
Abstract
Objective:
Congenital anomalies of the external ear may present a reconstructive challenge, particularly when normal chondrocutaneous components of the auricle fail to develop. Our goal was to develop a novel technique for lobule reconstruction of a congenitally absent earlobe with photographic documentation of the technique.
Methods:
Informed consent for perioperative photography and publication of case details was obtained. A postauricular, turnover flap with ipsilateral conchal cartilage grafting was performed to reconstruct the lobule, and a superiorly based, postauricular, rotation advancement flap was used to close the donor site defect.
Results:
Perioperative photographs are included demonstrating technique and cosmetic results.
Conclusions:
Malformations rarely involve the lobule or lower third of the ear primarily. Literature regarding lobule reconstruction for congenital malformations is scarce. We present a novel technique for lobule reconstruction of a congenitally absent earlobe performed in a single stage that avoids a visible neck scar and allows for simultaneous conchal cartilage harvest. The technique demonstrated satisfactory cosmesis regarding contour and overall appearance and these results remained stable at 1-year follow up.
Introduction
Congenital abnormalities of the auricle are significantly varied in appearance and severity, and numerous descriptive terms and classifications have been proposed.1-3 Auricular anomalies can be broadly classified as either deformational (anomalies resulting from abnormal forces on the external ear during development) or malformational (anomalies resulting from errors in embryogenesis between the fifth and ninth week of gestation). Deformations generally have all chondrocutaneous components of the auricle intact and can often be treated with ear molding alone if initiated early.3,4 Conversely, auricular malformations result in deficiencies in skin or cartilage and generally require surgical correction with local skin flaps and/or cartilage grafting to reconstitute a normal appearance.
Both categories of auricular abnormalities most commonly and most significantly cause aberrations in the structure of the superior helix. 2 Congenital anomalies of the lobule are less commonly described and are often characterized in the context of congenital earlobe cleft, although the literature is sparse.5,6 In their classification of earlobe clefts, Kitayama et al include a fourth group for “defective lobe” or complete absence of the lobule; however, as discussed previously, congenital anomalies are varied and may present with multiple auricular abnormalities. 5 Complete absence of the lobule is rare, particularly when other auricular components are fully or partially developed, and techniques regarding lobule reconstruction for congenital deformity are lacking. Reconstructive techniques are mainly described for management of traumatic deformity or oncologic resection. The most popular techniques for earlobe reconstruction require local tissue transfer from neck skin, including modified bilobed (Gavello technique) and Limberg flaps.7-9 Nonanatomic cartilage grafts, including use of donor septal cartilage in a 2-stage approach, have been proposed for prevention of contracture and maintenance of shape in the reconstructed lobule. 10 However, these commonly utilized flap techniques necessitate a visible neck scar and a second surgical site if cartilage harvest is planned. In the present article, we describe a rare case of a congenitally absent lobule reconstructed with a novel, postauricular turnover flap with conchal cartilage grafting and a postauricular rotation advancement flap for closure of the donor site defect.
Case Presentation
Written, informed consent for perioperative photography and publication of case details was obtained. The patient was a 9-year-old male presenting with right-sided aural atresia, conductive hearing loss, preauricular skin tag and pits, and congenital auricular malformation with a complete lobule deficiency. A computed tomography scan ruled out signs of cholesteatoma and demonstrated only mild dysplasia of the incudomalleolar complex correlating with his hearing loss, for which he was satisfied managing solely with aided-hearing. However, he was particularly bothered by the appearance of his auricle, and he and his family sought reconstructive options. His right external ear demonstrated mild helical lidding, his triangular fossa was missing due to a lack of superior antihelical crus, the total size of the helix was mildly smaller compared to the contralateral side, and his lobule was completely absent (Figure 1A). His cartilaginous antitragus, incisura intertragica, and caudal helix were intact at inferior extent of the auricle, but no soft tissue lobule was present. The patient was bothered only with the inferior third of the auricle and requested reconstruction of only the lobule and removal of his preauricular tag. A postauricular turnover flap with ipsilateral conchal cartilage grafting was performed to reconstruct the lobule and a superiorly based, postauricular rotation advancement flap was used to close the donor site defect. His 1-year postoperative result is shown in Figure 1B and C.
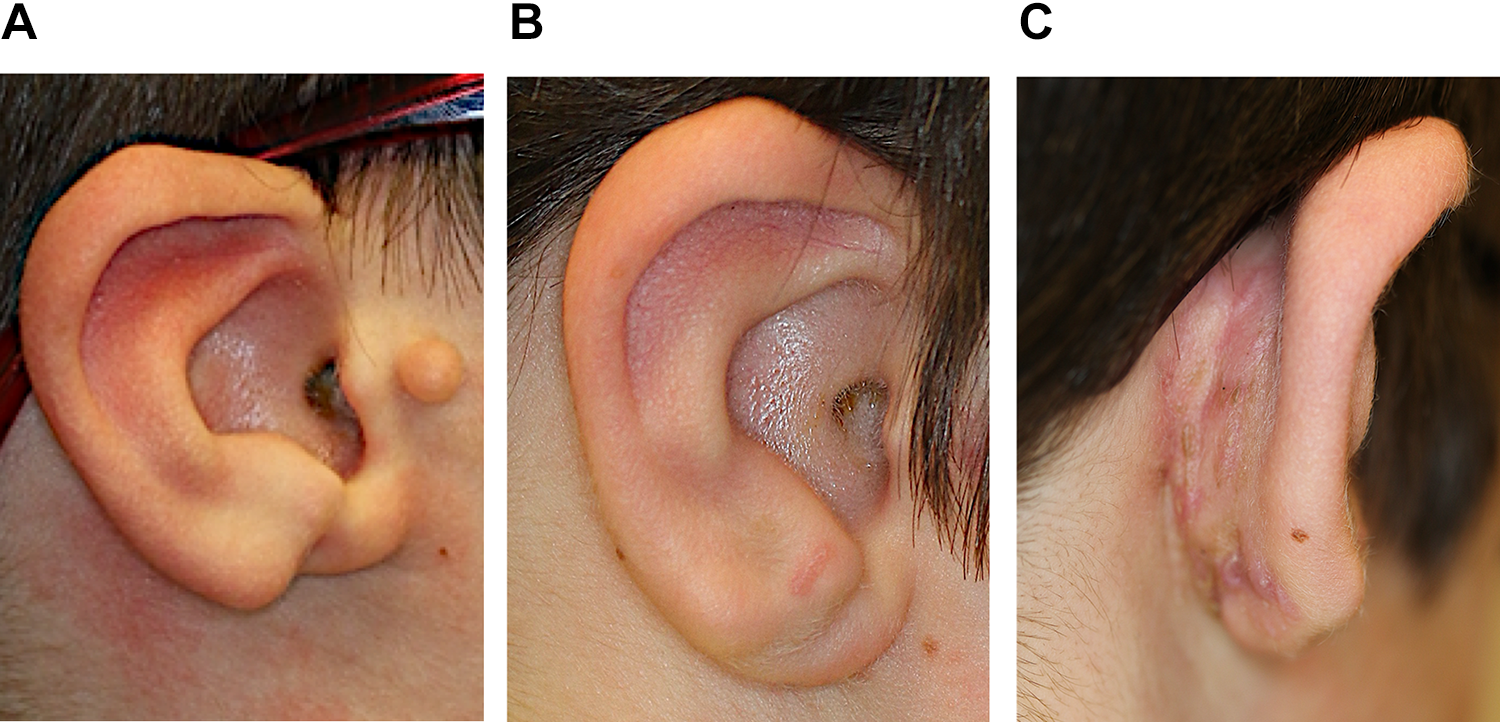
Preoperative image of auricle with congenitally absent lobule (A). One-year postoperative image following lobule reconstruction (B). All surgical scars concealed on the posterior auricle (C).
Procedure in Detail
A template of the contralateral auricle was fashioned for surgical planning. As shown in Figure 2A, postauricular turnover flap was designed to reconstitute the lobule and a postauricular rotation advancement flap and a mastoid advancement flap were designed for closure of the secondary defects. A conchal cartilage graft for framework stabilization was also planned from the ipsilateral ear. A 50:50 mixture of 1% lidocaine with 1:100 000 epinephrine and 0.25% Marcaine was injected. The preauricular skin tag was excised. We then made all of our flap incisions and flaps were elevated in the supraperichondrial plane. After the posterior conchal bowl was exposed with flap elevation, a 2.1 × 1.1 cm piece of conchal bowl cartilage was harvested based on our template from the ipsilateral ear. The conchal cartilage graft was secured superiorly to the existing auricular cartilaginous framework and inferiorly to deep tissue with 4-0 polydioxanone II suture (Figure 2B). The turnover flap was folded over the inferior edge of this cartilage graft and sutured in place with 5-0 poliglecaprone suture. The superiorly based postauricular flap was rotated and advanced inferiorly and then the mastoid skin flap was advanced anteriorly to close the donor sites with 5-0 poliglecaprone suture (Figure 2C). A chromic quilting suture was performed to the postauricular and turnover flaps to further stabilize the framework. Figure 2D demonstrates the final appearance of the closure directly following the procedure.
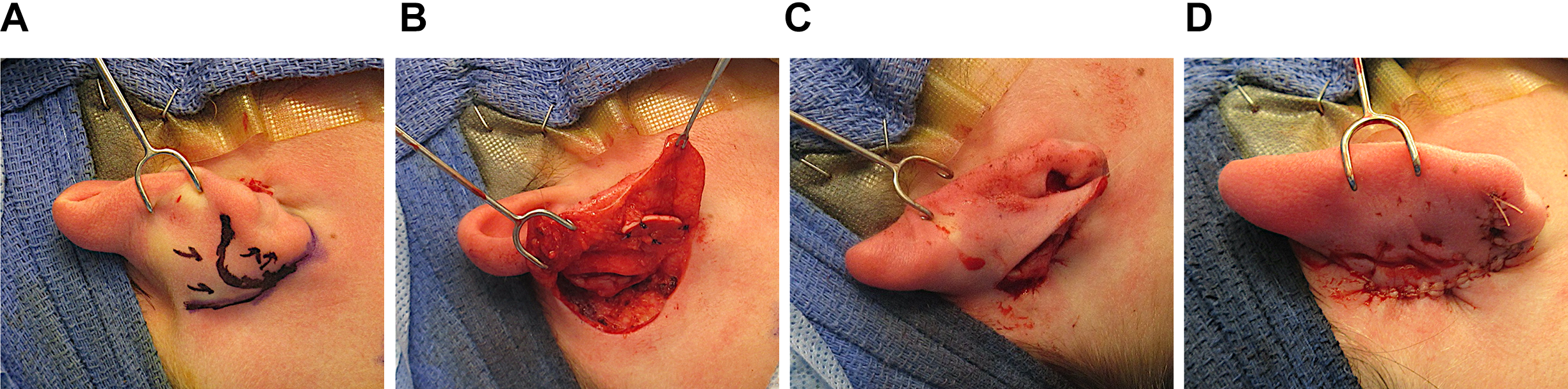
Intraoperative photographs detailing the procedure. Design of postauricular turnover and rotational advancement flaps (A). Cartilage harvested from the concha is secured to the inferior auricular cartilage to create a lobule framework (B). Postauricular flaps secured to cover cartilage and close the donor site (C). Final appearance of the closure (D).
Discussion
The present article describes a rare case of congenital absence of the earlobe and a novel technique for lobule reconstruction. The benefit of this technique is that it can be performed as a single-stage procedure while allowing for cartilage harvest from the same surgical site. Furthermore, all visible scars are concealed on the posterior surface of the auricle. The postoperative result was cosmetically satisfactory at the 1-year postoperative follow-up, and there were no complications.
Our technique is unique both in the context of congenital deformity and for earlobe reconstruction overall and potentially could be applied to other etiologies, although it is ideal in the setting of a congenitally absent lobule. The advantage in the application of this procedure to a congenital deficiency is the continuity of the skin bridge from anterior to posterior allows the turnover flap to be easily rolled forward. In the setting of acute trauma or oncologic resection, there would be an absence of an intact skin bridge until healing was complete, and scar or interrupted vascular supply may compromise the elevation and placement of the turnover flap. However, with an individualized approach, surgeons may still find utility with this reconstructive technique in select circumstances for a wider range of patient presentations or reconstruction may be delayed to allow for interim wound healing of the skin bridge. A postauricular approach to local flap reconstruction of the lobule is particularly advantageous given the access to conchal cartilage and the ability to conceal visible scars posterior to the auricle. Additional otoplasty techniques would also be an option with this surgical access if such procedures, such as antihelix formation or conchal setback, were required for management of other helical abnormalities. 11 In this case, the patient and family did not wish any additional upper helical or antihelical refinements.
Conclusion
A congenitally absent lobule is a rare presentation of auricular malformation. Current reconstructive options in lobule reconstruction have been based largely on trauma or oncologic resection and rely on local soft tissue flaps, which generally cause a visible scar on the neck or preauricular area. In the present article, we describe a single-stage procedure for reconstruction of the congenitally absent earlobe that affords access to conchal cartilage, conceals scarring on the posterior auricle, and allows access for other otoplasty techniques. The procedure demonstrated satisfactory cosmesis regarding contour and overall appearance, there were no complications, and results remained stable at the 1-year postoperative follow-up visit.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.