
Abstract
Background:
India announced nationwide lockdown on March 24, 2020, to control the COVID crisis. Due to lockdown, the health care system, that is, delivery and utilization of the health facilities were adversely affected.
Clinical Setting:
Presentation and management of nasal foreign body cases over 3 months post COVID lockdown has been discussed. Factors for delayed diagnosis and management are assessed and compared with pre-COVID era.
Result/Outcome:
Due to lockdown and COVID phobia, more complicated cases of nasal foreign body are presented in post lockdown period.
Conclusion:
We need to formulate and standardize the management strategies to avoid such unfortunate circumstances so that even non-COVID cases are managed more appropriately and in a timely manner.
Introduction
The corona virus disease (COVID-19) was declared a global pandemic by World Health Organization on March 11, 2020. 1 Swift actions taken to combat and restrict the spread of the disease included rigorous lockdown, cessation of international travel, restricted movement, screening, and isolation of the suspected and confirmed cases.2,3
In order to mitigate the rapid spread of the virus and to prepare the health care sector to deal with this sudden health crisis, Government of India announced country wide lockdown starting from March 24, 2020. 3 This pandemic has had hit our economy hard by negatively impacting each and every sector of our economy especially the travel and tourism industry, education system, and public health care sector ultimately leading to a temporary economic lockdown.4,5 To cope with this crisis, non essential services were kept on hold and a large proportion of existing resources were channelized to manage COVID patients. 3 Besides this, restricted movement, sudden halt of public transportation, loss of income, and COVID phobia all led to delay in seeking medical help. As a result, more complicated cases were registered when the country started to unlock.
In view of the above scenario, we strive to analyze the subtle rise in number and varied presentation of nasal foreign bodies during the post lockdown period at our tertiary care pediatric center.
Cases
Eight children reported in our ENT outpatient department between June 1, 2020, to August 31, 2020, with complaints of persistent nasal blockage and obstruction, mucopurulent discharge, and epistaxis. Of these 8, only 2 patients had a clear history of nasal foreign body insertion but could not seek timely consultation due to the ongoing lockdown.
Clinical examination was done in strict compliance with the prescribed guidelines advised by our institute to prevent COVID infection. Anterior rhinoscopy revealed unilateral mucopurulent discharge in most of them along with granulations, mucosal erosions, crusts, and clotted blood. Although suspicion of nasal foreign body was kept in mind but no foreign bodies were visualized during clinical examination. Awake nasal endoscopy was deferred to limit aerosol generation, which was expected to be significant due to crying in a pediatric patient. Imaging in the form of X-ray or computed tomography (CT) scan (Figures 1 and 2) was advised depending upon the cases and children were worked up for endoscopic evaluation under general anesthesia. Details and outcome of all 8 cases are tabulated in Table 1.
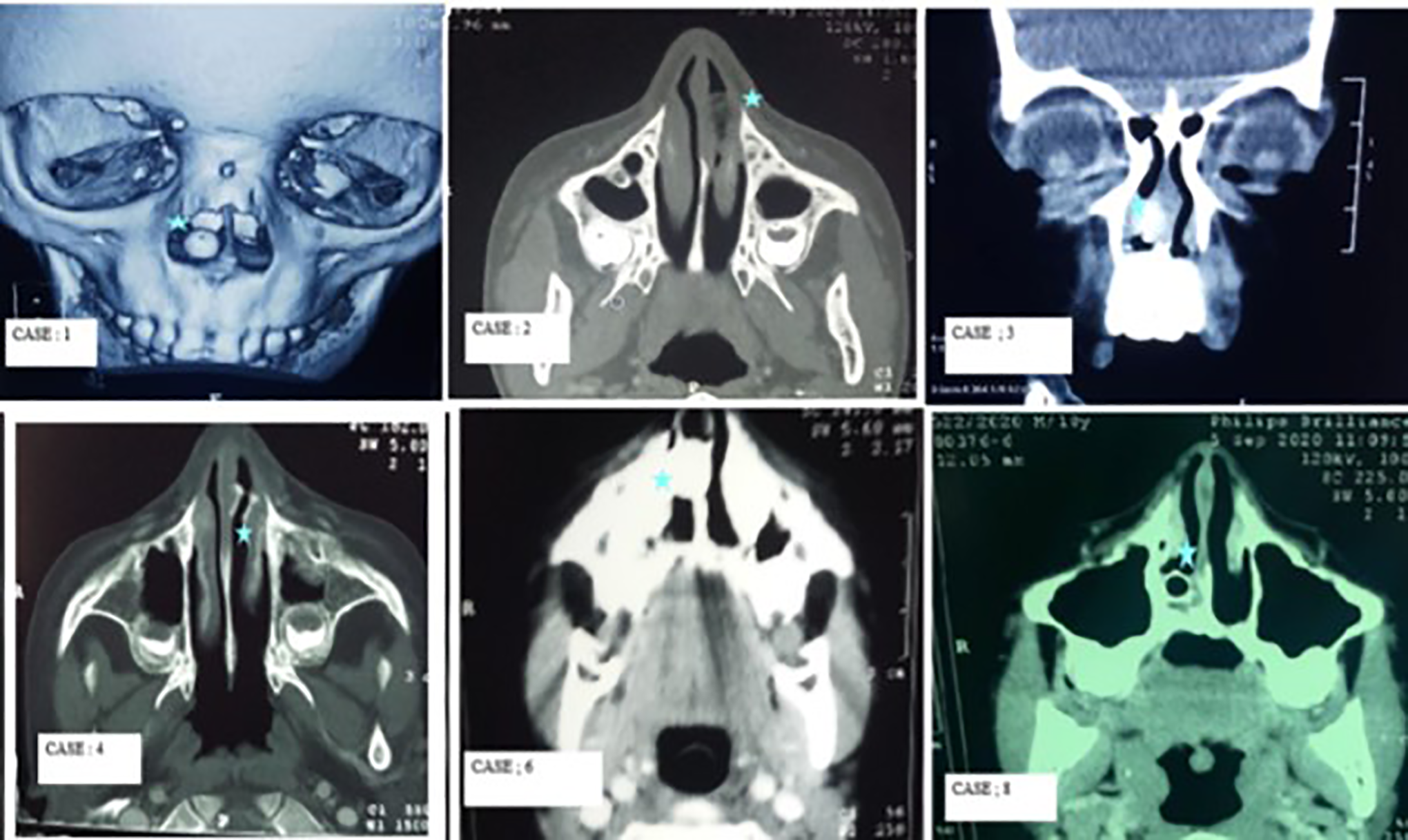
Computed tomography (CT) images of cases showing foreign bodies in the nasal cavity (5-point star). Case: 1—Incidental finding right nasal cavity opaque spherical Foreign body. Case: 2—Heterogenous soft tissue density lesion measuring (17 × 12 mm) with mottled density seen in anterior part of left nasal cavity. Case: 3—Iso to hypodense lesion (10 × 7 mm) in right nasal cavity with focal calcification. Case: 4—A dense hollow cylindrical shaped structure (600 HU) around 10.0 × 8 × 7 mm seen in anterior part of left nasal cavity. Case: 6—Well-defined solid radio dense lesion (3000 HU) with streak artefacts seen in right nasal cavity, impinging on the cartilaginous part of nasal septum causing ulcerations. Case: 8—Spherical hollow foreign body around 8-mm diameter with hyperdense margins (800-1200 HU) seen along the floor of right nasal cavity with mucosal thickening.
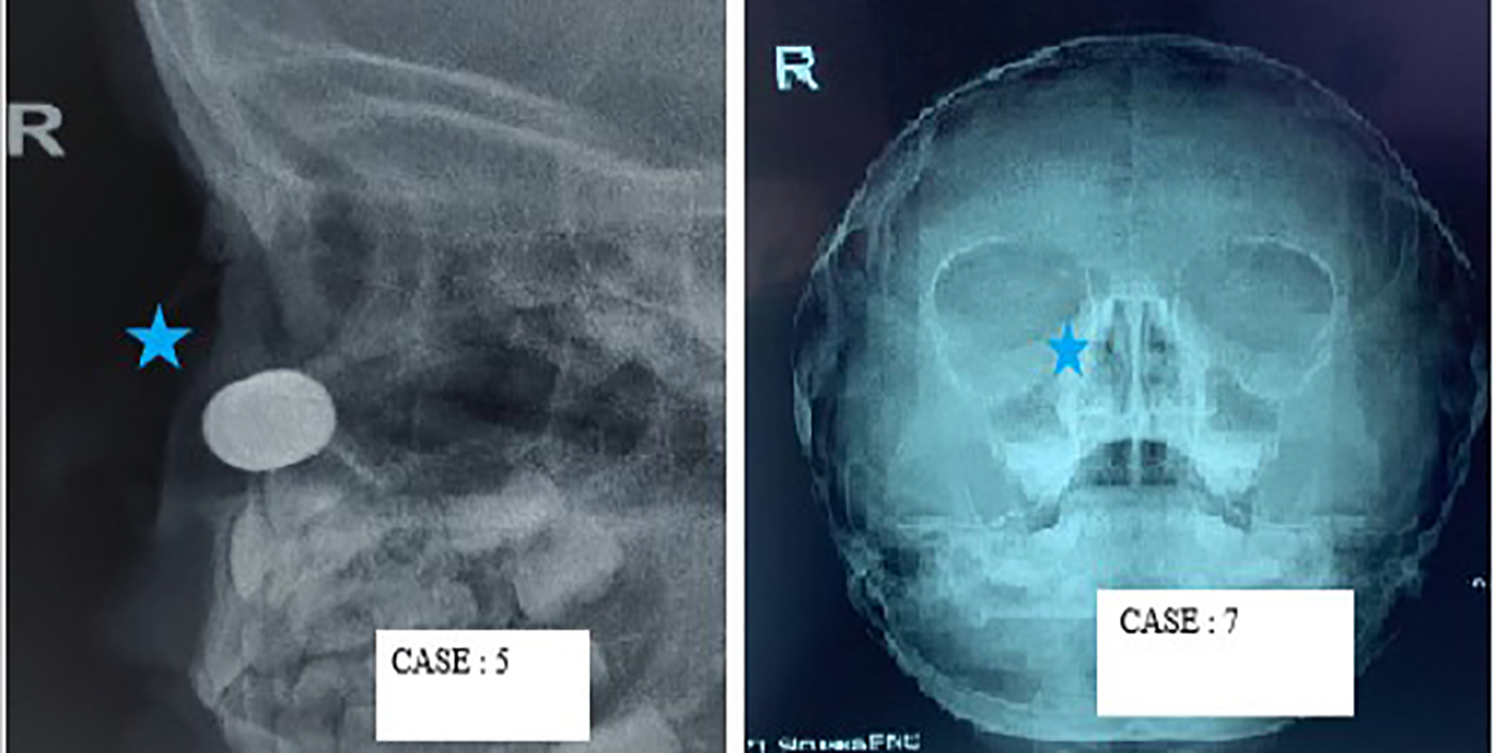
Nasal X-ray of cases with nasal foreign bodies (5-point star). Case: 5—Radio opaque object visible turned out to be 2 magnets. Case: 7—Faint shadow of LED bulb filament is visible on right side.
Characteristics and Outcome of 8 Children With Nasal Foreign Body (FB).
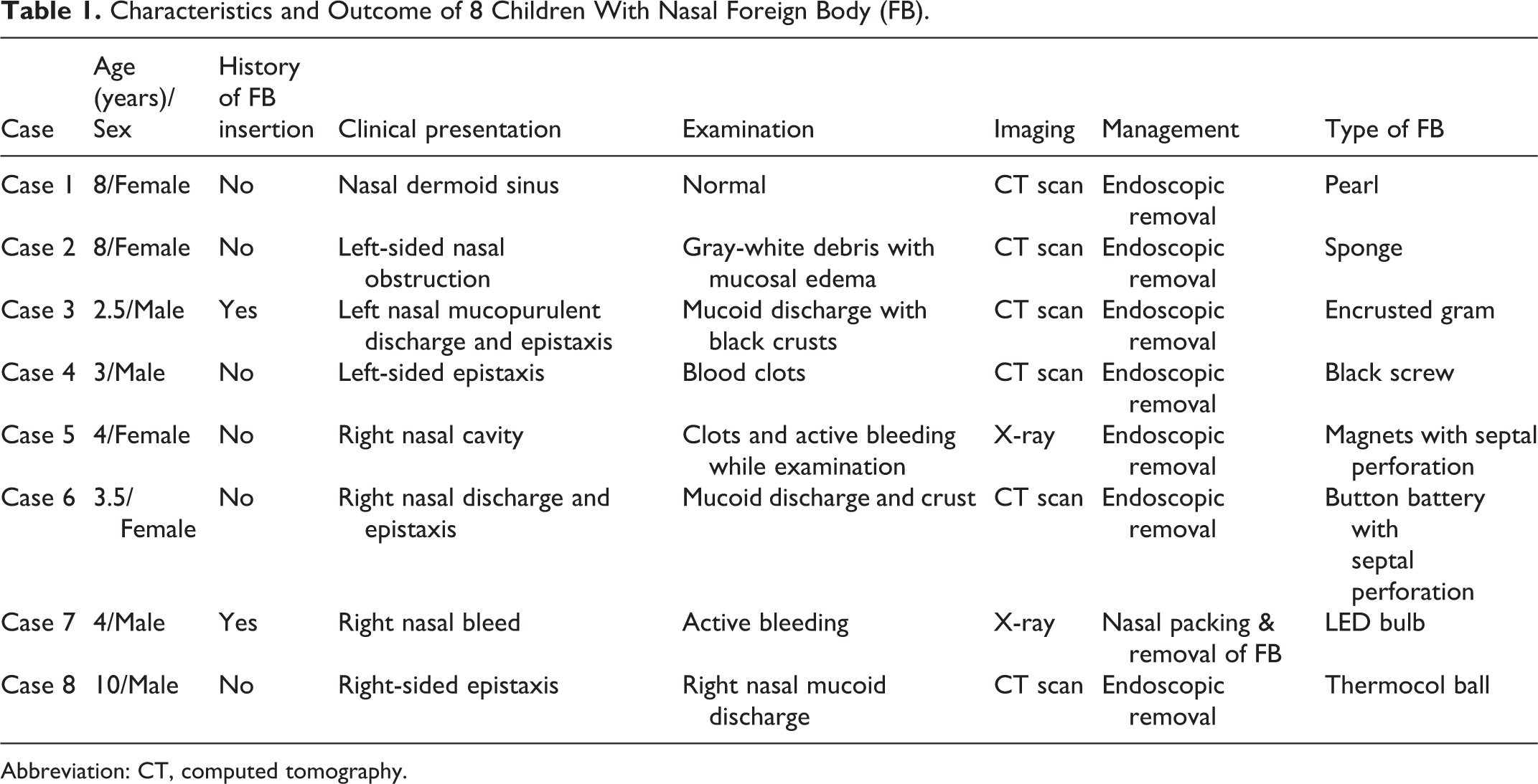
Abbreviation: CT, computed tomography.
In addition, factors that contributed to delayed diagnosis, seeking of medical help, and therapeutic delay are also assessed and tabulated in Table 2.
Factors Contributing for Delayed Presentation and Management.
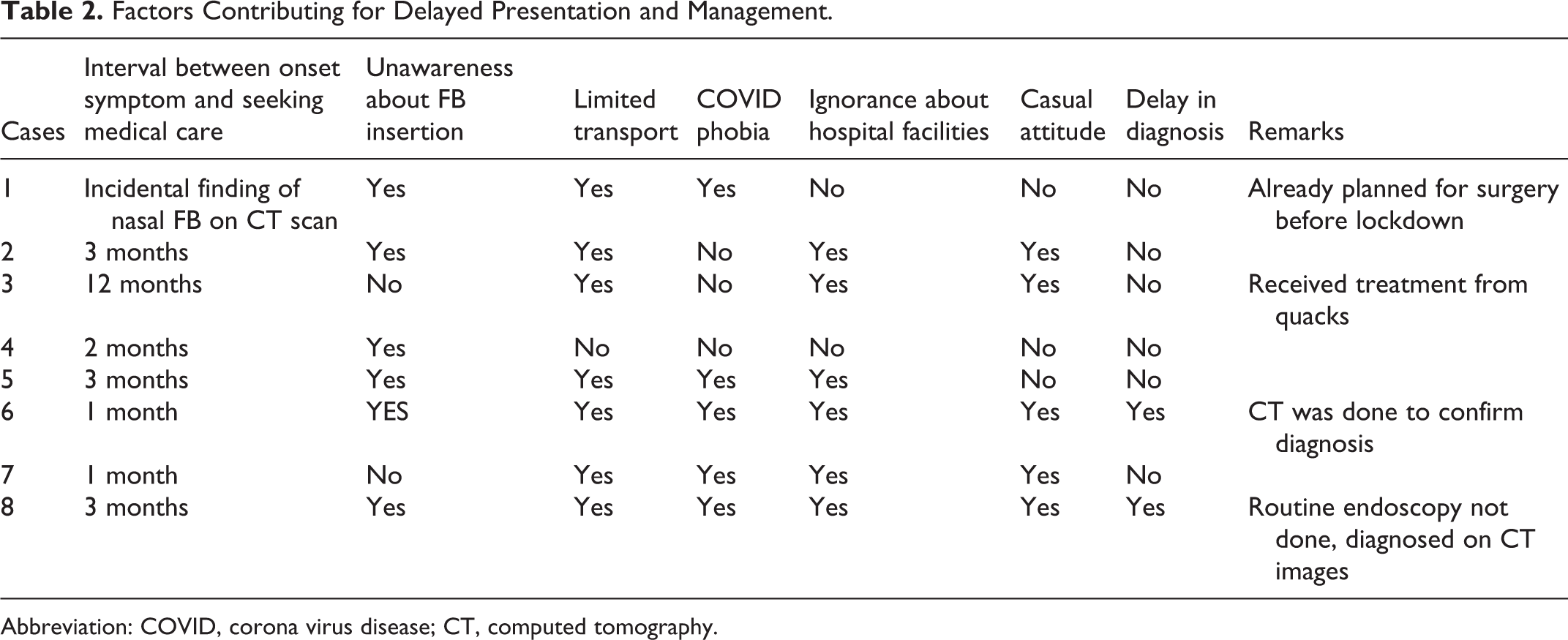
Abbreviation: COVID, corona virus disease; CT, computed tomography.
We found significant time lag between onset of symptoms and time of seeking medical care. Reasons of delayed presentation varied from patient to patient, including casual attitude of patients’ attenders, COVID phobia, restricted movement, limited transport facilities, shutdown of private clinics, and poor financial status. Besides these factors, the general population were not aware about the existence of non-COVID centers and the available facilities. The most common reason stated was that they were not able to come as the hospitals were nonfunctional according to them. Referred patients were not timely referred to higher centers due to the abovementioned limitations. All these factors led to delayed presentation of cases ranging from 4 weeks to 9 months.
Beside delayed presentation, incomplete history and long-standing pathology led to delayed diagnosis by clinicians due to limited staff, resources, and the need to adhere to new guidelines and protocols. There were also unavoidable delays in laboratory and radiological investigations due to restrictions of timings of work. Moreover, limitations of operating facilities and mandatory COVID screening prior to any procedure contributed to delayed diagnosis and management.
In pre-COVID settings, any child who presented with unilateral nasal discharge/epistaxis, awake nasal endoscopy was done in outpatient clinic and any foreign body if visualized was removed in the same setting. Seldom imaging was required in these cases. However, during COVID pandemic, we prefer to get a CT scan/X-ray in almost all cases to avoid outpatient-based endoscopies. Although such cases were simple and easy but this delay in process lead to few complications and increased morbidity of patient.
In all the cases, foreign bodies were visualized, easily removed (Figure 3) and postoperative period was uneventful. But in 2 cases (cases 5 and 6), septal perforation was encountered due to chemical leak from magnets and battery. In case 7 (LED bulb), nose was packed for 24 hours to control epistaxis.
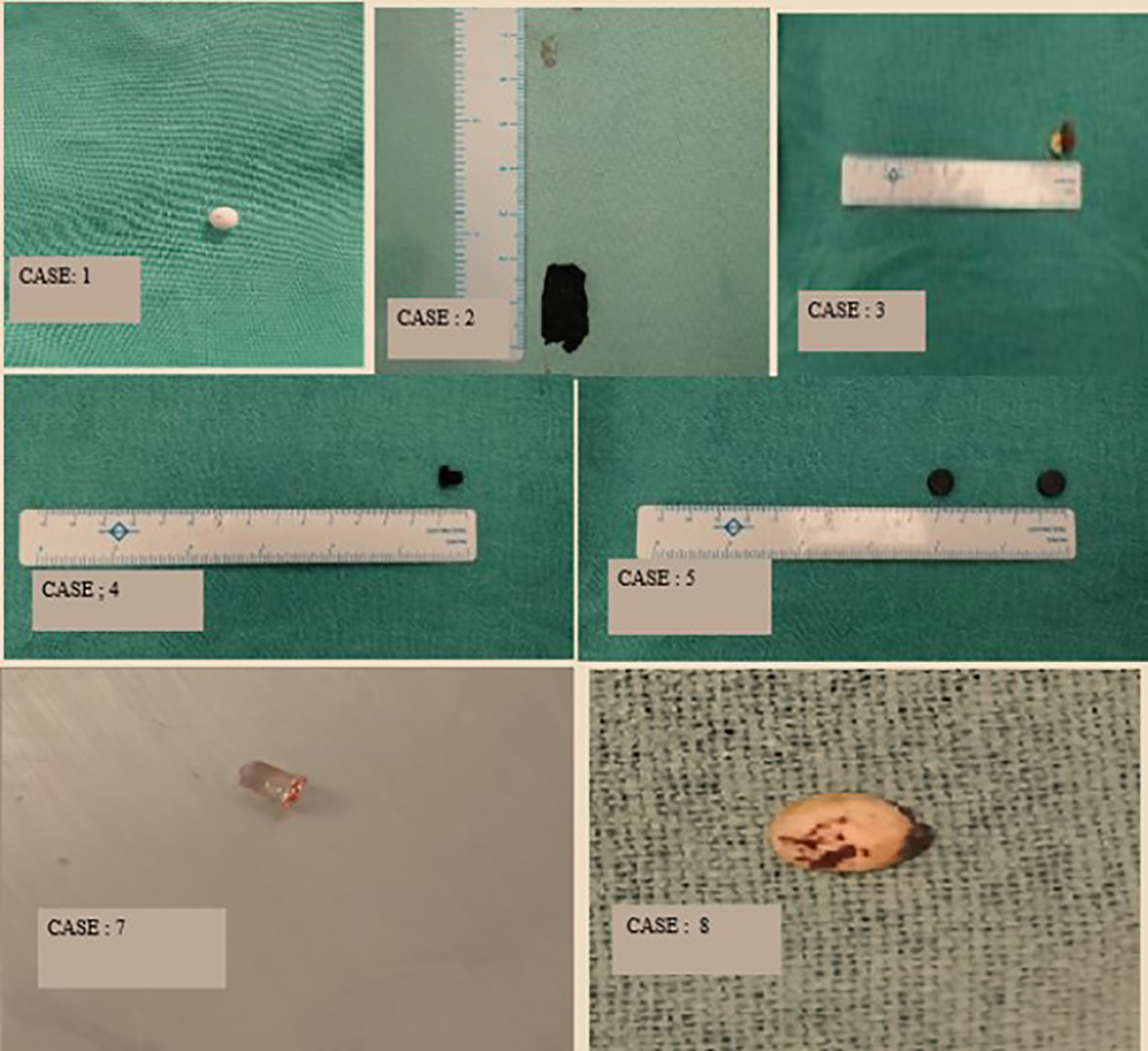
Image showing nasal foreign bodies removed such as pearl, sponge, encrusted gram, plastic screw, 2 magnets, LED bulb, thermocol.
Discussion
The COVID-19 pandemic has significantly and adversely affected our lives and resources. To slow down the spread of the virus, the Indian government had implemented a country wide lockdown in late March 2020, which continued till May 2020. 2 Although the lockdown has bought us time to deal with this unprecedented situation and somewhat flattened the curve, it had impacted our economy adversely and resulted in widespread unemployment, hunger, and inaccessibility to health care.4,5
During this pandemic, the escalated number of COVID cases in India led to drastic rise in demand for health care facilities. 3 The apex hospitals with the best infrastructure and equipped with huge number of beds and other facilities were exclusively allotted to cater to COVID patients. These hospitals stopped holding normal OPDs for the general non-COVID cases. This negatively affected the radius population it was previously catering to. The country wide lockdown and COVID phobia had led to sharp decline in the number of patients seeking health facilities, especially for routine checkups, elective and nonemergent conditions. Although essential health care facilities remained open but restricted international and domestic travel affected patients flow to the hospitals. Fear of contracting the disease prevented the general public to approach even the nearest health care facility until and unless it was an emergency. Moreover, Government of India had also issued an advisory on postponing elective and nonessential services to deal with this crisis. 3 Due to lockdown, there was significant reduction in number of referrals from other hospitals or dispensaries. This all led to potential delay in diagnosis and treatment of acute and chronic conditions, resulting in presentation of more complications of otherwise simple and straightforward cases such as nasal foreign bodies.
Being a pediatric tertiary care center, we had dealt with nasal foreign bodies on day-to-day basis but due to the abovementioned reasons, we encountered more complicated cases of nasal foreign body in our center during unlock period. We wanted to share our experience to convey how a simple, OPD treatable condition can turned into a complicated case without timely intervention. Such cases imposed an additional psychological and economic burden on the patient and family as well as health care system due to multiple hospital visits, diagnostic procedures, sedation, and hospital stay. Also technical challenges and modifications to manage such cases due to the ongoing pandemic has been mentioned.
As such nasal foreign bodies are very common finding in pediatric group 6 and mostly that include rubber, eraser, paper, pebbles, pearls, beans, sponge, nuts, chalk, wood pieces, metal bolts, small parts of toys, and so on. 7 Children have a natural tendency to insert anything and everything into nose, ear, and mouth while playing. Reason can be as simple as to relieve a minor itch or to tease their peers. 6 Usually nasal foreign bodies are diagnosed clinically on anterior rhinoscopy and often has clear-cut history of something in the nose.6,7
In many instances instead of being located in the anterior part of nose, sometimes foreign body may lodge posteriorly and has a potential to be dislodged into the airway leading to life-threatening acute respiratory obstruction. 7 Nasal foreign bodies carry an additional risk of being carriers of the causative organisms of the many infectious diseases. 8 Therefore, however small they look, nasal foreign bodies should not be taken lightly.
Missed or ignored foreign bodies may persist for longer periods and this delay in diagnosis or presentation can lead to a number of complications. Inflammatory changes in adjacent tissue results in mucosal erosions, ulceration, epistaxis, and over a period of time foreign bodies get encrusted. 7 In the later stage, they may present as rhinolith due to accumulation of minerals over them. 6 Batteries leak toxic chemicals and has a corrosive effect on the sensitive nasal mucosa. 9 Both pressure necrosis and direct current effects on the mucosa contribute to extensive tissue damage. Paired magnets also create a current with similar results which can lead to a septal perforation 10 if not dealt with promptly. These mucosal changes, that is, edema, granulations, or calcifications tend to conceal the clinical picture of a nasal foreign body and may mimic as sinusitis, tumor, and bleeding polypus. Sometimes, diagnosing nasal foreign bodies can be challenging 6 and in such cases imaging is helpful to rule out other differentials. 11
In 2 of our patients, magnets and button battery persisted in the nasal cavity for an unknown period of time which led to septal perforation. Unilateral nasal discharge especially in child should raise the suspicion of the nasal foreign body, until proven otherwise.6,7 Long-standing nasal foreign bodies may present with nasal obstruction, foul smell, epistaxis, and anosmia. Most of our patients presented with unilateral nasal discharge. Few cases also presented with epistaxis. Thus, a thorough physical examination involving anterior rhinoscopy, rigid /flexible nasopharyngoscopy should be performed before a label of “no foreign body” is stamped on the case. 6 However, due to ongoing corona pandemic, diagnostic endoscopies, being aerosol generating procedures were avoided in routine OPD. Hence, to confirm the diagnosis imaging in the form of X-rays and CT was done.
In younger patients, nasal foreign body removal may require experience and great skill. 6 Management of most of the nasal foreign bodies are quite simple. Direct visualization and extraction by using alligator forceps, Eustachian tube catheter, hooks, probes, suction, 6 balloon catheters, glue, 12 and curettes is most common.7,13
Usually in apprehensive patients and cases of complicated nasal foreign bodies such as impacted and encrusted rhinoliths, and so on, sedation is recommended for endoscopic examination and foreign body removal to avoid risk of inhalation or ingestion. 7 Thus, we want to emphasize that most of these cases could have been managed in our OPD if they had presented on time. As initially most of the foreign bodies are visible and are located anteriorly without any nasal discharge or crusting, these could have been removed easily. This is merely one such example of the many more complicated cases that may have presented after lockdown in all the departments. Reduced services and facilities led to delayed diagnosis and management resulting in increased morbidity and mortality in pediatric group. Although with the sudden outbreak of pandemic, lockdown might have seemed to be the essential and only way to tackle it but these strategies have had a significant negative impact on routine health service delivery. Hence, it is very essential to emulate from the evidence-based data from other countries to ensure provision of adequate and timely health care to all patients. This pandemic has shown reality about the existing lacunae in our public health care system. We need to devise standard global policies, protocols, and strategies to fight such unprecedented crisis in future.
Conclusion
This series conducted over a period of 3 months has exposed the lacunae in the present health care facilities. Patients having chronic or nonurgent conditions were affected adversely during this pandemic owing to these deficits in the health facilities, ease of access to the hospital and COVID phobia. We need to formulate and standardize appropriate and clear-cut management strategies to avoid similar unfortunate cases amid a COVID-like crisis so that even the non-COVID cases are managed with equal pathos.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.