
Abstract
Introduction:
Psoriasis is an inflammatory skin disease that is characterized by T-cell-mediated hyperproliferation of the keratinocytes. It develops through immune-mediated mechanisms and is defined as an immune-mediated inflammatory disease. The inner ear is susceptible to inflammatory attacks, and vertigo and dizziness can occur as a complication. There is little information about psoriasis and the vestibular system.
Objective:
This study aimed to investigate the cervical vestibular-evoked myogenic potential (cVEMP) results of psoriasis patients and the effect of psoriasis on the vestibular system.
Materials and Methods:
Randomly selected and included in the study were patients who had been admitted to the Dermatology Outpatient Clinic of the Afyon Kocatepe University Medical Faculty, between November 15, 2017, and March 15, 2018, with the diagnosis of psoriasis, in addition to a healthy control group. This research was designed as cross-sectional study. Ethics committee permission was received. Both cVEMP and distortion product otoacoustic emission (DPOAE) tests were administered to all of the participants. Values were compared between the control group and psoriasis patients.
Results:
The study included 43 psoriasis patients and 40 controls. The duration of treatment of the patients and the drugs that they were using were noted. The psoriasis patients had lower p13–n23 amplitude differences in their cVEMP tests (P < .05). These patients also had lower signal to noise ratio values, at 4 and 6 kHz, on their DPOAE tests (P < .05).
Conclusion:
Psoriasis is an immune-mediated inflammatory disease that can be associated with vestibulocochlear dysfunction.
Introduction
Psoriasis is an inflammatory skin disease that is characterized by T-cell-mediated hyperproliferation of the keratinocytes, the etiology of which is unclear. It is usually characterized by glossy skin or pearly white scales on the extensor surface of the body and the scalp, with limited erythematous plaques or papillae. There is increased immune cell activation in psoriatic patients and there are several factors that trigger this increased immune cell activation. 1
The inner ear and vestibular system are susceptible to inflammatory attacks and vertigo can occur as a complication. The main feature in autoimmune vertigo is the presence of an abnormal immune response directed against delicate components of the inner ear. Russo et al described the autoimmune vertigo according to the clinical presentation. It is divided into 2 groups
2
: Isolated immune-mediated vestibular disorders such as autoimmune inner ear disease, delayed endolymphatic hydrops, Ménière disease, and bilateral vestibulopathy. Association with systemic autoimmune diseases such as rheumatoid arthritis, systemic lupus erythematosus, antiphospholipid syndrome, anticardiolipin syndrome, disseminated vasculitis, relapsing polychondritis, Sjögren syndrome, Vogt-Koyanagi-Harada syndrome, Hashimoto’s thyroiditis, Goodpasture syndrome, Cogan syndrome, Behçet disease, Sarcoidosis, Wegener granulomatosis, and multiple sclerosis. Psoriasis also belongs to this category.
The cervical vestibular-evoked myogenic potential (cVEMP) test is believed to assess saccular vestibular signals carried via the vestibulospinal tract. Recently, cVEMP has been commonly used to evaluate the effects of drugs or systemic diseases on the vestibulocochlear function of the inner ear. 3 This study was the first in the literature to apply the cVEMP test to psoriasis patients. In light of the work previously done, this study aimed to investigate the effects of psoriasis on the vestibular system and inner ear using the cVEMP and distortion product otoacoustic emission (DPOAE) tests. 4
Materials and Methods
Patients who were admitted to the Dermatology Department of the Afyon Kocatepe University Faculty of Medicine Hospital, between November 15, 2017, and March 15, 2018, who had been diagnosed with psoriasis by a specialist or and were continuing to receive psoriasis treatment were included in the study.
The patients and control groups were age and sex matched. None of the individuals in the healthy control group had any known diseases or drug use. None of the healthy control group or psoriasis patients had any vertigo-related medical history.
The following patients were excluded from the study: those who did not volunteer to participate; those who were exposed to occupational or environmental noise; those with other inflammatory diseases or comorbidities, such as hypertension, diabetes mellitus, thyroid function disorders, liver function disorders, kidney function disorders, heart failure, chronic otitis, tympanosclerosis, or otosclerosis; and those who had ear-related pathologies or had previously undergone ear surgery.
Approval for this study was received from the Ethics Committee Commission of the Afyon Kocatepe University Faculty of Medicine, dated November 3, 2017, and numbered 2017/11-284.
Vestibular Elevation With the cVEMP Test
The cVEMP test was used to measure the surface electromyographic activity of the sternocleidomastoid cortex with an interacoustics eclipse device at the Department of Otorhinolaryngology-Audiometry of Afyon Kocatepe University. A 95-dB 500-HZ tone burst was used. Patients who were nonresponders to the test were excluded.
Hearing Elevation With DPOAE Test
The DPOAE is a specific test for assessing the cochlear function. The test is reliable and sensitive enough to detect even minor cochlear pathologies. The Echoport ILO288 USB (Otodynamics Ltd) was used for the DPOAE measurements. Signal to noise ratio (SNR) values at 1000, 1500, 2000, 4000, 6000, and 8000 Hz were recorded. In these studies, hearing thresholds over 8000 Hz were not evaluated because of the low number of responses in the tests.
Data Entry and Statistical Analyses
Statistical analyses of the study data were performed using SPSS version 15.0. All analyses were performed with 95% confidence intervals. Mean, standard deviation, and median values were used when descriptive analyses were presented. Independent groups were assessed by t test, while 2-group comparisons were assessed by the Mann-Whitney U test, and variables with normal distribution (parametric variables) were evaluated between the groups. The Spearman correlation test was used to analyze the measured data in comparison with each other. P < .05 was considered statistically significant.
Results
The study was conducted with 43 patients with psoriasis and 40 healthy controls. These participants included 47 women and 36 men. There were 22 male and 21 female patients with psoriasis. The healthy control group consisted of 14 males and 26 females. The average age of all participants was 38.5 ± 17.4 years. Patients with psoriasis had a mean age of 42.2 years, and the healthy control group had a mean age of 33.5 years.
Psoriatic arthritis was present in 7 (16.3%) of the 43 psoriasis patients. The mean duration of disease was 14.6 years and the mean duration of treatment was 11.7 years among the psoriasis patients. The mean Psoriasis Area and Severity Index (PASI) score of the psoriasis patients was 6.8 ± 5.2.
In the psoriasis patients group, 26 received systemic therapy and 17 received only local therapy. In the systemic therapy group, 10 patients used biological agents comprising ustekinumab (interleukin [IL]-12 + IL-23 blocker) by 2 patients, efalizumab (LFA-1/CD11a blocker) by 1 patient, and tumor necrosis factor alpha (TNF-α) blocker by 7 patients. The others of the systemic therapy group used the following drugs: 15 patients used metothrexat + folbiol combination, 8 patients used acitretin, 3 patients used psoralen and ultraviolet A (PUVA), and 4 patients used narrowband ultraviolet B (NBUVB).
When the psoriasis patients were compared with the healthy control group, the cVEMP values of psoriatic patients revealed significantly lower p13–n23 amplitude differences (millivolt) in both ears (P < .05; Table 1).
Significantly Lower p13–n23 Amplitude Differences in the cVEMP Tests of the Psoriasis Patients When Compared to the Healthy Control Group (P < .05).
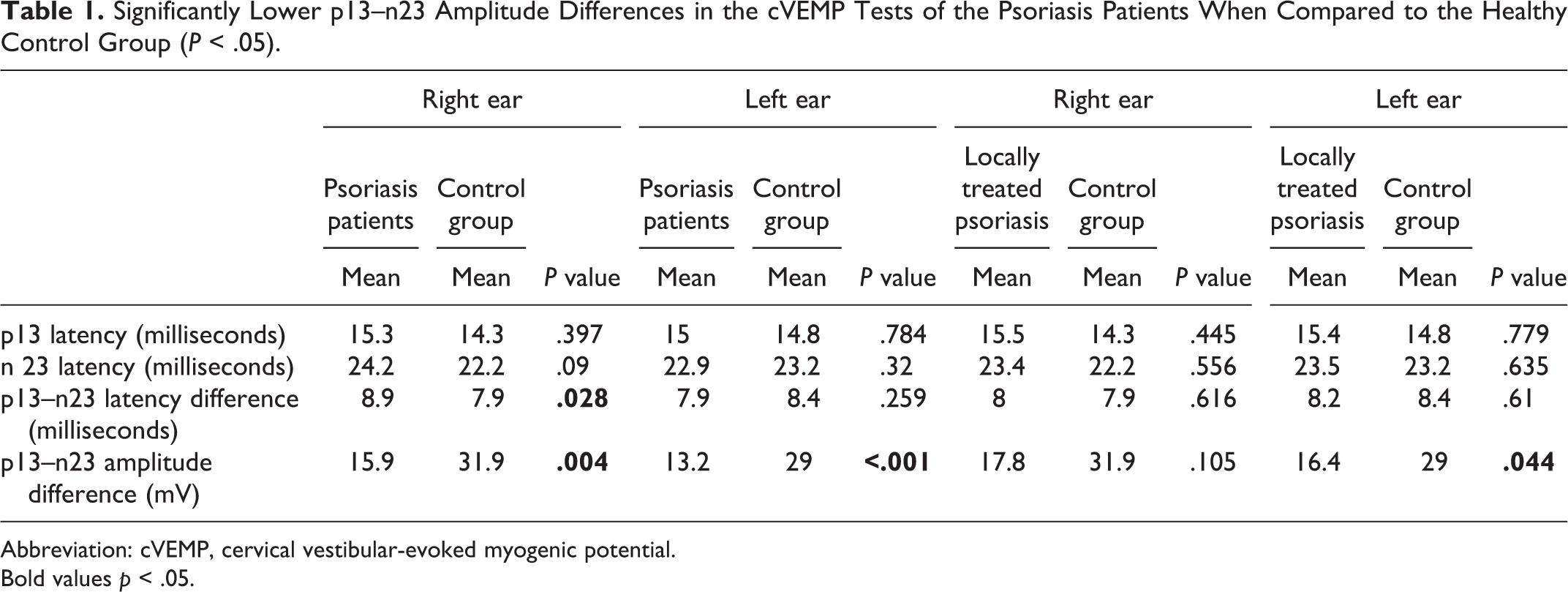
Abbreviation: cVEMP, cervical vestibular-evoked myogenic potential.
Bold values p < .05.
No significant difference was found between the psoriasis patients with psoriatic arthritis and those without psoriatic arthritis in terms of the cVEMP values (P > .05).
Locally treated psoriasis patients had significantly lower p13–n23 amplitude differences in the left ear when compared to the healthy control group (P < .05; Table 1). The p13–n23 amplitude differences in patients with higher PASI scores were found to be lower and significant (P < .05).
Psoriasis patients also had hearing loss due to the vestibulocochlear inflammatory effect. When the DPOAE test results of the psoriasis patients were compared with those of the healthy control group, it was observed that the psoriasis patients had significantly lower SNR values, at 4000 and 6000 Hz, in both ears (P < .05; Table 2).
SNR Values of the DPOAE Tests of the Psoriasis Patients and the Healthy Control Group.
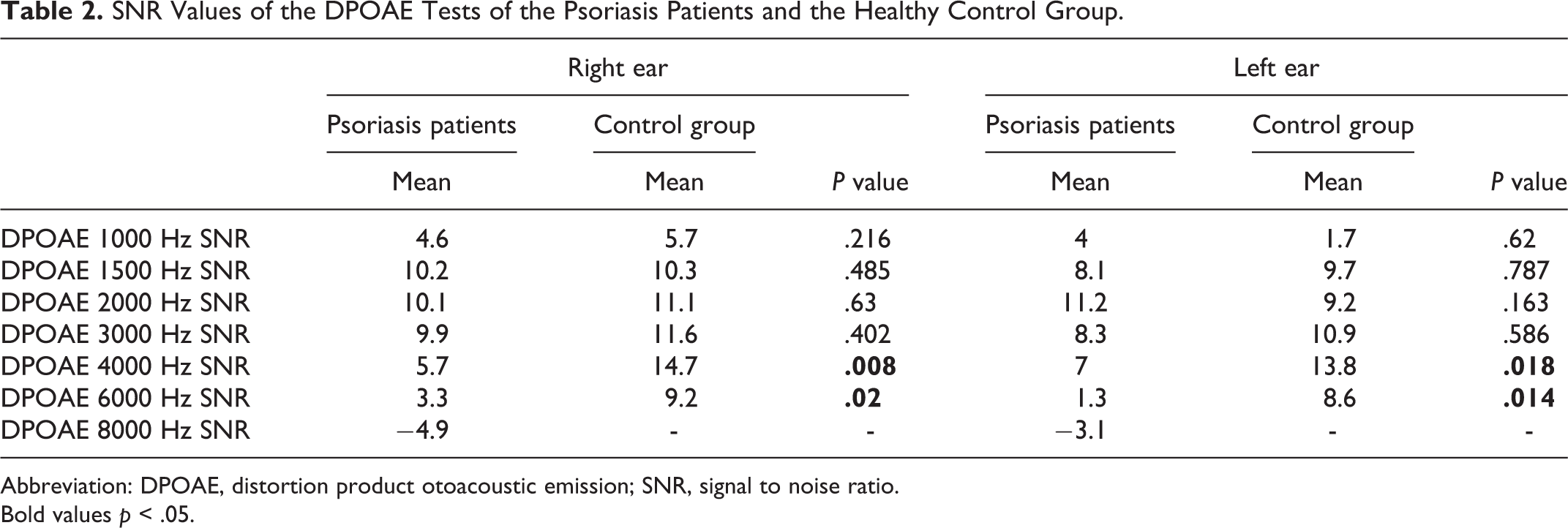
Abbreviation: DPOAE, distortion product otoacoustic emission; SNR, signal to noise ratio.
Bold values p < .05.
Discussion
Psoriasis involves the rapid transformation of the epidermis as a consequence of the accelerated proliferation and differentiation of epidermal keratinocytes, where the mitotic rate of basal keratinocytes increases and leads to thickening of the epidermis. Several factors trigger this increased immune cell activation. Tumor necrosis factor α is found to be high in psoriatic lesions. In psoriatic skin, the TNF-α, T lymphocytes, and pro-inflammatory cytokines produced by keratinocytes and macrophages have been found at high levels. Interleukin 1, IL-6, and IL-8 induce the production of pro-inflammatory cytokines. The source of TNF-α in psoriasis is not clear. 1
Recent studies investigating the comorbidities associated with psoriasis have shown that psoriasis is not limited to the skin. In psoriatic patients, metabolic syndrome, coronary heart disease, hyperlipidemia, obesity, and inflammatory bowel disease rates have all been found to be higher than in the normal population.5,6
Cervical vestibular-evoked myogenic potential is a reliable and quick test for the assessment of vestibular function. Many abnormal results like the elongation of p13–n23 latency or lower amplitude voltages have been shown in Ménière patients, vestibular neuritis, and benign paroxysmal positional vertigo patients. 7
There have been very few studies about vestibular functions in psoriasis patients. Amor-Dorado et al. compared 60 psoriatic arthritis patients and 60 healthy controls and reported that the psoriasis patients had abnormal computerized dynamic posturography test results (P < .05). 8 Temel et al. compared 61 psoriasis patients and 61 controls using a saccadic test and reported that significantly abnormal oculographic results were obtained for the psoriasis patients. 9
In this study, the psoriasis patients had significantly lower p13–n23 amplitude differences in the cVEMP test. These findings suggested abnormal cVEMP results and vestibular dysfunction in the psoriasis patients. There have been no other studies in the literature evaluating vestibular functions with cVEMP in psoriasis patients. The presence of psoriatic arthritis, gender, and duration of disease or treatment had no influence on the cVEMP values.
In a recent study, Ertugrul et al. reported that psoriasis patients had significantly higher abnormal caloric test results than the control group. 10 The PASI score of psoriasis patients with abnormal caloric responses was significantly higher than that of patients with normal caloric response. In the current study, the p13–n23 amplitude differences in patients with higher PASI scores were found to be lower and significant.
In this study, the psoriasis patients had significantly lower SNR values in both ears at 4000 and 6000 Hz on the DPOAE test. These findings suggested that the cochlea is a target organ in psoriasis. In the study of Ertugrul et al., no significant difference was found in the SNR values between the groups in either ear. 10
Localized treatments do not cause vestibular impairment in psoriasis, and locally treated patients provided a good opportunity to evaluate the effect of psoriasis on the vestibular system; however, there is a question that arises from this situation. Receiving only localized treatment may be the cause of mild psoriasis versus receiving systemic treatment that may be the cause of severe psoriasis and inflammation. The effect of systemic treatment could not be determined in this study. Moreover, this study also included a small number of participants. These comprise the limitations of this study.
Among the psoriasis patients, lower p13-n23 amplitude differences in the cVEMP test were in agreement with the findings of Ertugrul et al. The results indicated that psoriasis patients may suffer from vestibular dysfunction.
Conclusion
Psoriasis is an inflammatory and immune-mediated disease. Many findings have shown vestibulocochlear dysfunction in immune-mediated inflammatory diseases. This study showed that psoriasis patients had significantly abnormal cVEMP results and may have had vestibulocochlear dysfunction when compared to the control group. Larger, longitudinal, or prospective studies are required to investigate these patients.
Supplemental Material
Supplemental Material, sj-pdf-1-ear-10.1177_0145561320970683 - Vestibular Function in Psoriasis Patients
Supplemental Material, sj-pdf-1-ear-10.1177_0145561320970683 for Vestibular Function in Psoriasis Patients by Abdullah Kınar, Abdulkadir Bucak, Şahin Ulu, Nilay Duman and Nur Betül Baştuğ in Ear, Nose & Throat Journal
Footnotes
Author’s note
Nilay Duman is now affiliated to Bursa City hospital, Turkey.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.