
Abstract
Extramedullary plasmacytoma (EMP) is a malignant tumor formed by monoclonal abnormal proliferation of plasma cells, which is mainly characterized by localized masses and very rare in the larynx, particularly in the false vocal cord. We present a larynx EMP that arises from the false cord without systematic involvement. After surgical resection, the patient received adjuvant radiotherapy and was recurrence-free during the 8-month follow-up.
Extramedullary plasmacytoma (EMP), also known as extraosseous plasmacytoma, is a malignant tumor of the lymphoid hematopoietic system. It is derived from plasma cells but involved in different sites of solitary bone plasmacytoma and multiple myeloma. 1 Extramedullary plasmacytoma is a rare malignant tumor, accounting for approximately 5% of all plasmacytomas. 2 Up to 80% of EMPs occur in the head and neck region of the patients, particularly in the nasal cavity and paranasal sinus (up to 30%), and in the nasopharynx and oropharynx (about 20%). 3 Extramedullary plasmacytoma in the larynx is extremely rare, which may occur in various sites of the larynx such as the epiglottis, vocal cords, and subglottis. 4 Its presence in the false vocal cord has been rarely described. To provide references for clinical treatment, we present an extremely rare case of EMP that arises from the false vocal cord.
A 57-year-old female with progressive hoarseness for 3 months duration presented to our hospital. Laryngoscopy revealed the left false vocal cord was reddish and diffuse swelling (Figure 1A), with smooth surface and normal activity. The narrow-band imaging endoscope did not observe the intraepithelial papillary capillary loop at the abnormal mucosal surface (Figure 1B). Cervical magnetic resonance imaging with contrast enhanced showed the contrast-enhancing soft tissue located in the bilateral supraglottic portion thickened obviously, with short T1 (Figure 2A) and long T2 signal (Figure 2B). This mass was strengthened after enhancement (Figure 2C). Besides, no swollen lymph nodes were identified bilaterally on both sides using the cervical ultrasound. No abnormality was detected in the laboratory examination. Biopsy of the lesion was performed under general anesthesia and microscopic observation found many well-differentiated plasma cells and lymphocytes infiltration. Immunohistochemical analysis revealed that the plasmacytic cells were positive for CD38, CD138, Lambda, and Ki-67. To complete the diagnosis process, the patient underwent the hematologic screening, protein electrophoresis, and bone marrow analysis. Positron emission tomography/computed tomography (PET/CT) scans were performed to exclude a systemic condition. All examinations were negative, and the definitive diagnosis was EMP. Complete surgical resection was not suitable for this patient, then she underwent a cycle of radiotherapy (5 times/week for 5 weeks and 50 Gy each time) and reexamined laryngoscope as see in Figure 1C. An 8-month follow-up after the surgery showed no local recurrence, and the patient is still being followed up.
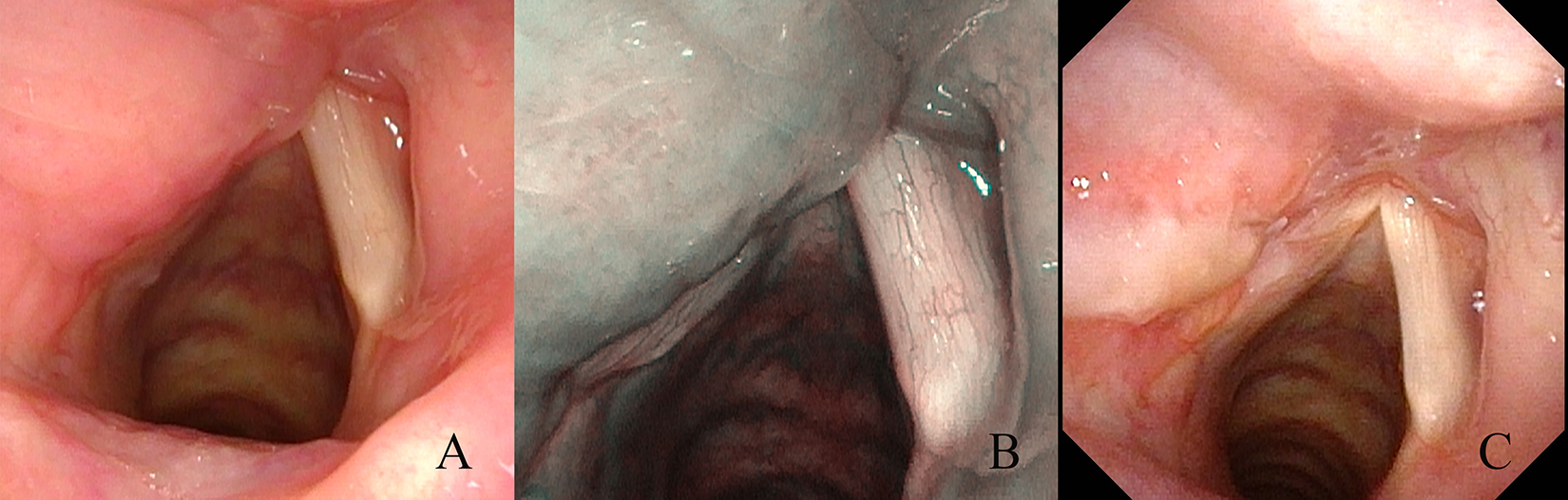
Laryngoscopic version of a mass arising from the left false vocal cord. A, The mass was reddish, diffuse swelling and smooth surface under white light endoscoopy. B, Without abnormal intraepithelial capillary loops under narrow-band imaging endoscopy. C, Laryngeal lesion after surgical resection.
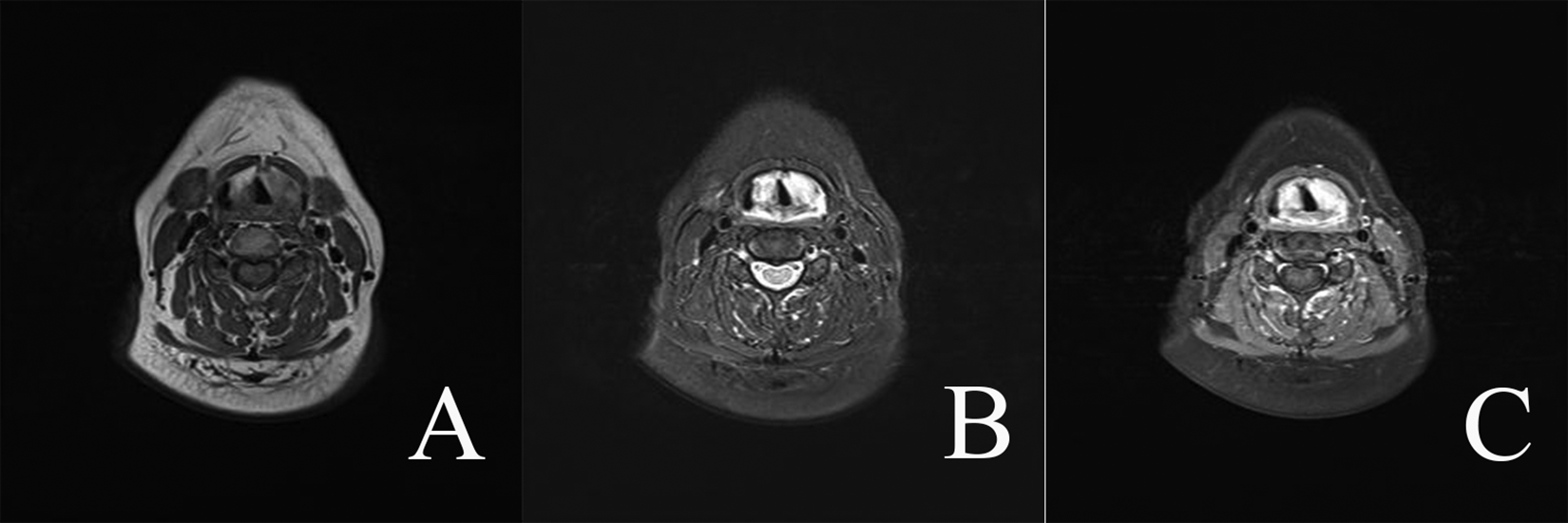
Cervical magnetic resonance imaging with contrast enhanced.
Extramedullary larynx plasmacytoma of the false vocal cord is a very rare condition, which should always be considered in the differential diagnosis of larynx masses. This tumor can appearance many morphologic forms, sometimes as a single, smooth polypoid mass, and sometimes as diffuse swelling tissues just like our patient. 4 Due to the nonspecificity in the clinical symptoms, laryngoscope findings, and imaging examination (CT, MRI, or PET-CT), it is easily misdiagnosed to other diseases, such as laryngeal amyloidosis, lipoid proteinosis, laryngeal lymphoma, or other malignant tumors. The diagnosis of EMP mainly relies on histopathologic examination and immunohistochemistry. So far, the optimal treatment for EMP remains controversial. Single radiotherapy is traditionally used as the first treatment for EMP, followed by a combination of surgery and radiotherapy. Recently, surgery-based treatment, including surgical resection either alone or with adjuvant radiotherapy, has been proposed and proven that it could offer better survival outcomes compared to radiotherapy alone.4,5 The prognosis of head and neck EMP is good, the 5-year survival rate is as high as 80%, but about 20% of patients are prone to recurrence and 15% of patients can progress to multiple myeloma.6,7 In this case, the postoperative recovery after surgical resection combined with postoperative radiotherapy is good, and long-term follow-up should still be done.
Footnotes
Authors’ Note
The data sets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.