
Abstract
The emergency of esophageal button batteries is recognized. Foreign bodies in the ear or nose are treated as comparatively nonemergent. We present the case of a child who presented with suspected pen-nib in the nostril to highlight the importance of investigation and intervention in unwitnessed nasal foreign body and review the literature regarding X-rays in these cases. Fifteen papers were identified as per search parameters; 3 papers recommend the use of plain radiographs for nasal foreign bodies. We propose that in unwitnessed pediatric nasal foreign body insertion, a facial X-ray should be considered, especially if suspecting a metallic foreign body.
Introduction
The urgency of management of esophageal button batteries is well recognized and documented among otolaryngologists and emergency department (ED) doctors. Furthermore, in the United Kingdom, there has been media coverage over the concerns and risks related to children swallowing button batteries, 1 but tragic outcomes still occur 1,2
By comparison, foreign bodies in the ear or nose tend to raise less concern and alarm at first presentation. However, in foreign body impaction in children, the importance of history is negated by the oft unwitnessed access to, and insertion of, foreign body.
We present here a case to highlight the importance of low threshold for investigation and intervention in unwitnessed nasal foreign body and review of the literature specifically related to assessment and management of nonesophageal button battery. The discussion focuses on whether a change in practice to have a lower threshold for facial X-rays in children would be appropriate.
Case Presentation
A 2-year-old boy presented to the ED with a foreign body in his nose. The foreign body insertion was unwitnessed, but the parents noted a pen with a missing nib before bringing him to hospital. Emergency department doctors reportedly visualized a pen nib in the nostril but attempts at removal failed. Emergency department referred the patient to ENT for removal in theater, as the nib had reportedly embedded into the septum and removal attempts were causing bleeding and pain. The patient was nil by mouth waiting for theater until late in the evening. As the emergency list was still busy, the child was allowed to be fed, and theater was planned for the next day.
The initial attempt to remove the foreign body in the anesthetic room was difficult. There was poor visualization due to what was thought to be dried blood and ink debris.
Once debris was cleared in theater, the metallic foreign body was only then recognized as a button battery. There was extensive local damage from local pressure and tissue necrosis and the effect of the electrochemical damage to the mucosa (Figures 1 and 2).
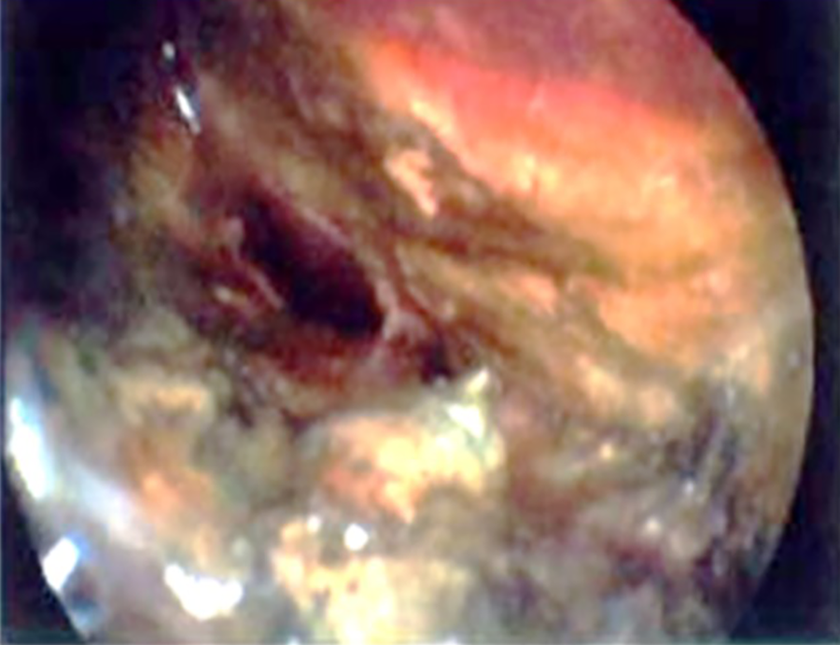
Anterior left septum and lateral wall.
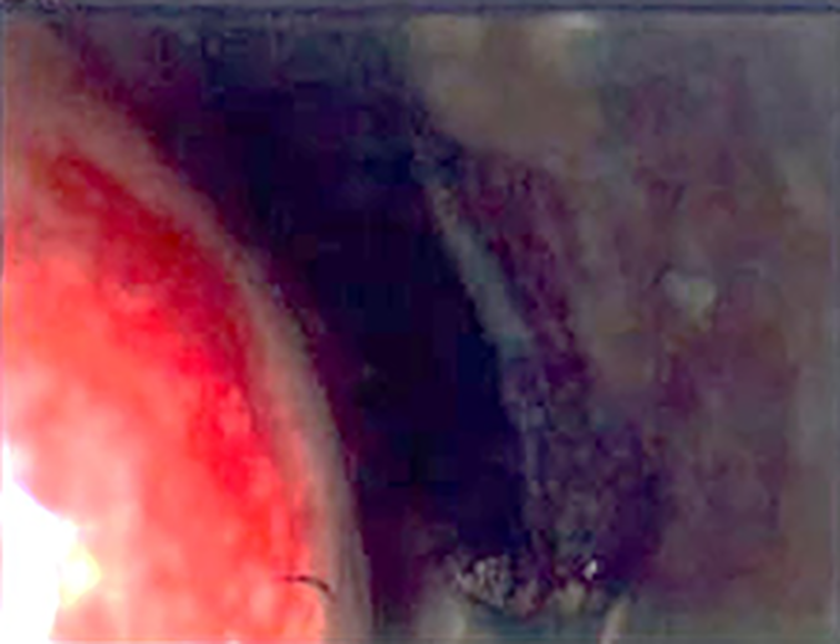
Anterior right septum and inferior turbinate.
After departmental review of the case, one management aspect discussed was the recognized practice of avoiding radiography in young children and infants. However, the classical radiographic appearance of button batteries would have allowed better recognition of the urgency of the case, which was underestimated based on the history of pen nib insertion. A contributing fact to “missing” the battery was due to the history that a pen nib was missing as per the parents’ collateral history, at both the ED and speciality reviews. A plain film X-ray would have shown the metallic foreign body was not a pen nib. In view of this, the literature was searched for any established practice or guidance regarding button batteries in the nose or ear.
Method
A search was completed with support from the Post Graduate Medical Library. Using the MEDLINE database, a search was completed for the terms “Button Battery” OR “Lithium Battery” AND “Ear” or “Nose” NOT “Oesophagus” NOT “TRACHEA.” The search was limited to English language articles related to children in the last 10 years. Other synonyms for “button battery” were included in the search; MeSH terms were used for Nose and Ear.
Results
A total of 15 abstracts were identified. All papers were reviewed, as they met the criteria agreed for inclusion. The criteria set was that any abstract that included a comment on pediatric button battery and included comment on ear or nose foreign bodies should be reviewed.
In the 15 papers reviewed, there were no comments related to aural button batteries. Eight papers directly commented on the use of X-ray in relation to button battery cases (table in Figure 3).
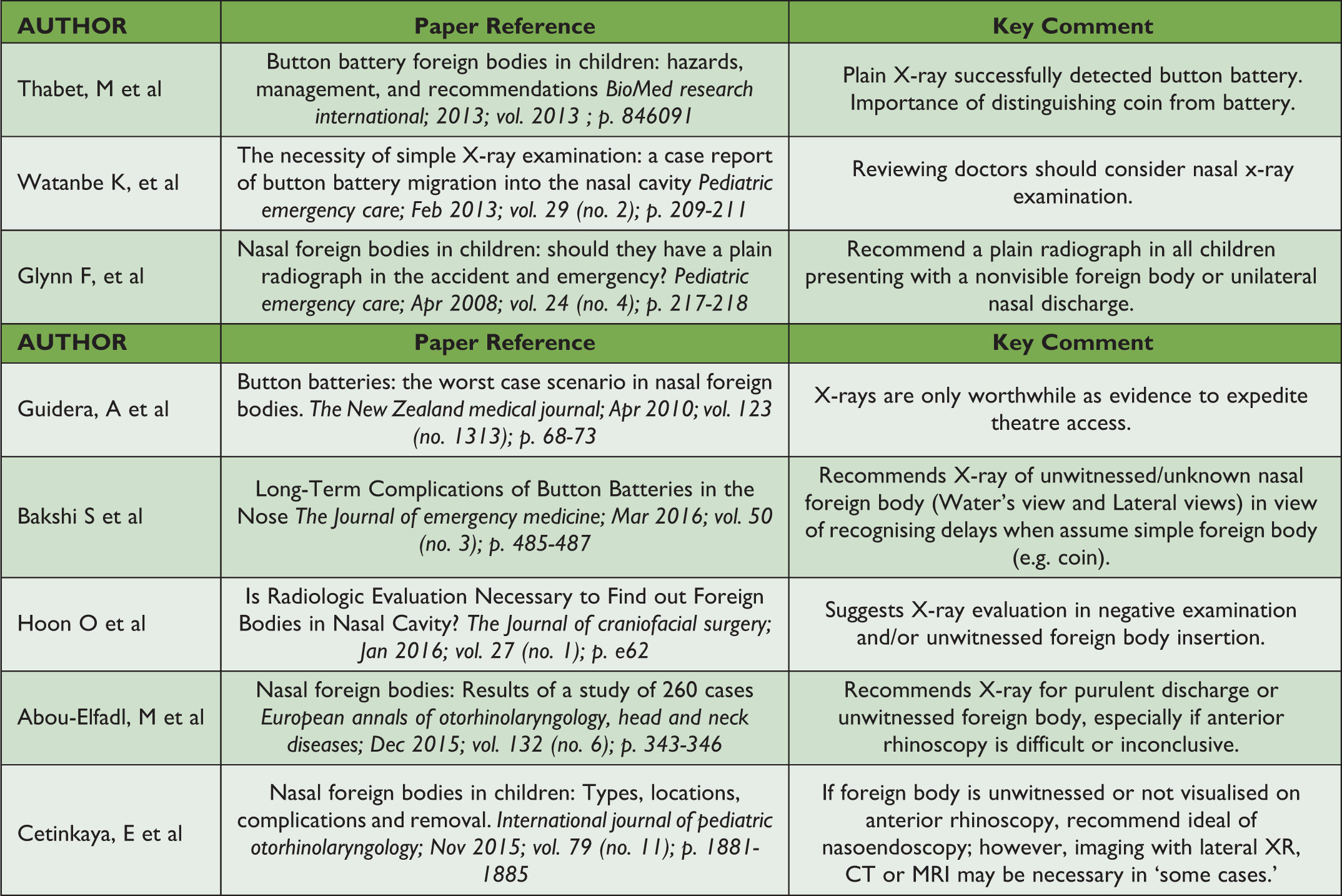
Summary of papers regarding button battery X-rays.
Discussion
The mode of damage of how button batteries cause injury is somewhat complex. There is the mode of “direct pressure” and resultant necrosis from an impacted foreign body. The electric current between the anode and cathode of the battery causes local damage to the mucosa it is in contact with. In addition, when a button battery is in contact with moisture, such as tissue fluid, this results in toxic leakage such as mercuric oxide, sodium potassium hydroxide, and so on. There is evidence that, in simple saline, there is a reaction that results in the release of hydrogen gas and hydrozide ions, both of which cause mucosal erosion. 3
Understanding that there are rapid albeit complex modes of damage from button batteries reinforces the aim of this work to assert the importance of a “low threshold” of suspicion for button batteries in unwitnessed foreign body insertion. Abou-Elfadl et al 4 assert that only 38% of pediatric foreign body insertions occur in the presence of an adult. In another report on foreign bodies presenting to the ED by Glynn et al, 5 3 of 44 foreign bodies were button batteries, unrecognized as such until extraction in theater. These experiences directly reflect the outcome of this case report and reiterate the message that there must be a low threshold for suspecting button battery in unwitnessed foreign body insertion and/or any suspicion of metallic foreign body, especially when the examination findings are disproportionate to or inconsistent with the type of foreign body reported.
Plain film X-ray is a useful and justifiable investigation in these circumstances. It is recognized that radiography in young children and infants is avoided in view of risks associated with childhood exposure to radiation. However, this risk–benefit balance must be assessed for each individual case. A change in practice will lead to more plain film X-rays but may be justified as it is important to intervene appropriately and urgently in those cases where button battery is highly likely on radiographs. The use of plain film X-rays and related exposure may mirror current practices for X-ray for suspected fractures in the equivalent age group. In addition, if the history is worrying enough in ingested foreign bodies, then plain film X-rays are performed regardless of age. This principle should be transferrable to the unwitnessed and disproportionately painful aural or nasal foreign body placement in children. Certainly, it has influenced the authors’ practice, and in April 2020, the author (Acharya) identified a nasal button battery on plain film X-ray and removed it (Figures 4 and 5) before perforation or further damage.

Plain film X-ray of unwitnessed nasal foreign body.

Button battery removed from nose.
Key Conclusions
Urgent removal must occur for button battery insertion regardless of site.
Recognition of button batteries is the key step in achieving this.
Therefore, early plain film X-ray should be justified in: °Unwitnessed foreign body insertions °Suspected unknown metallic foreign bodies °Disproportionate discharge or pain
Footnotes
Authors’ Note
ICJME Form submitted to journal. Consent for use of anonymised patient images for the purpose of educational use was sought.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.