
Abstract
Rhinoliths are petrified masses formed by accumulation of endogenous or exogenous salts around a nidus. Although rarely formed by the body, the most common cause is foreign bodies forgotten in the nose at childhood. Rhinoliths are rare and have been reported as a single case report in the literature. In this study, 24 different and different cases will be analyzed. Twenty-four interesting patients who were operated for rhinolith in the otorhinolaryngology clinic between 2014 and 2019 and were not seen in the literature before were analyzed retrospectively. The characteristics of these patients such as age, sex, additional pathology, foreign body coexistence, type of anesthesia used, and previous surgical status were analyzed. Fourteen patients were male and 10 were female (58.3% male, 41.7% female). The mean age was 30.4 (minimum 2, maximum 62). Twelve of the foreign bodies were on the right and 12 on the left (50%). Foreign body localization was 13 (54.1%) between the inferior turbinate (IT) and septum and 11 (45.9%) between the middle turbinate and septum. Tissue destruction was seen in 12 (50%; 7 septum, 5 IT) patients. Fifteen patients had additional pathology (mostly septum deviation). General anesthesia was used in 14 patients and local anesthesia was used in 10 (58.3%-41.7%) patients. Two patients (n = 2) had rhinoliths due to forgotten nasal packing after surgery and forgotten silicone nasolacrimal tube after dacryocystorhinostomy surgery. Rhinoliths should be considered with unilateral malodorous runny nose and resistant sinusitis attacks. The diagnosis is rigid endoscope and computed tomography imaging. It usually occurs as a result of forgotten foreign bodies. Rhinoliths may also form as a result of forgotten tampon after previous nose or eye surgery.
Introduction
Rhinoliths are calcified masses formed around a nucleus. Although they occur in all age groups, they peak in childhood and adolescent age groups. This core may be endogenous or exogenous. Endogenous ones may be part of the nasal mucus, blood clot, and epithelium. Exogenous ones are formed by calcification around the forgotten foreign bodies in childhood. Clinically, it is seen as headache, nasal congestion, or unilateral malodorous runny nose that does not persist despite treatment. Rhinoliths are detected during endoscopic examination, gray-brown color. When touched, they can cause severe headache and dizziness, so it may be difficult to remove with local anesthesia. They usually remain locally, sometimes destroying the surrounding turbinate and septum, causing a chemical reaction with the tissue. 1 The capsules consist of crystals of calcium carbonate, calcium phosphate, or magnesium carbonate. They are usually formed by petrification of foreign bodies entering the nose in childhood. After the first case of Bartholin in 1654, approximately 1000 rhinoliths between 6 months and 84 years have been reported. 2
In our study, 24 foreign body origin rhinolith cases, including forgotten surgical material, will be discussed. Clinical features of these patients, additional pathologies, foreign body types, imaging, forms of anesthesia used, additional surgical intervention, and so on will be explained.
Materials and Methods
In this study, 24 interesting patients, aged 2 to 62 years, who were operated for rhinolith in otorhinolaryngology clinic between 2014 and 2019, and not seen in the literature before, were analyzed retrospectively. Written informed consent was obtained from all of these patients. Age, sex, additional pathology, association of foreign body, type of anesthesia used were analyzed. Age, sex, foreign body side and foreign body shape, septum deviation, presence of additional sinus pathology, local tissue destruction, type of anesthesia used, and additional surgical intervention of these patients were analyzed. Examination was performed with 0 rigid endoscope, and computed tomography (CT) imaging was performed in adult patients. Local or general anesthesia was used according to rhinolith size and patient tolerance.
Results
Fourteen patients were male and 10 were female (58.3% male, 41.7% female). The mean age was 30.4 (minimum 2, maximum 62). All of the patients were diagnosed with the help of 0 endoscope using locally impregnated cottons. Computed tomography imaging was performed for localization of foreign body and local tissue involvement. Twelve of the foreign bodies were on the right and 12 (50%) on the left. Foreign body localization was 13 between the inferior turbinate (IT) and septum (54.1%) and 11 (45.9%) between the middle turbinate and septum. Tissue destruction was seen in 12 (50%; 7 septum, 5 IT) patients. Fifteen (8 patients had septum deviation, 3 patients had adenoid vegetation, 4 patients had nasal polyposis) patients had additional pathology. Septoplasty was performed in 8 patients, adenoidectomy in 3 patients, and FESC operation in 4 patients. General anesthesia was used in 14 patients and local anesthesia was used in 10 (58.3%-41.7%) patients (Table 1).
Demographic and surgical features of rhinoliths
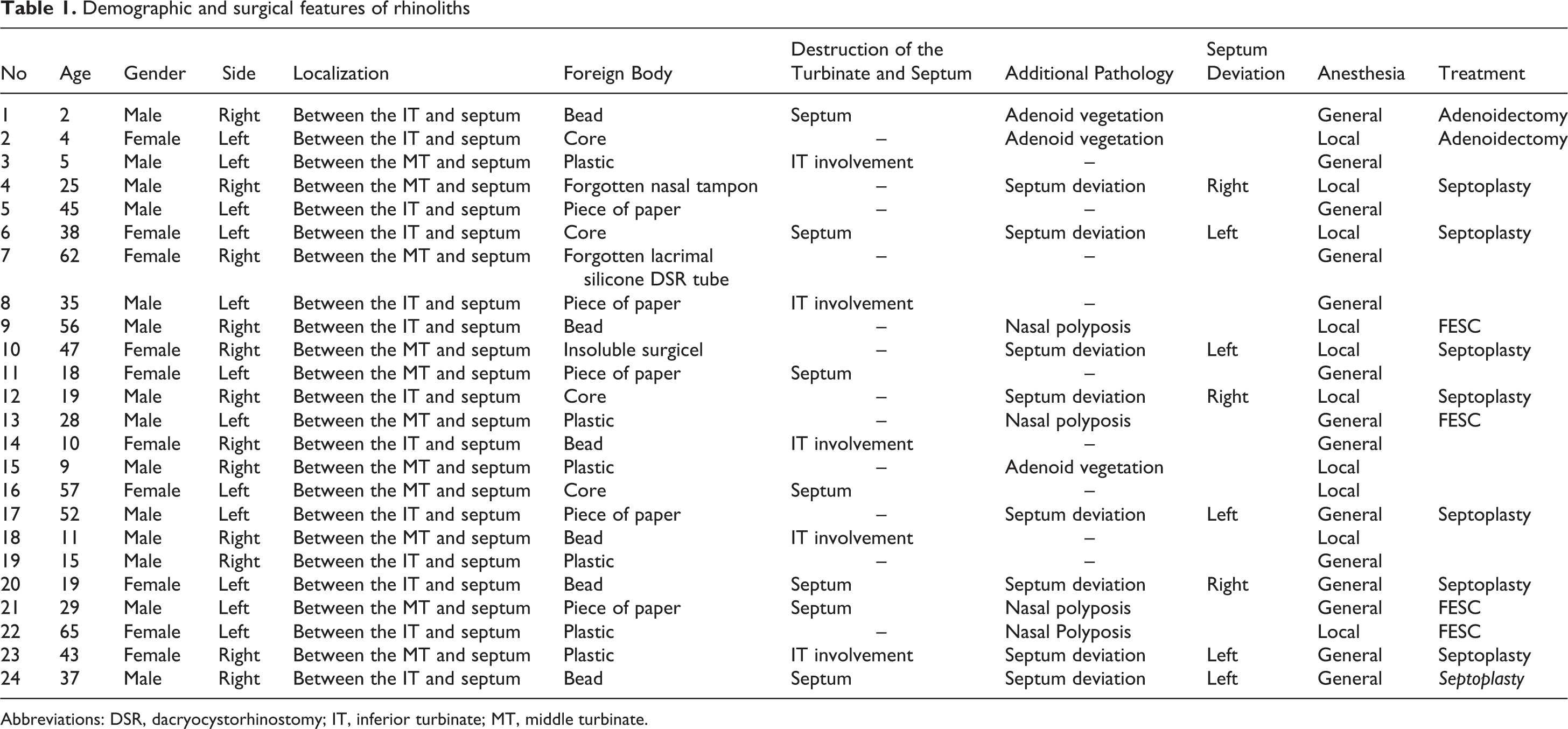
Abbreviations: DSR, dacryocystorhinostomy; IT, inferior turbinate; MT, middle turbinate.
Two patients (n = 2) had rhinoliths due to forgotten nasal packing after surgery and forgotten silicone nasolacrimal tube after dacryocystorhinostomy surgery. The first patient was a patient who had septoplasty at the external center 1.5 years ago and forgot to take a tampon, and the other was a 62-year-old patient who had undergone dacryocystorhinostomy due to lacrimal canal occlusion 20 years ago (Figure 1). Foreign bodies can make tissue destruction (Figure 2).

Rhinoliths due to forgotten tube after dacryocystorhinostomy surgery.
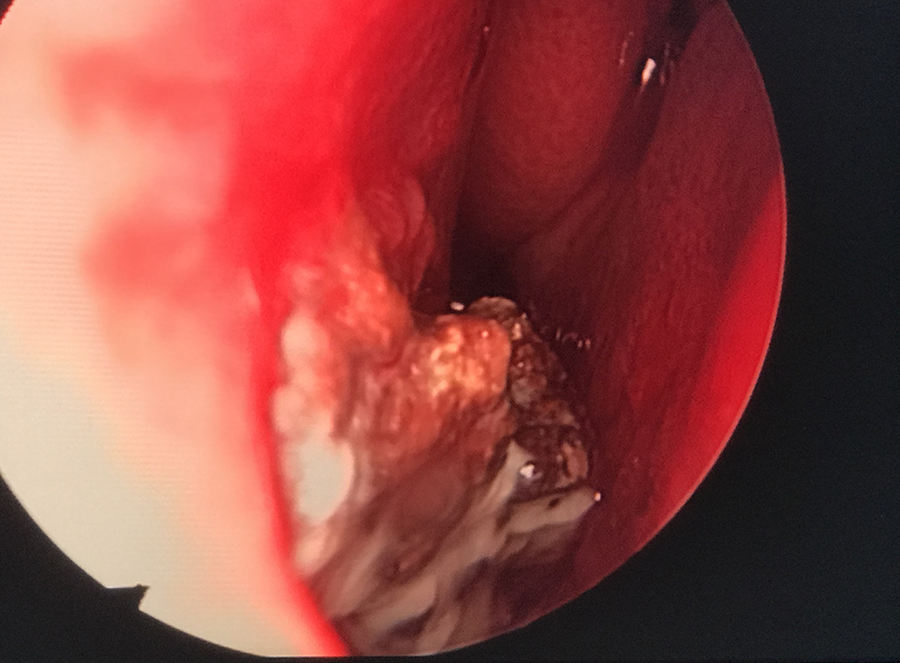
Rhinoliths destroying lower turbinate.
Discussion
The etiology of rhinoliths is controversial. They usually occur by encapsulating mineral salts around a nidus. They may accumulate around an endogenous nidus due to nasal discharge, bleeding, or epithelial debris caused by chronic inflammation. However, most of them are formed by accumulations around foreign bodies entering the nasal cavity from childhood. 3
All cases in our study were caused by foreign bodies. These bodies are usually foreign bodies such as plastic and nuclei. 1,4 Two specific cases were due to the forgotten tampon after previous eye and nose surgery, which has not been previously reported in the literature. The first of these patients was due to forgotten Doyle nasal splint due to previous septoplasty. The other was developed as a result of failure to remove the silicone nasolacrimal tube placed after nasolacrimal duct obstruction surgery 20 years ago (Figure 1) In the literature, no postnasal tamponade rhinolithiasis has been reported.
Unilateral nasal obstruction is the most common clinical finding of patients with rhinolith. The most edematous diagnostic finding of these patients is malodorous and unilateral nasal discharge. It is often confused with the diagnosis of allergic rhinitis and sinusitis. 5 In addition, headache, facial pain, epistaxis, cough, and sneezing may be seen. 6 The most frequent complaints of our patients were runny nose and nasal obstruction.
Rhinoliths are detected during endoscopic examination, gray-brown color. Rigid or flexible endoscopy can be used. 7 Computed tomography is the gold standard for diagnosis, since these are usually radiopaque. Therefore, it can be confused with structures such as nasal osteoma, fibroma, hemangioma, and osteosarcoma. In our cases, we used it only to identify additional pathology in adult patients and to show tissue overalls. Septum deviation may be associated with additional sinonasal pathologies such as nasal polyposis. Touching them may cause severe headache and dizziness. Clinically, they are seen as sinusitis and vestibulitis that do not pass despite treatment. Therefore, it may be difficult to remove with local anesthesia. They are usually removed with general anesthesia. Direct pediatric anesthesia should be used regardless of size. General anesthesia was used in most of our cases. Thus, surgical interventions such as septoplasty, septorhinoplasty, adenoidectomy, or FESC can be performed together. 8
The most common site of rhinoliths is between the IT and the septum. They may also originate from the nasopharynx. They may cause local reactions in the tissue in which they are located. They usually remain locally, sometimes destroying the surrounding turbinate and septum, causing a chemical reaction with the tissue. Complications such as Marjolin ulcer, squamous cell carcinoma, naso-oral fistula, and palatal perforation have been reported due to local irritation and destruction. 9 A significant proportion of our cases had septum and lower turbinate destruction.
Conclusion
Rhinoliths should be considered with unilateral malodorous nasal discharge and attacks of resistant sinusitis. The diagnosis is rigid endoscope and CT imaging. It usually occurs as a result of forgotten foreign bodies. Previously reported cases include cores, plastics, and so on. No nasal tamponade has been reported. Based on our cases, rhinoliths may be formed as a result of forgotten tampon after previous nose or eye surgery.
Footnotes
Authors’ Note
Consent was obtained from the families of the patients. Ethics committee approval was obtained.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.