
Abstract
Hemangiopericytomas (HPCs) are rare vascular tumors, and head and neck hemangiopericytoma (HNHPC) accounts for 11% to 16% of all HPCs, possibly occurring at any age. However, according to a recent study, HNHPC was most frequently observed in middle-aged adults and had a slight predominance of female patients. In the present case, we report the successful treatment of HNHPC.
Introduction
Hemangiopericytomas (HPCs) are rare vascular tumors that were first described by Stout and Murray in 1942. The tumor originates in the pericytes, arranges alongside the capillary vessels, and has smooth muscle characteristics. HPC most commonly occurs in the lower extremities and retroperitoneum. Other sites, including the head and neck, include the neck, mouth, and sinonasal tract soft tissues. HPCs are rare vascular tumors, and head and neck hemangiopericytoma (HNHPC) accounts for 11% to 16% of all HPCs possibly occurring at any age. 1 The diagnosis of HNHPC relies mainly on histological examination. The primary treatment of HNHPC is complete resection, and the effects of radiation therapy and chemotherapy are uncertain. However, some studies recommend implementing chemotherapy or radiotherapy if common cancer-related adverse events, such as positive surgical margins and poor pathologic differentiation, are encountered. A large tumor size (>5.0 cm), poor pathological differentiation, and nonsurgical treatment are associated with the recurrence and metastasis of HNHPC. Lifetime clinical follow-up is warranted to improve survival rates, as most studies have reported late recurrences. Here, we report a case of HPC resected from the left-lateral neck of a 43-year-old man who presented to our hospital with progressive enlargement of a left-sided neck mass.
Case Report
A 43-year-old man presented to our hospital with a huge left-lateral neck mass growing slowly over 2 years (Figure 1A) and was hospitalized. The patient had no previous history of chronic disease or surgery but had a 20-year history of smoking. The tumor was painless and not associated with systemic symptoms; however, some slight compression-related symptoms, including occasional choking after eating and slight gasping after general activity, were observed. The mass was fixed, non-tender, did not fluctuate, and had a general texture on palpation. The mass measured 13.1 × 8.8 cm (Figure 1B). Routine laboratory test results were within normal limits. Magnetic resonance angiography and computed tomography (CT) imaging showed that the upper margin of the mass was 3.3 cm from the skull base, and compression of the bilateral internal carotid artery, bilateral common carotid artery, and left internal jugular vein were obvious, greatly increasing the risk of bleeding and the difficulty of ligation. The lower part of the mass was located between the trachea and esophagus and was partially adhered to the esophagus. Digital subtraction angiography (DSA) was performed before surgery to clarify the vascular supply to the mass and reduce intraoperative bleeding. DSA showed that the blood flow in the left common carotid and internal carotid arteries was not blocked, and a branch of the external carotid artery supplied the mass; thus, we performed vascular embolization to reduce intraoperative bleeding.
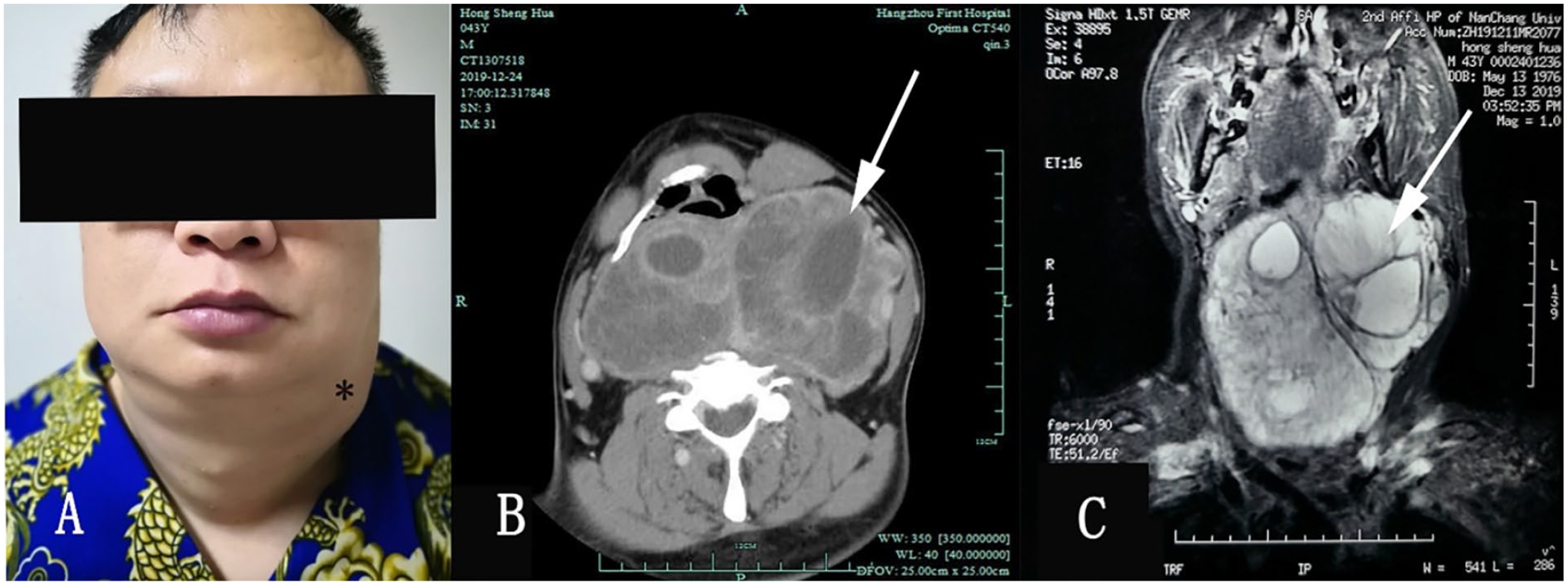
A huge mass on the left side of the neck before the surgical resection (A). Enhanced CT scan (B) showing an inhomogeneous enhancement in the mass. Vital tissues and vessels around the mass were not violated. MRI (C) of the neck revealed that the giant mass (about 13.1 × 8.8 cm) was found in the prevertebral space.
After the preliminary investigation, the patient underwent surgery. A tracheotomy was performed to reduce the risk of surgery, and complete surgical excision of the neck mass was performed under general anesthesia using an extra-cervical approach. An H-shaped incision was made in the neck, and the neck skin, subcutaneous tissue and platysma muscles were separated layer by layer. A single, large, and well-circumscribed tumor was found in the prevertebral space after excising the left sternocleidomastoid muscle. The upper margin of the tumor was close to the skull base, and the lower margin was close to the entrance of the thorax. The surrounding tissues, including the thyroid, superior laryngeal nerve, middle thyroid vein, internal jugular vein, and common carotid artery, were displaced laterally due to the tumor. After careful sharp and blunt dissection, the anterior, posterior, and medial margins of the mass were completely dissected from the neck (Figure 2A). The surgery was successful, with no damage to the surrounding tissues during the tumor resection.
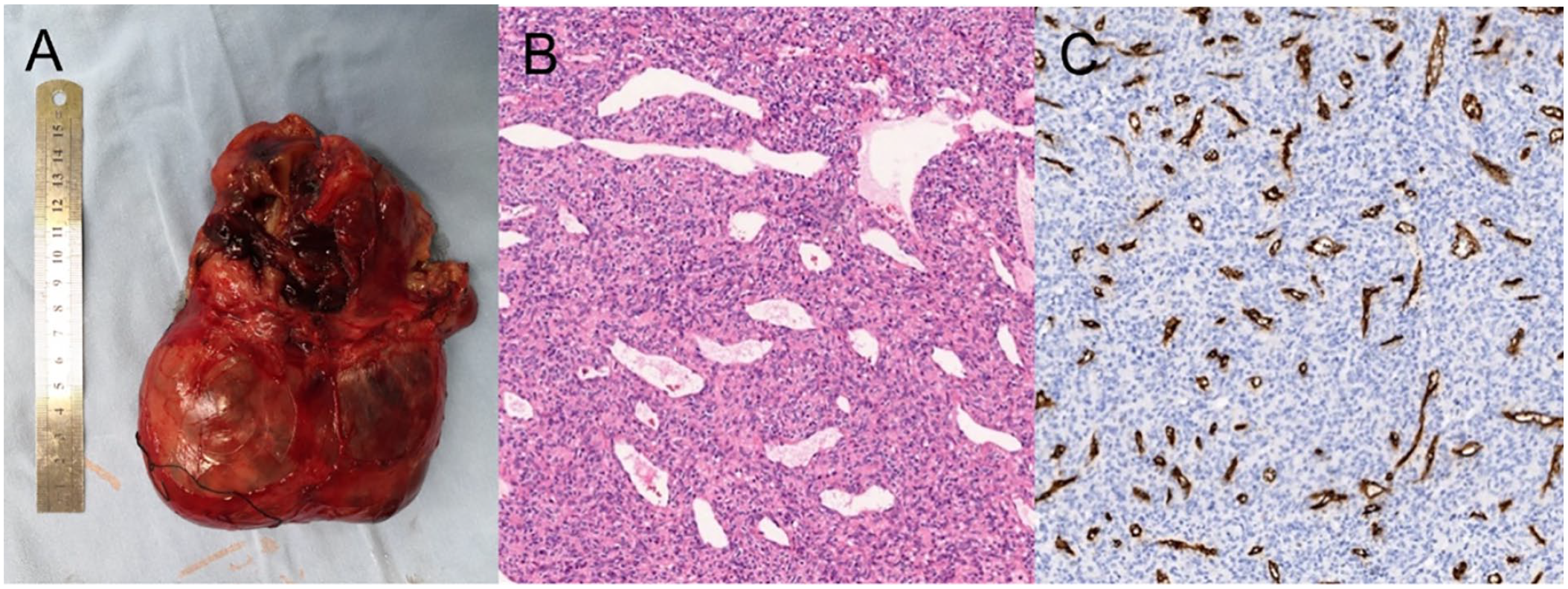
The mass was completely dissected from the neck’s contents, measuring 15.0 × 13.0 × 4.0 cm in size. The tumor’s interior was not completely solid, and 10 mL of yellow liquid was extracted during the operation (A). Histologic appearance of HPC. The tumor showed compact and uniform cells with a large number of small vascular cavities and compact reticular fibers with hematoxylin and eosin stain (HE) × 200 (B). The positive staining of CD34 was brown granular in the cytoplasm (×100) (C).
The postoperative pathological report suggested that the mass was a HPC. Immunohistochemical analysis of the mass showed that the cells were positive for VIM, Desmin, Caldesmon, Collagen IV, and CD34, whereas they were negative for CD117, S-100, and Syn. Gross examination revealed it to be an oval mass, encapsulated, and 15.0 × 13.0 × 4.0 cm in size, with abundant and slightly dilated blood vessels on the surface (Figure 2B and C). The tumor’s interior was not completely solid, and 10 mL of yellow liquid was extracted.
Three months later, at the scheduled follow-up, the patient had recovered well with no postoperative complications, and compression-related symptoms, such as slight asthma and dysphonia, had resolved. CT revealed no evidence of recurrence or residual disease (Figure 3B).
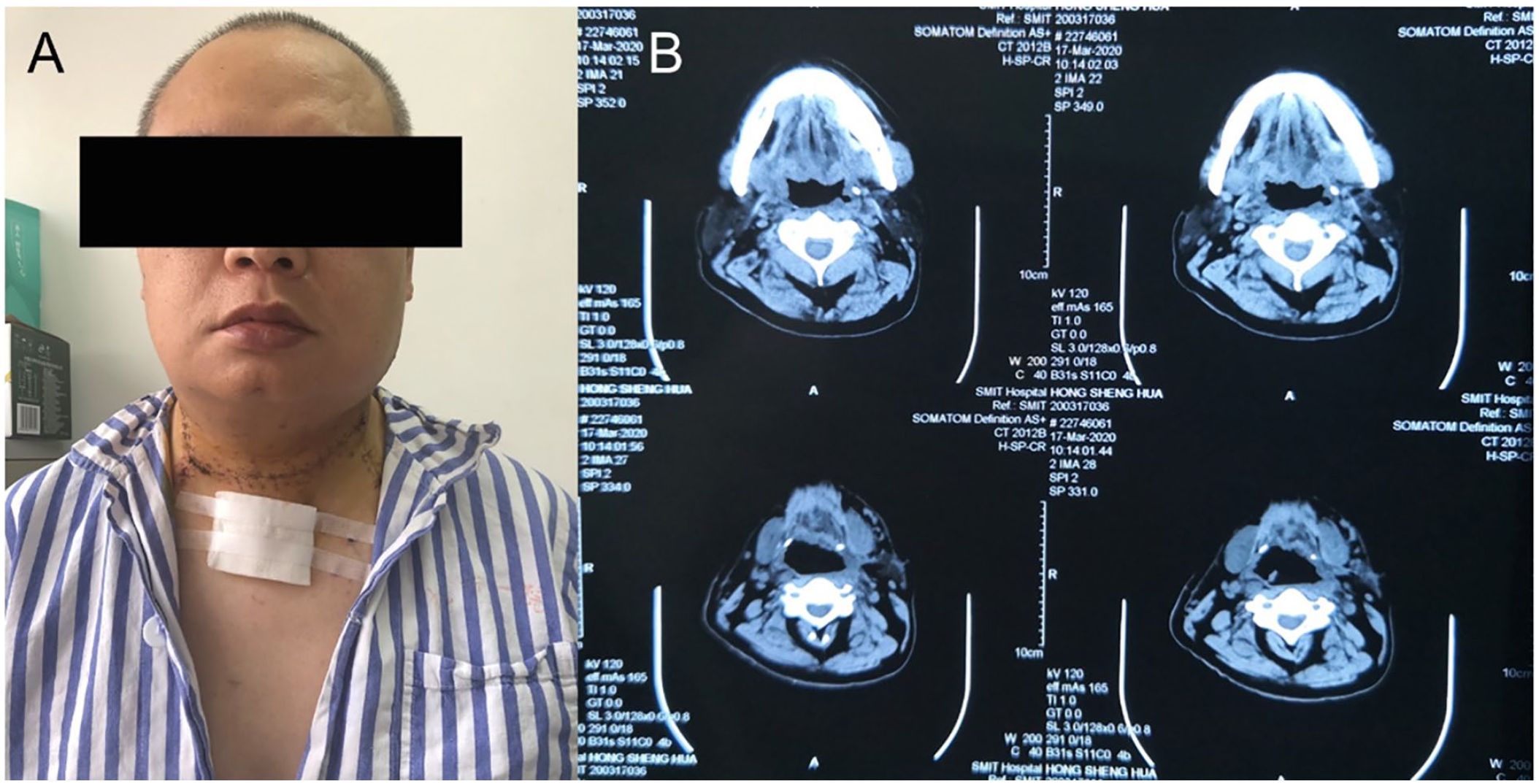
The patient recovered well after the operation without any postoperative complications found (A). CT scan was performed 3 months after the operation—no evidence of recurrence (B).
Discussion
HNHPC most commonly occurs in the connective and soft tissues of the head and neck, followed by the sinonasal cavities and orbit. Compared to other HPCs, HNHPC presents with a significantly smaller tumor size, averaging 4.5 cm. 2 The post-styloid compartment contains the internal carotid artery; internal jugular vein; cranial nerves IX, X, XI, and XII; cervical sympathetic chain; and the lymph nodes. Combined with preoperative patient imaging data analysis, the evaluation of tumor size, location, and anatomical relationship with the important surrounding neurovasculature is an important reference for selecting surgical access. To ensure surgical safety, the tumor should be removed completely to avoid any tumor residue. Immunohistochemical studies have suggested that patterns of vimentin, FXIIIa, FVIIIa, CD34, CD99, p16, and bcl-2 positivity are consistent with the diagnosis of HPC.3,4 In addition, Soriano-Hernandez et al 5 reported that CD34 is an ideal marker for diagnosing atypical HPC. Owing to the low prevalence and nonspecific symptoms of HNHPC, surgical resection appears to be the primary treatment. The diagnosis of HNHPC mainly relies on the histological examination. Complete resection is the primary treatment in the patients with HNHPC. The effects of radiation therapy and chemotherapy are uncertain, although it is recommended in some studies that chemotherapy or radiotherapy could be implemented once common cancer adverse factors are identified, such as positive surgical margins, poor pathologic differentiation, and so on. Large tumor size (>5.0 cm), poor pathologic differentiation, and nonsurgical treatment are related to the recurrence and metastasis of HNHPC. Lifetime clinical follow-up is warranted to improve the survival rate since late recurrences have been reported in most studies.
Footnotes
Data Availability Statement
All relevant data are within the article and its additional files.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Statement of Informed Consent
There are no human subjects in this article and informed consent is not applicable.