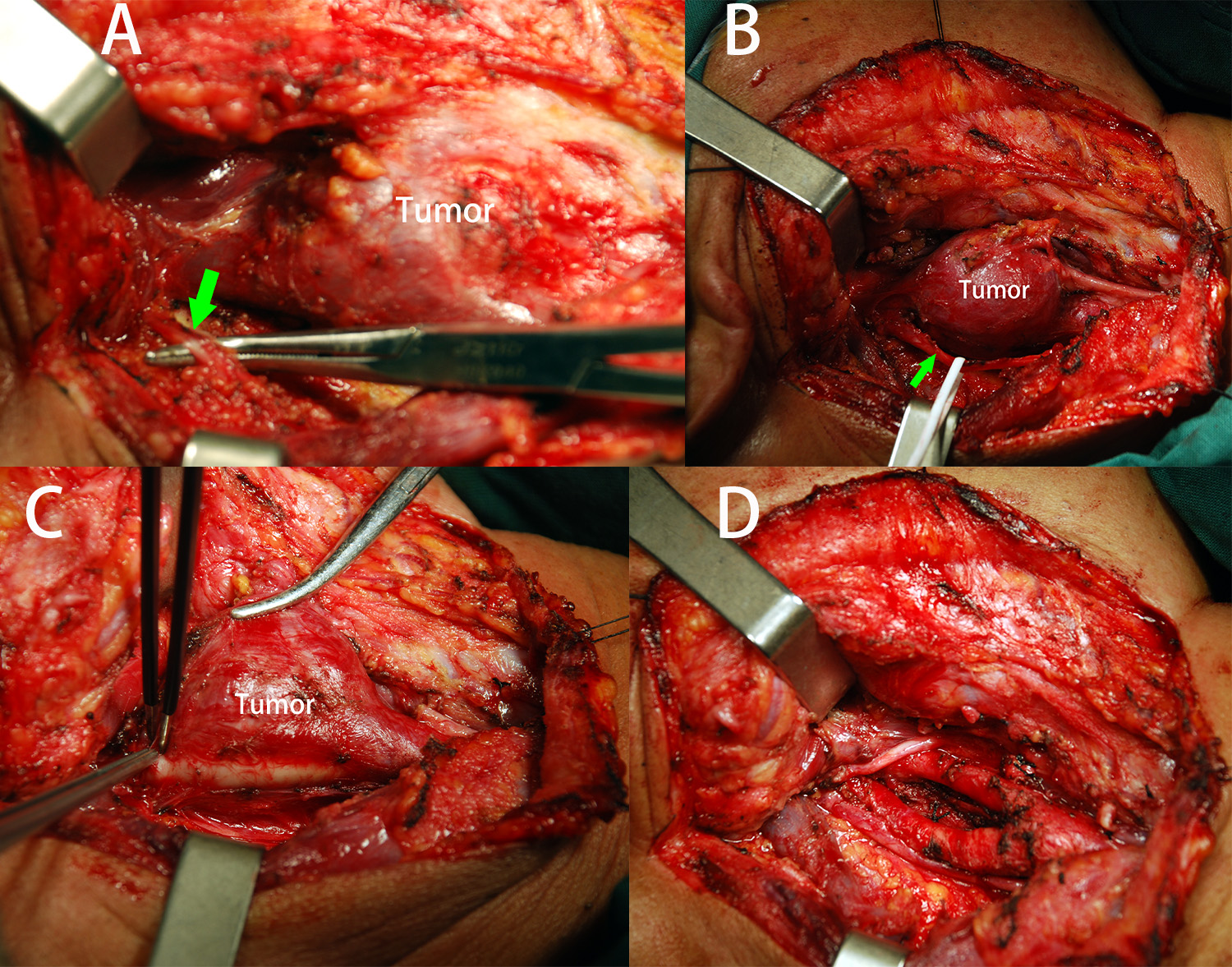
A, Separating and reserving the cranial nerves (green arrow) close to the tumor body; (B) Retraction of the cranial nerves and revealing each border of the tumor to form an “isolated island”; (C) Resection of the tumor started from the “weak point”; (D) After a subadventitial resection of the tumor, the major vessels are well preserved.
Statistical Analysis
Comparison of indices including the Shamblin classification, maximum tumor size, reflux systolic pressure, necessity of vascular reconstruction, intraoperative blood loss, postoperative morbidities and length of stay, and recurrence, between the SG (n = 8) and the CG (n = 29), was subject to a Mann-Whitney U analysis. The value was expressed as mean ± standard deviation, and a probability value of P < .05 was considered to be statistically significant. Statistical analysis was performed using Statistica 16.0 software (StatSoft, Inc).
Results
All 37 patients successfully underwent resection of CBT with use of the “isolated island” technique. Of the 8 advanced age patients included in the SG, 3 were male and 5 were female, with ages ranging from 60 to 76 years (mean = 63.6 ± 5.5 years). With regard to systemic disease, hypertension was detected in 3 patients (1 mild, 2 moderate), and type II diabetes was present in 2 patients, no cardiovascular or cerebrovascular or other chronic diseases were observed. In the CG, there were 12 male and 17 female patients, with ages ranging from 24 to 44 years (mean = 35.4 ± 6.7 years). No systemic disease or other comorbidities were observed in patients of the CG. Follow-up interval for the SG and CG were 22.9 ± 7.1 months and 25.4 ± 10.9 months, respectively.
Comparison of the preoperative indices including clinical symptoms, unilateral or bilateral occurrence, Shamblin classification, dominant nurturing vessels, and maximal tumor size between the 2 groups is presented in Table 1. The prevalence of Shamblin I, II, and III classification in the SG was 12.5% (n = 1), 62.5% (n = 5), and 25% (n = 2), respectively, while in the CG was 10.3% (n = 3), 55.2% (n = 16), and 34.5% (n = 10), respectively. All patients in the SG demonstrated a unilateral occurrence of CBT; whereas in the CG, there were 7 (24.1%) patients who presented with bilateral CBTs. All these 7 patients demonstrated a familial predisposition, 5 of whom underwent a genomic examination and all these 5 patients demonstrated a SDHD mutation. No significant difference in clinical symptoms, dominant nurturing vessels and maximal tumor size were detected between these 2 groups.
The Comparison of the Preoperative Indices Including Clinical Symptoms, Unilateral or Bilateral Occurrence, Shamblin Classification, Dominant Nurturing Vessels, Tumor Size (cm) Between the Study (SG) and the Control Groups (CG).
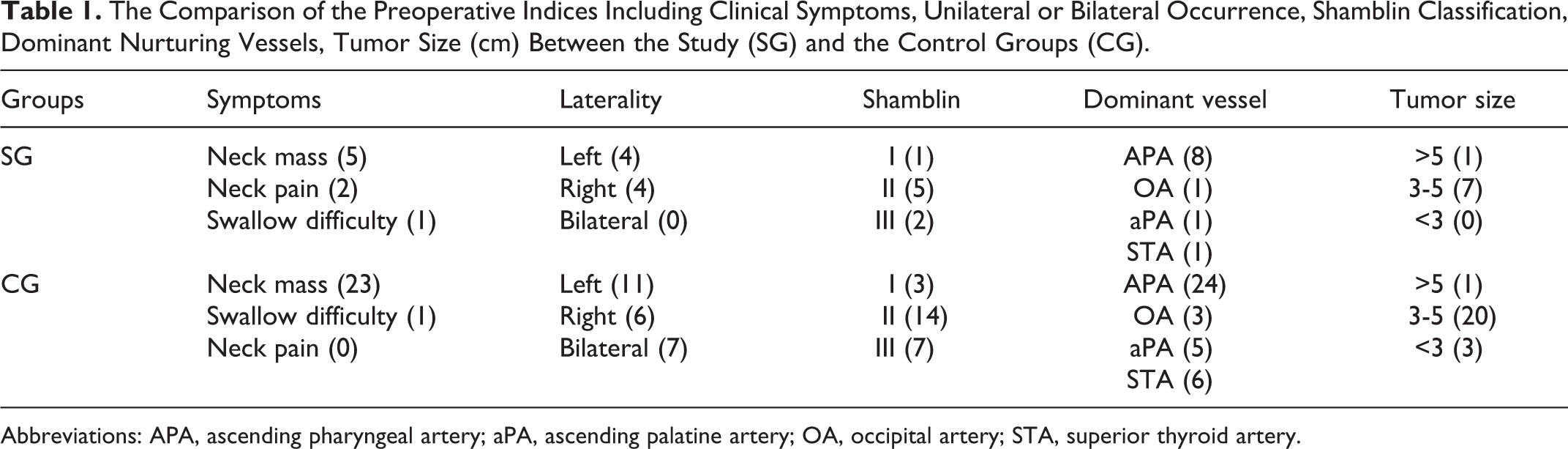
Abbreviations: APA, ascending pharyngeal artery; aPA, ascending palatine artery; OA, occipital artery; STA, superior thyroid artery.
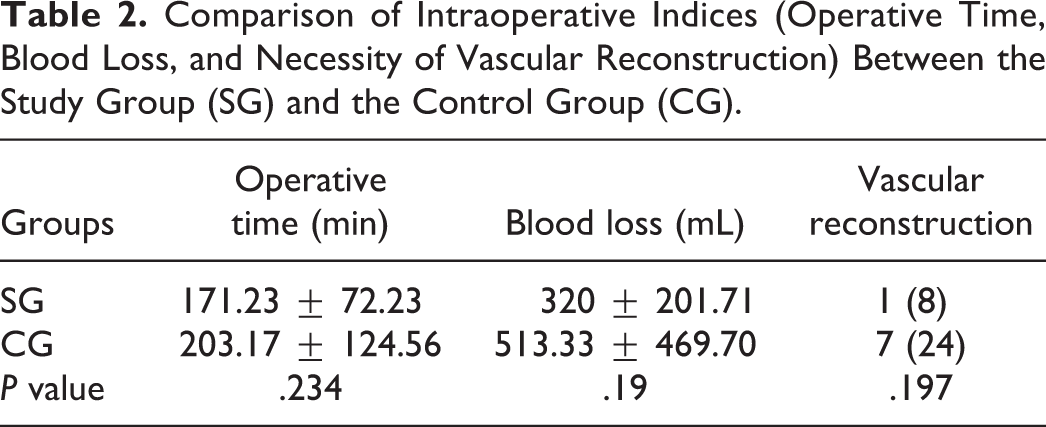
The comparison of intraoperative indices is demonstrated in Table 2. No statistically significant difference of intraoperative blood loss and operative time was detected between the SG and the CG (P > .05). The necessity of vascular reconstruction (Figure 2) was required in one patient in the SG (1/8, 12.5%), while it was necessitated in 8 patients in the CG (8/29, 27.6%).
Comparison of Intraoperative Indices (Operative Time, Blood Loss, and Necessity of Vascular Reconstruction) Between the Study Group (SG) and the Control Group (CG).
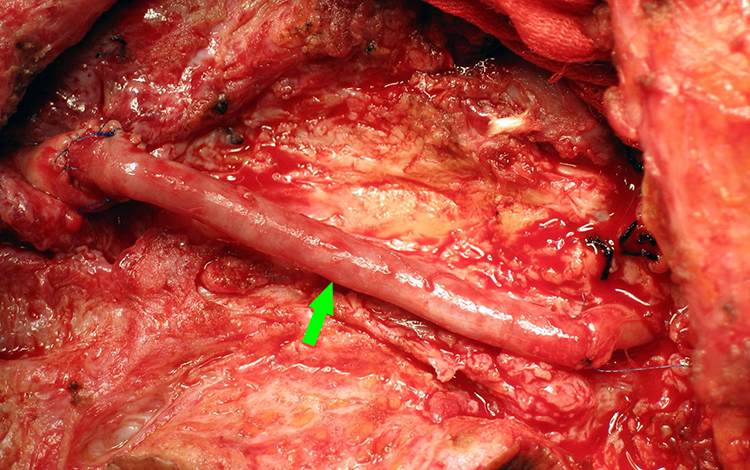
Reconstruction of the internal carotid artery using the saphenous venous.
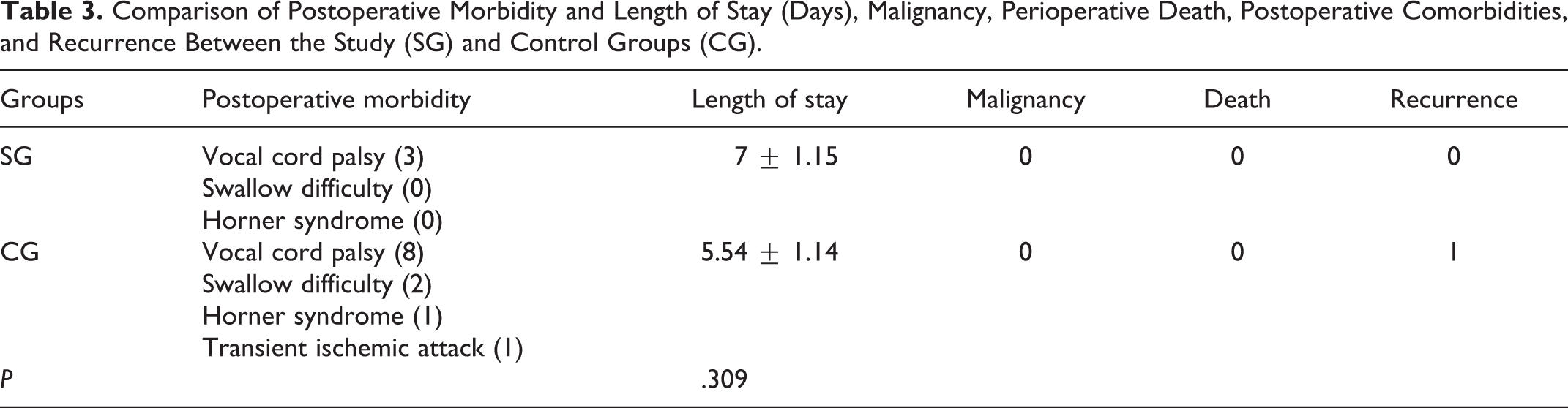
With respect to perioperative issues, comparisons of postoperative length of stay, postoperative comorbidities, and recurrence between these 2 groups are shown in Table 3. The postoperative length of stay in patients of advanced ages (7 ± 1.15 days) was longer than that of younger age group (5.59 ± 1.12 days, P = .004). Transient ischemic attack (TIA) occurred at the second day after surgery in one patient in the CG, which was considered to be caused by carotid artery spasm and subsequently resolved after medical treatment. One patient in the CG recurred during the third year of follow-up. There was no mortality during the perioperative period and the entire follow-up interval.
Comparison of Postoperative Morbidity and Length of Stay (Days), Malignancy, Perioperative Death, Postoperative Comorbidities, and Recurrence Between the Study (SG) and Control Groups (CG).
Discussion
The abundant vascular supply and complex relationship with contiguous neurovascular structures poses significant challenges in surgical resection of head and neck paragangliomas.16,17 Comorbidities such as stroke, TIA, and injury of lower cranial nerves are possible reported complications. For patients of young age with CBT, surgical extirpation is routinely recommended as the treatment option, whereas a strategy of observation or radiotherapy may be more likely recommended for patients of more advanced age (≥60 years old). 18 However, we feel that advanced age should not be an absolute contraindication for surgical extirpation of CBT. This study demonstrated that application of an “isolated island” technique for resection of CBT in patients with advanced age is a rational management approach with seemingly low immediate perioperative and overall postoperative complication rates. However, these results may in part be predicated on a surgeon’s overall skill level and performing these surgical procedures at a high-volume head and neck and vascular surgery center.
A genetic predisposition in patients with CBT was reported in up to 40%, especially in young patients with a familial history.19,20 In addition to the living conditions at high attitude environment as a risk factor, sporadic occurrence of CBT has also been reported to be associated with genetic mutations. 1 Of note, for those with bilateral CBTs, inheritance may play a key role, 21 and a similar familial phenomenon was also observed in 7 patients with bilateral CBTs in our study control group (<45 years old). The SDHx mutation was considered to be the most common type for patients with a familial history or sporadic occurrence of CBT, while the SDHD constitutes the imprinting gene associated with the paternal inheritance of CBT 22 ; 5 of those 7 patients with bilateral lesions underwent genomic analysis also demonstrated a SDHD mutation in this cohort. For patients with bilateral CBTs, the molecular examination for SDHx (SDHD, followed by SDHC, SDHB, SDHAF2) was recommended, and surgical resection commenced from the side with the lower Shamblin classification stage. If no injury of ICA or lower cranial nerves occurred for the operated side, resection of the contralateral side would be considered; or else, observation or radiotherapy for the side with higher Shamblin stage was recommended.21,22 Conversely, all 8 patients with advanced age demonstrated a unilateral occurrence of the lesion, which did not present with a familial predisposition.
The intimate correlation of CBT with the great vessels (common carotid artery or ICA) are commonly seen in Shamblin II and III classifications, which also poses significant challenges and risk of vascular rupture during surgical resection. 8 In the younger age group, the prevalence of Shamblin I, II, and III was 10.3%, 55.2%, and 34.5%, respectively. The temporary intraoperative vascular occlusion followed by vascular reconstruction with usage of saphenous vein were subsequently employed in 8 (27.6%) patients, and no catastrophic events occurred. Given the complex relationship of the CBT with the great vessels and lower cranial nerves, this may become a relative contraindication for surgical resection of CBT in patients of advanced age. In this case series, the proportion of Shamblin I, II, and III for the advanced age group was 12.5%, 62.5%, and 25%, respectively. However, the need for vascular reconstruction in the advanced age group was low (14.3%) in this cohort, and no severe postoperative complications were detected. We may therefore propose that temporary vascular occlusion and the need for subsequent vascular reconstruction are not always needed, which may not be an absolute contraindication to perform a CBT resection in patients of advanced age too.
The “isolated island” technique was not innovative, and previously described where the dissection started gradually from the periphery weaker points toward the central portion of the tumor achieving complete resection. 16 Upon adoption of an “isolated island” technique, separation from the weak point was employed first, or the portion of the tumor body which adheres less intimately with the great vessels was separated in a subadventitial plane, leaving the resection of most adherent portion as the last step. In addition to the judgment based on preoperative radiological assessment, the strategy of preservation or reconstruction of the carotid arteries could also be modified at this stage. The “isolated island” technique has been successfully applied in all 37 patients with CBT, and no inadvertent injuries to the great vessels occurred. Therefore, the “isolated island” technique may be an appropriate technique for surgical extirpation of the CBT, including those patients with advanced age.
Postoperative complications and mortality subsequent to resection of the CBT have been occasionally reported.23,24 Generally, vascular fragility is routinely increased in advanced age, and more vulnerable to be damaged by comparison with that of arteries in younger patients. Therefore, the subsequent risk of comorbidities related to resection of CBT would also be increased in patients with advanced age. To perform a CBT resection, the patient must be in good enough health to undergo surgery and general anesthesia. Moreover, systemic disease such as hypertension, type II diabetes, and other cardiovascular or cerebrovascular lesions may also preclude resection of a benign lesion intimately adherent to great vessels, especially for patients with advanced age. Our current study shows that patients of advanced age have a longer postoperative length of stay, but there were no statistically significant increases of vascular rupture or additional lower cranial nerve injuries when compared to the younger age group. However, the enrolled patients of advanced age who underwent CBT resection in current study did not harbor any cardiovascular or cerebrovascular or other chronic diseases, which is critical to come into a treatment plan. Therefore, surgical resection of CBT in the elderly patients can be achieved safely but requires careful patient selection and high-volume expertise at a tertiary referral specialty center.
In accordance with the experience from other centers, surgical resection of CBT was routinely performed by a team composed of a vascular surgeon and a head and neck surgical oncologist, especially for those patients with Shamblin II and III clinical subcategories.6,16 Vascular reconstruction was performed by a high-volume vascular surgeon when reconstruction was necessary. Of note, in addition to the patients’ treatment preferences, the decision to extirpate a CBT in advanced age group needs critical careful multidisciplinary discussion prior to surgery. In our center, a DSA examination is routinely performed for patients with CBT who underwent surgical extirpation, which is also the prerequisite for all patients with advanced ages. Only patients with good anterior and posterior communications and the systolic reflux pressure higher than 60 mm Hg was appropriately selected in case that the inadvertent rupture of great vessels were to occur. 25 Furthermore, preoperative embolization of nurturing vessels for CBT (ie, ascending pharyngeal artery) was employed in our early stage experience; however, it was later not commonly performed as it did not seem to decrease intraoperative bleeding.
There are significant limitations to this study. It is in essence a retrospective study with a small sample size for patients of advanced ages, which limits the quality of evidence to propose a rational treatment strategy for surgical management of CBT in patients of advanced ages. Moreover, the average age of patients in advanced age group was 63.6 ± 5.5 years, we did not have experience for surgical extirpation of patients with very old age (more than 75 years old). Furthermore, the eventual impetus to remove a CBT in patients with advanced ages is determined by many variable factors, including the general condition of the patient to tolerate the anesthesia and surgical procedure, comorbidities (eg, cardiovascular or cerebrovascular or other chronic diseases), functional status of the lower cranial nerves, the appeal and willingness of the patients to choose a surgical treatment option, and the weighing of the overall risks, benefits, and alternatives. 26 Therefore, we are not advocating for surgical resection of CBT in all patients with advanced age; however, surgical resection may be appropriate is select motivated patients and can be performed safely in a high-volume specialty center.
Conclusion
Surgical resection of CBT in patients of advanced age seems reasonable when the surgical indication is appropriately selected. The “isolated island” technique is safe for extirpation of CBT in both young and advanced age groups with seemingly low postoperative complication rates.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: N.R.L. holds stock in Navigen Pharmaceuticals and was a consultant for Cooltech Inc.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the National Key R&D Program of China (2019YFC0119300).