
Abstract
Penetrating traumas of the head are generally life-threatening injuries, whose management poses a substantial challenge for emergency department teams. These injuries are characteristically violence-associated and frequently accompanied by damage of essential organs including brain, meninges, large vessels, cranial nerves, eyes, viscerocranium, internal ear, and/or labyrinth. Here, we present an exceptional case of head trauma caused by a knife blade, which was stuck deep inside in the petrous bone. After the extraction of the knife, the patient had very few immediate and no long-term post-traumatic complications. In conclusion, high-end technical equipment as well as an interdisciplinary team of specialized physicians is recommended for the management of penetrating head trauma to optimize the outcome.
Introduction
Head traumas by thrusting weapons such as knifes are characteristically violence associated.1,2 Their severity is determined by a variety of factors such as penetration site, depth of penetration, or type of the penetrating object. Generally, these injures are life-threatening as they are frequently accompanied by damage of essential organs including brain, meninges, large vessels, cranial nerves, eyes, viscerocranium, internal ear, and/or labyrinth.1-4 Due to the high risk of vital complications and the relative scarcity of such traumas, their management poses a substantial challenge even for emergency department teams of tertiary care hospitals. Nevertheless, only few case reports are available describing the management of similar traumatic head injuries. Particularly, to the best of our knowledge, there is no publication discussing the case of a knife stuck in the petrosal bone and its management in a tertiary care hospital.
Case Report
A 47-year-old male patient was assaulted by an unfamiliar person during an argument in public, who stabbed a knife in his head. Preclinically, the patient intravenously received fentanyl, norepinephrine, and propofol. On admission to the emergency department of our tertiary care university hospital, the knife was stuck in the skull approximately 2 cm above and behind the left ear with only few centimeters of the residual blade being visible and moderate local bleeding (Figure 1). After turning off the propofol infusion, the patient was awake, alert, and oriented to person, place, time, and events, with a Glasgow Coma Scale score of 15/15. His vital signs were stable and the neurological examination revealed no deficits including facial nerve function.
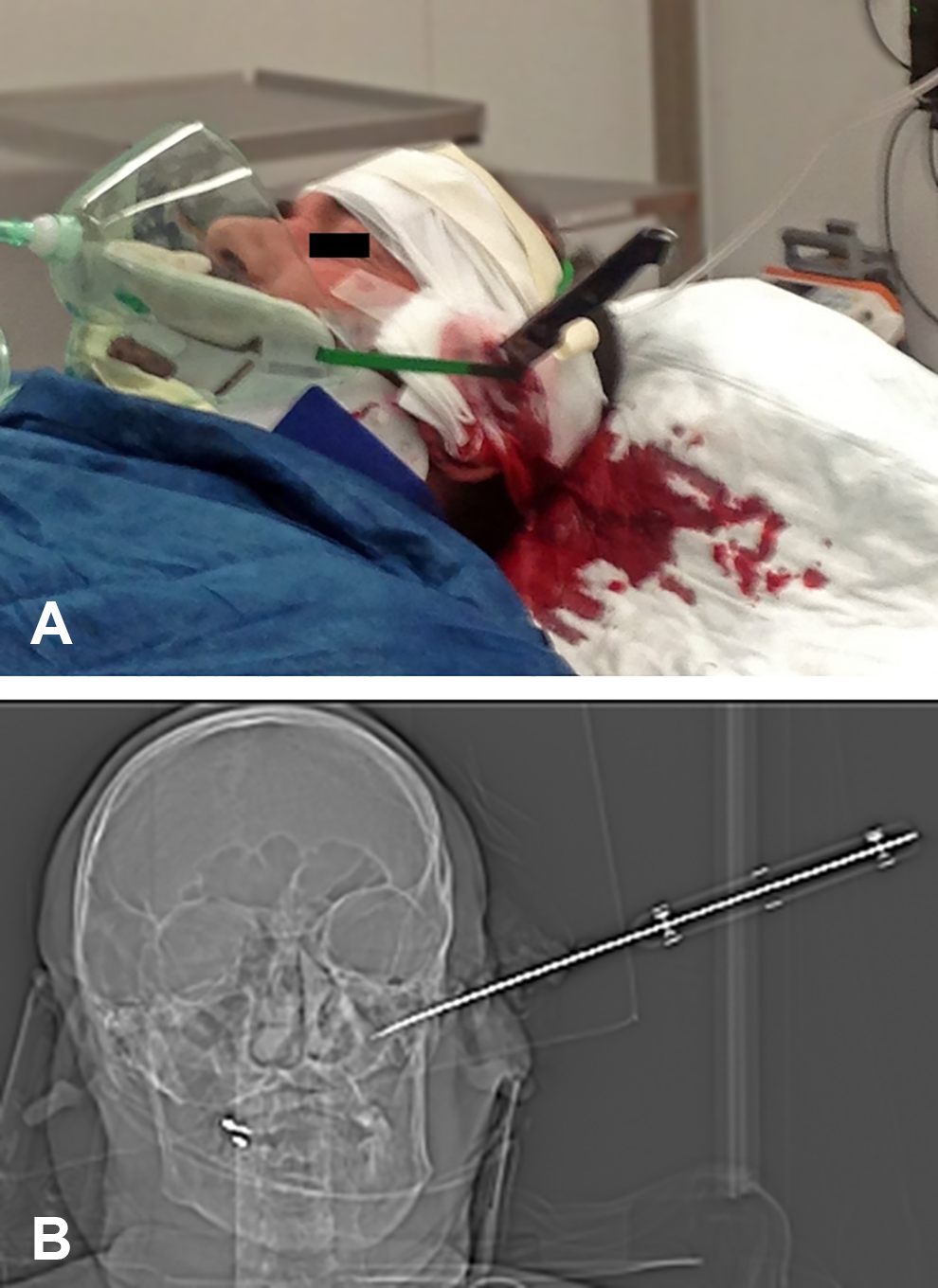
Status upon admission to the emergency department. Side view of the patient with the knife in situ (A). Reformatted computed tomography (CT) image illustrating intrusion direction and depth of the penetrating knife in the left petrosal bone region (B).
Following the first examination, he was anesthetized, intubated, and ventilated before a computed tomography (CT) scan of the skull was conducted. The CT scan (Figure 2) revealed the precise localization of the knife: It entered the skull behind the ear, penetrated the petrous bone, and intersected the middle ear, whereas the very tip of the blade was located in the sinus sigmoideus without perforating the inner layer of the dura mater (Figure 2). Cerebral angiography indicated no acute bleeding of the sinus sigmoideus, while the blood flow around the tip of the knife was reduced.
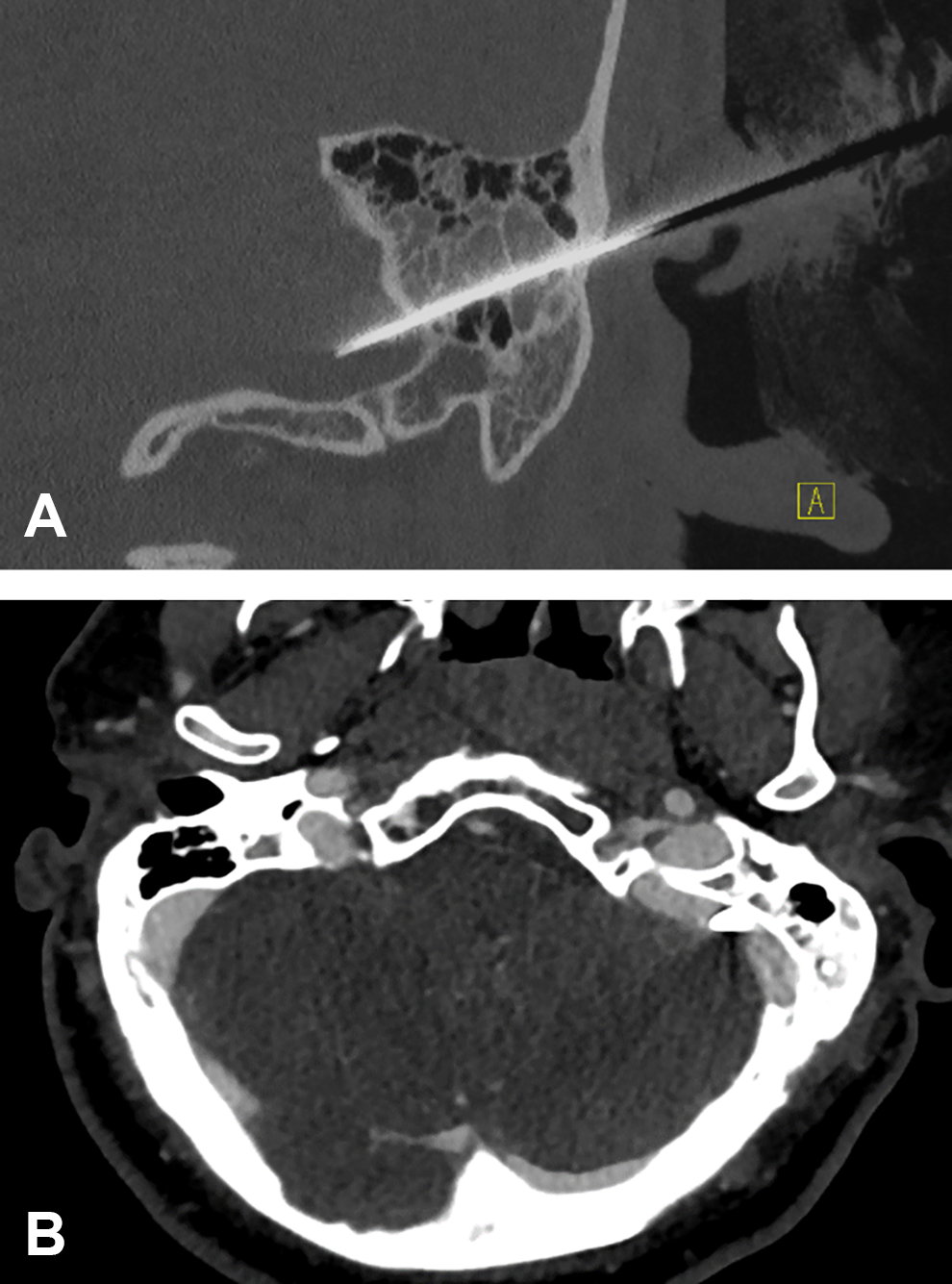
Status upon admission to the emergency department. Coronal reformatted computed tomography (CT) image of the left petrosal bone (A, native imaging; bone window) and axial reformatted image (B, venous phase; soft tissue window) illustrating the penetration of the left petrosal bone by a knife after stab injury. The tip of the knife (arrow) is located within the sigmoid sinus (B, *). Additional finding: Partial occlusion of the left mastoid cells with hemorrhage fluid.
The interdisciplinary team of radiologists, anesthesiologists, neurosurgeons, and otorhinolaryngologists–head and neck surgeons discussed possible treatment options including the management of potential complications considering the location of the knife. Finally, it was decided to cautiously remove the knife under CT scan monitoring with surgical standby in case of complications. During the process of evaluation and decision-making, it was particularly emphasized not to lever the knife during removal despite the compact and solid structure of the petrous bone as a perforation of the sigmoid sinus should be avoided strictly.
After several removal attempts had failed, 2 persons together were finally able to remove the knife using a large forceps as cross guard while pulling smoothly on both sides. Two follow-up CT scans with angiography, immediately and 30 minutes after intervention, did neither reveal an acute intracerebral bleeding nor a cerebrospinal fluid fistula. Hemostasis in the superficial wound area was achieved by bipolar electrocoagulation. Subsequently, the 2.5 cm wound was sutured and the patient admitted to the intensive care unit for observation and antibiotic treatment.
The following days, CT and magnetic resonance imaging (MRI) scans were conducted to check for intracerebral bleeding, ischemia, tissue injury, or thrombosis. The CT scan revealed a filling defect of the sinus sigmoideus and the MRI validated a post-traumatic partial thrombosis of the sinus sigmoideus (Figure 3).
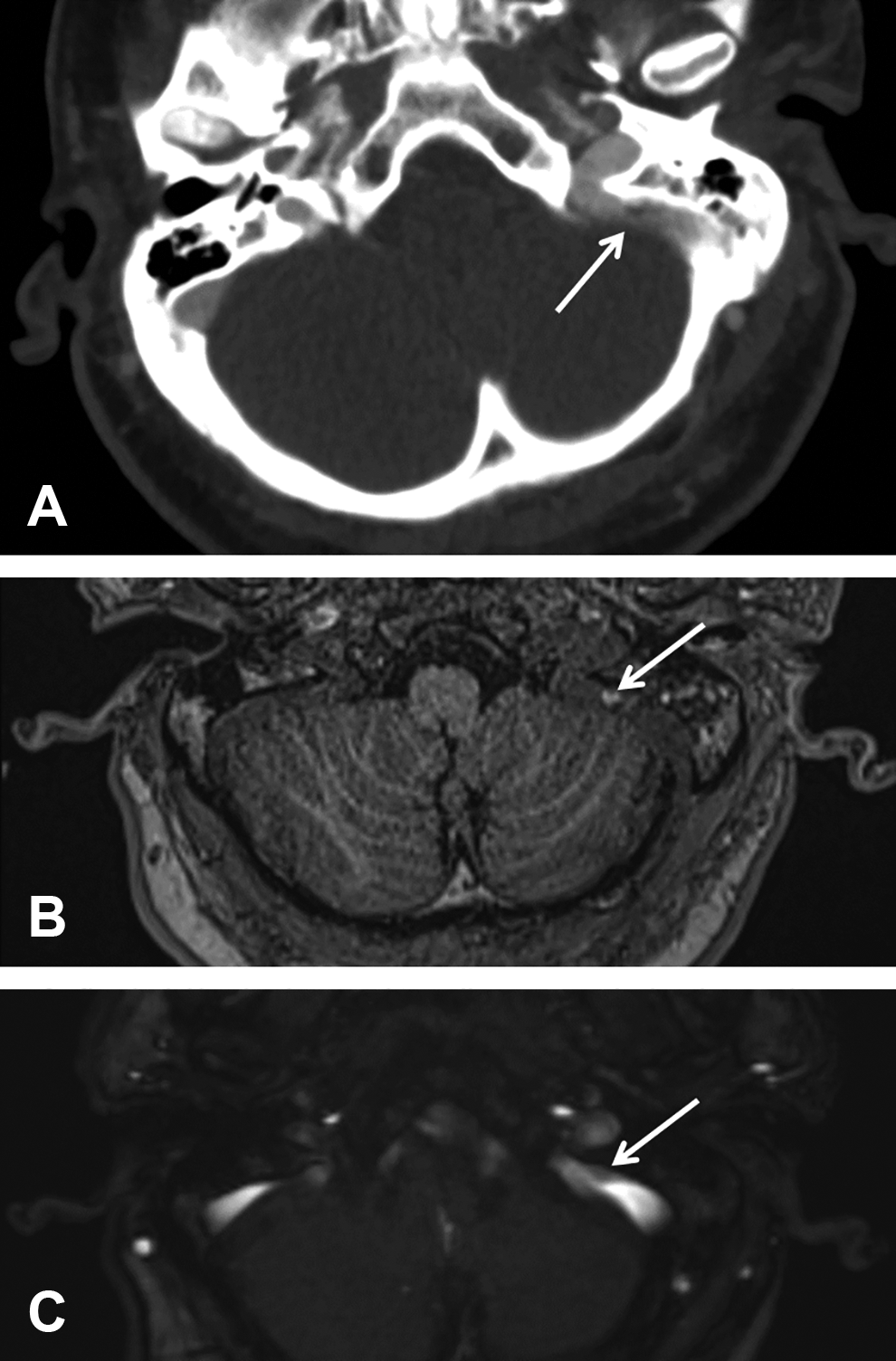
Status after removal of the knife. Axial formatted computed tomography (CT) image (venous phase; soft tissue window) with focal, hypodense filling defect in the left sigmoid sinus: Suspicious for post-traumatic partial sinus thrombosis (A). Supplementary magnetic resonance imaging (MRI) imaging confirmed partial sinus thrombosis of the left sigmoid sinus with a T1W-hyperintense thrombus (arrow in B, axial fat-saturated T1 weighting) as well as a filling defect in the venous time-of-flight (TOF) angiography (arrow in C).
The further postoperative course in the clinic was uneventful. No neurological deficit was detectible in clinical examinations and the wound did not show signs of irritation or infection. As expected, audiometry indicated conductive hearing loss due to a hemotympanum (Figure 4). The patient was discharged to ambulatory care after 10 days. The 1-month follow-up examination confirmed a neurological status without pathological findings, the wound healed well, and after complete resorption of the injury, the patient ended up with nothing more but a scar in the temporal area.
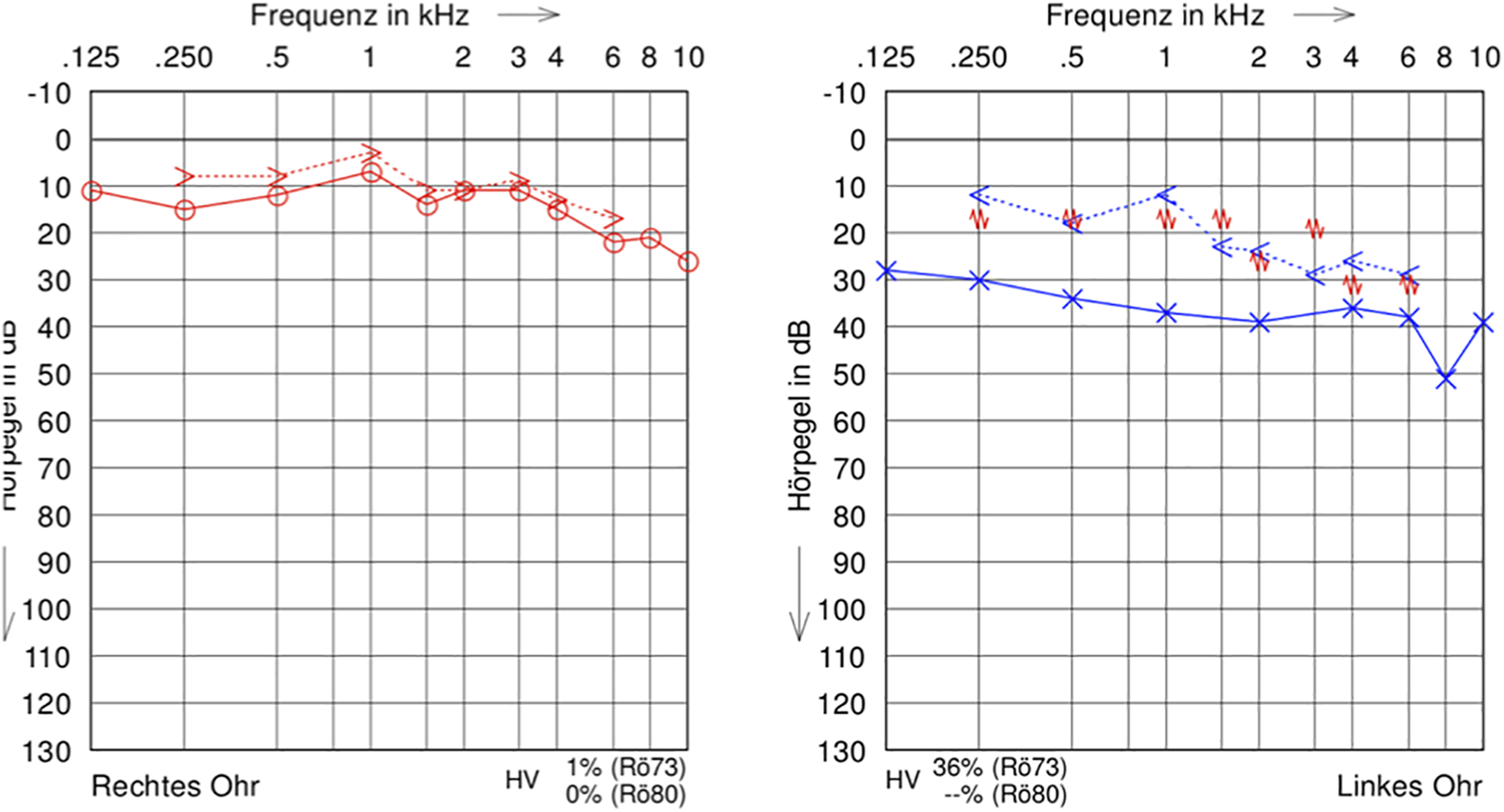
Audiogram after removal of the knife. Conductive hearing loss on the left due to hemotympanum.
Discussion
Head injuries and particularly brain stab wounds implicate vital complications such as intracranial hemorrhage, injury of essential vessels, local or systemic infection, dramatic neurological deficits, and loss of critical systems including the visual, auditory, vestibular, and olfactory system. The likelihood for different complications and the clinical outcome is determined by a variety of factors such as penetration site, depth of penetration, or type of the penetrating object.1-4 Accordingly, the management of penetrating head injuries depends on these aspects. Therefore, the first step is airway maintenance and hemodynamic stabilization of the patient.3,5,6 Subsequently, it is mandatory to assess the type of penetrating object, the penetration site, penetration depth, as well as the affected and endangered structures.3,6,7 High-resolution CT is essential to exactly analyze the location of the object for planning the removal as well as to conduct follow-up scans of the head to be able to plan the management in case of complications. Besides, the preoperative cerebral angiography helps to identify damages of the vascular system. Unavailability of these radiologic imaging methods might result in avoidable secondary brain injury.6-11
As soon as these information have been collected, the removal of the object should be planned accurately to anticipate potential peri- or postinterventional complications. 6 Extractions of penetrating objects should then be performed carefully with minimal additional damage. Penetrating objects in the petrous bone require special attention. First, the petrous bone is the hardest bone in the body, which implies that penetrating objects are fixed firmly in this bone and demand a great force to extract it. 12 Secondly, the petrous bone incases various essential organs and structures such as the inner ear, the labyrinth, the facial nerve, or the carotid artery. Moreover, several critical structures including brain, brain stem, cranial nerves, and big vessels are located in close proximity to the petrous bone implying the potential hazard of these injuries.4,11,13
The major principle is not to attempt to remove the knife before a careful investigation has been performed, and the interdisciplinary team is prepared to remove the instrument with an appropriate plan. 5 Removal of the penetrating object should retrace the original trajectory of the knife. During extraction, care must be taken not to produce any rocking movements which may be transmitted to the tip of the knife.1,3
An interdisciplinary approach for management and treatment of penetrating head trauma is recommended by most authors. However, the appropriate methods of extraction are controversially discussed in the literature.1-3,5,6,11,14,15 Options to remove the object are either by simple withdrawal or by a surgical approach such as mastoidectomy. Grobbelaar and Knottenbelt described 11 cases, in which no patient had abnormal bleeding or any other relevant complication related to simple withdrawal. 14 In contrast, Gluncić et al suggested that a blade should be removed through an interdisciplinary team of otorhinolaryngologists–head and neck surgeons, maxillofacial surgeons, neurosurgeons by a surgical approach performing mastoidectomy, even if there are no signs of vascular injury. The authors promote this approach since a retained knife blade might temporarily tamponade an incised vessel, and hence, removal could subsequently lead to serious hemorrhage. In this context, surgical exposure of the penetrating object as well as the affected vessel would allow immediate surgical management of complications associated with removal of the object. However, in their case, the knife was also impossible to remove by pulling forces when admitted to the hospital emergency unit. 2 Generally, a surgical approach is mandatory, if the brain is affected.1,11,15
As neither endocranial nor inner or middle ear structures were critically affected in our case and imaging revealed only a minimal intrusion into the sinus sigmoideus we decided to withdraw the knife carefully. A CT angiography recorded immediately after the intervention showed no bleeding of the sinus sigmoideus after knife removal.
Reviewing the literature on comparable injuries described to date revealed that no general appropriate algorithm has been published for the management of such injuries. Hence, their management requires an individual approach for each case. This might be highly effective and associated with minimal collateral damage only through multidisciplinary teamwork of neuroradiologists, otorhinolaryngologists–head and neck surgeons or maxillofacial surgeons, and neurosurgeons. To optimize the outcome, interdisciplinary management in a clinic providing maximal medical care would be ideal for treatment of penetrating injuries of the petrous bone. Finally, cautious postoperative care reduces secondary complications such as bleeding or infections. In this context, angiography is essential not only in the acute situation to exclude bleeding complications of arteries or the sigmoid sinus but also secondary for detection of post-traumatic thrombosis of the sigmoid sinus, a dural arteriovenous fistula, or traumatic aneurysms which may appear months to years after the trauma.
Conclusions
Despite being rare events, penetrating head injuries are severe threats to the patient’s health, which require high-end technical equipment as well as an interdisciplinary team of specialized physicians to be able to provide an optimal treatment. In particular, it is mandatory to meticulously plan the management of such traumas to avoid unnecessary complications by the injury itself as well as by removal of the object.
Footnotes
Acknowledgments
The authors thank our colleague Christoph A. Reichel for critically reviewing the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.