
Abstract
An extramedullary plasmacytoma (EMP) is a rare neoplasm characterized by monoclonal proliferation of plasma cells without features of multiple myeloma. Most EMPs occur in the head and neck region, especially in the aerodigestive tract. We herein report a case of an EMP arising from the nasal inferior turbinate. The mass was surgically removed, and a short cycle of radiotherapy was performed after the surgery. There was no recurrence of the tumor after 1 year of follow-up. These result may be useful for physicians who encounter similar situations in clinical practice.
Introduction
An extramedullary plasmacytoma (EMP) is a rare tumor that occurs outside the bone marrow, accounting for only 3% of all plasmacytomas. 1 The most common sites of EMPs are the nasal cavity, sinuses, nasopharynx, and oropharynx. 2 EMPs, which typically affect male and female individuals in a 3:1 ratio, usually occur during the fourth to seventh decades of life.3,4 The treatment process is not yet standardized. To provide references for clinical treatment of this uncommon disease, we herein present a rare case of an EMP arising from the inferior turbinate.
Case report
A 24-year-old woman with a 2-month history of progressive nasal obstruction presented to our department of otolaryngology. Although she experienced no spontaneous epistaxis, bleeding occurred after nose-picking. The patient received no symptomatic treatment during the disease course. Nasal endoscopy showed an extremely large tumor in the left nasal cavity that bled easily when it was touched (Figure 1). Magnetic resonance imaging (MRI) was performed to define the extent of the lesion and showed that the mass was originating from the inferior turbinate. After an intravenous contrast agent was given, T1-weighted images showed significant enhancement of the lesion (Figure 2). Surgical resection of the mass was performed under general anesthesia to improve the nasal obstruction. Plasma radiofrequency ablation was used to remove the mass and inferior turbinate under nasal endoscopy. After removal, the tissue was immediately sent to the pathologist to determine its histologic nature. Immunohistochemical analysis revealed plasmacytic cells that were positive for CD138 and MUM1 (Figure 3). Bone marrow examination was normal. Full-body MRI and positron emission tomography were performed to rule out systemic conditions. Finally, the patient was definitively diagnosed with EMP of the nasal inferior turbinate. Three months after surgery, the patient underwent a cycle of radiotherapy (five times per week for 5 weeks; total dose of 50 Gy). Repeat MRI 1 year later showed no obvious signs of recurrence (Figure 2).
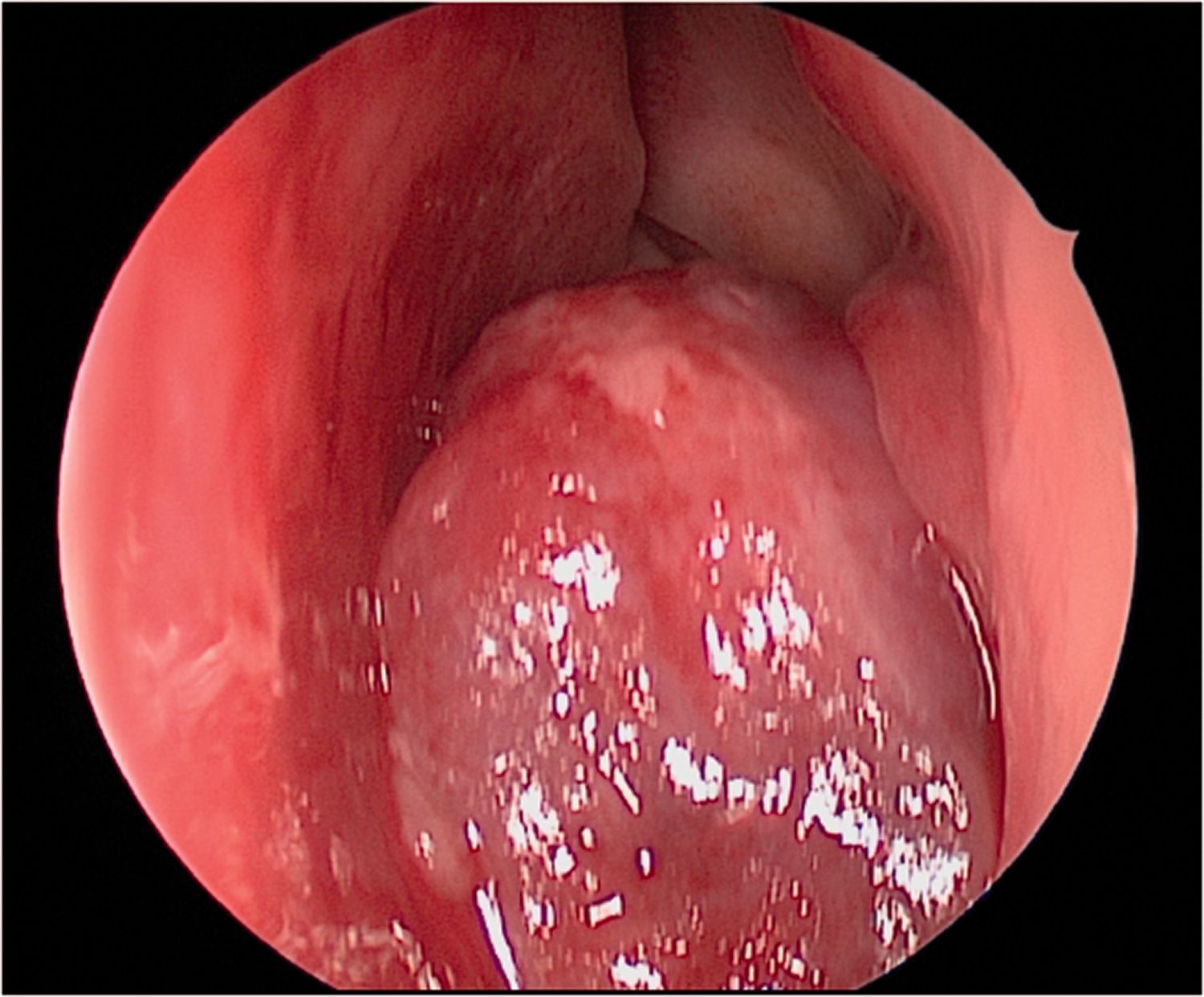
Endoscopic view of the mass in the left nasal cavity.

Magnetic resonance imaging of the patient with a extramedullary plasmacytoma. (a) The T1-weighted coronal image showed a soft tissue lesion involving the left inferior turbinate. (b) The T1-weighted axial image following the administration of contrast medium showed notable contrast enhancement of the mass lesion. (c) Magnetic resonance imaging 1 year after surgery showed no recurrence of the tumor.

Tissue after surgical removal at ×400 magnification. (a) A dense infiltrate of mature plasma cells was present. (b) The cells positively reacted to CD138 staining. (c) The cells positively reacted to MUM1 staining.
This report was approved by the Medical Ethics Committee of Peking University People’s Hospital. The patient provided written informed consent for publication of this case. The reporting of this study conforms to the CARE guidelines. 5
Discussion
Plasmacytomas are malignancies that proliferate with monoclonal B cells and include three types: multiple myeloma, solitary bone plasmacytoma, and EMP. 6 The incidence of EMP is very low, ranging from 0.04 to 3.00 cases per 100,000 individuals. It accounts for 1% of all tumors in the head and neck region and 4% of non-epithelial neoplasms in the sinus tract.7–9 The most common manifestations are soft tissue swelling and nasal congestion. Other clinical features are epistaxis, nasal discharge, pain, proptosis, and cranial nerve palsies.
The diagnosis of EMP is based on histopathological examination, and systemic diseases should be excluded by performing serum and urine protein electrophoresis, immunoelectrophoresis, a skeletal survey, and a marrow biopsy. 10 Several characteristic MRI findings of EMPs have been identified, including the presence of features of expansion, the absence of features of infiltration, and the presence of notable contrast enhancement.11,12 An EMP from the inferior turbinate tends to expand into the nasal cavity or nasopharynx and rarely toward the medial wall of the maxillary sinus.
The treatment of EMP includes surgery, radiotherapy, chemotherapy, or various combinations of these modalities. However, the treatment process is not yet standardized because the tumor is rare. Radiotherapy alone is likely the mainstay of treatment for many cases because of the marked radiosensitivity of EMP. However, the optimal dose of radiation is unclear. 13 Considering the high incidence of eventual progression to multiple myeloma, patients should be kept under constant surveillance. About 30% of patients with EMP develop multiple myeloma within 10 years after the initial diagnosis. 14 Chemotherapy is used only for disseminated disease. Survival depends on whether the disease has disseminated. 15 The 10-year survival rate ranges from 50% to 80%. 16 Surgical resection of a large mass may be successful but should still be followed by radiotherapy. 6 Radiotherapy can be delayed until after surgery, but it is still required because tumor excision results in a very high rate of local recurrence without subsequent radiotherapy. 17 One study also showed that a combination of surgery and radiotherapy had better survival outcomes. 4
Our patient received a combination of radiotherapy and surgery. After a follow-up of 1 year, there was no recurrence of the tumor. Further follow-up is needed to determine the long-term prognosis.
Conclusions
An EMP is a rare tumor, and the treatment process is not yet standardized. We have herein reported a case of EMP arising from the nasal inferior turbinate. After the surgery, radiotherapy was performed. There was no recurrence of the tumor after a follow-up of 1 year. Although further follow-up is needed to determine long-term outcomes, these result may be useful for physicians who encounter similar situations in clinical practice.
Footnotes
Acknowledgement
The authors thank the patient for consenting to publication of this report.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.