
Abstract
Psoriasis is a chronic, autoinflammatory skin disease. Tumor necrosis factor-alpha inhibitors are commonly used for the treatment of moderate-to-severe psoriasis; however, paradoxical psoriatic eruptions are a well-recognized adverse effect. There are no validated guidelines to manage this. We present the case of a 48-year-old woman with severe pustular psoriasis who developed acute paradoxical reactions after her first two infusions of infliximab, requiring hospitalization. She achieved disease control after transitioning to secukinumab, an interleukin-17 inhibitor. This case highlights the importance of early monitoring for paradoxical reactions in patients with severe psoriasis after initiating tumor necrosis factor-alpha inhibitor therapy and the value of transitioning to an alternative biologic class for effective management.
Introduction
Psoriasis is a chronic, autoinflammatory skin disease driven by inflammatory cytokines, including tumor necrosis factor-alpha (TNF-α), interleukin-17 (IL-17), and IL-23. TNF-α inhibitors are widely used for the treatment of moderate-to-severe psoriasis; however, paradoxical psoriatic eruptions are a well-recognized side effect.1–4 These reactions are most commonly reported in patients receiving TNF-α inhibitors for conditions such as inflammatory bowel disease, rheumatoid arthritis, and ankylosing spondylitis, with fewer cases reported for patients with psoriasis.1,5 Infliximab is the most frequently reported to be associated with paradoxical psoriasis. 4 No validated guidelines exist for TNF-α inhibitor-induced paradoxical psoriasis. We present the case of a 48-year-old woman with long-standing severe pustular psoriasis who developed acute paradoxical psoriasiform reactions to her first two doses of infliximab, ultimately achieving disease control with the IL-17 inhibitor, secukinumab. Informed consent was provided by the patient for publication.
Case report
A 48-year-old woman with an 18-year history of plaque and pustular psoriasis presented to the emergency department (ED) with a 3-day history of worsening psoriasis. Notably, she had two prior hospital admissions for pustular psoriasis flares, one of which was complicated by mixed hypovolemic and septic shock secondary to skin failure. At this presentation, her pustular psoriasis was being treated with cyclosporine 200 mg twice daily.
Examination revealed numerous ruptured vesicles with foul-smelling drainage on her back, intertriginous areas, and upper extremities. Laboratory investigations revealed an acute kidney injury (AKI) related to hypovolemia. Intravenous fluids were initiated, and cyclosporine was held. She required transfer to the intensive care unit for septic shock and hypoxemic respiratory failure. Skin culture grew Staphylococcus aureus and Streptococcus dysgalactiae. She was treated with intravenous piperacillin–tazobactam, vasopressors, albumin, and intravenous hydrocortisone.
The dermatology service initiated infliximab at 5 mg/kg and an oral corticosteroid taper at prednisone 40 mg daily. During the infliximab infusion, she developed extremity pain, diaphoresis, and an urticarial eruption. This was managed by decreasing the infusion rate. It was decided to proceed with the second infliximab dose as scheduled, with premedication.
The following day, there was increased erythema, pruritus, and pustular drainage. The dermatology service suspected a mild acute infusion reaction and a potential component of corticosteroid withdrawal. The taper was decreased from 10 to 5 mg weekly. During the remainder of her admission, skin lesions were managed with topical betamethasone valerate and petroleum, and pain was managed with oral hydromorphone. She was discharged 1 week later on prednisone 30 mg.
She received the second dose of infliximab 5 days after discharge. Two days later, she presented to the ED with another pustular psoriasis flare, AKI, and a pain crisis requiring admission. She was unable to ambulate, wear lower-body clothing, or use the toilet due to pain. Examination revealed widespread erythema with large, well-demarcated plaques, and peripheral desquamating scale involving the trunk, arms, thighs, buttocks, and face. There were pustules on the left inner thigh and right arm, and hyperkeratosis with fissuring on the palms and soles. There was no mucosal involvement. Her Psoriasis Area and Severity Index (PASI) score was 22 (Figure 1). She was afebrile with liver enzymes and eosinophils within normal limits, and elevated neutrophils. Paradoxical psoriasis induced by infliximab was diagnosed. Infliximab was discontinued, and a secukinumab application was submitted.
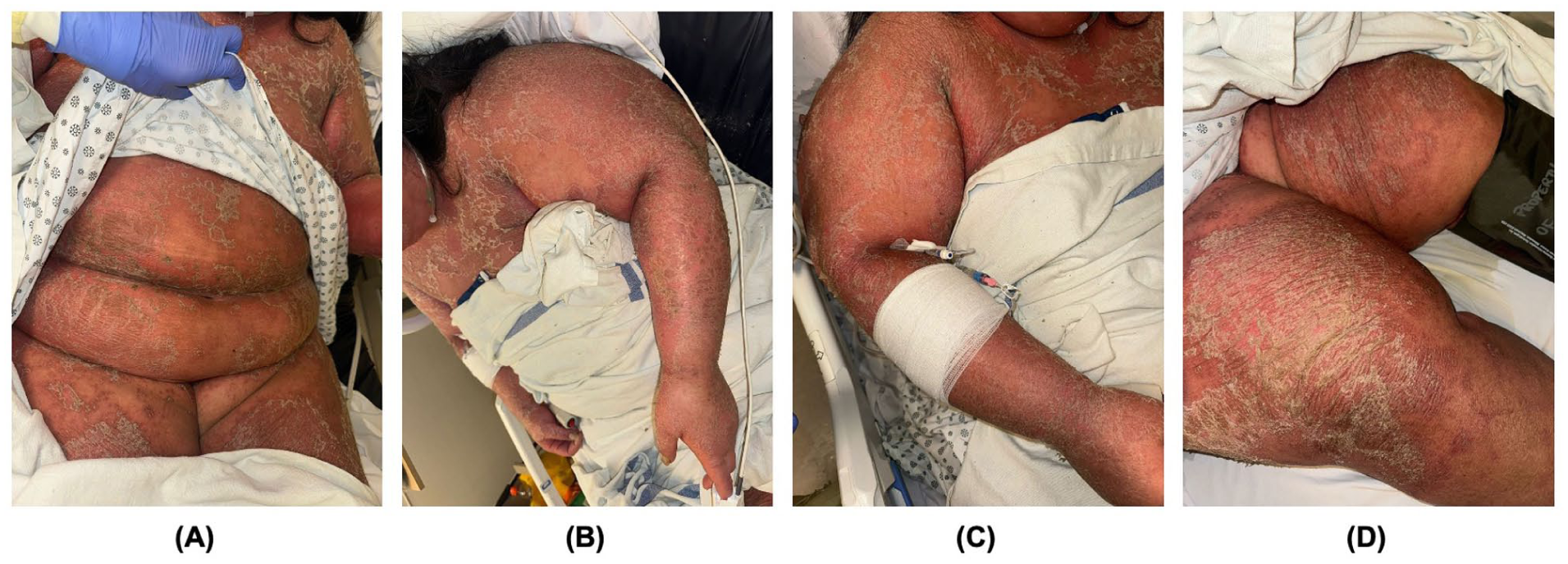
Two days after the patient’s second infliximab infusion, examination revealed widespread erythema with large, well-demarcated plaques, and peripheral desquamating scale involving the trunk (a), arms (b, c), thighs (d), buttocks, and face. There were pustules on the left inner thigh and right arm, and hyperkeratosis with fissuring on the palms and soles.
She was discharged 1 week later with improving psoriatic lesions using topical corticosteroids and the continued prednisone taper. Oral acitretin 50 mg daily was taken for 1 month while awaiting secukinumab approval.
Secukinumab treatment was initiated with a loading dose of 300 mg weekly for 5 weeks, followed by 300 mg monthly. Her pre-treatment PASI score was 6.6, which improved to 1.2 after loading doses. Four months after initiating secukinumab, the PASI score was 0.5.
Discussion
While classical psoriasis is primarily T-cell mediated, paradoxical psoriasis by TNF-α inhibitors is thought to be relatively less T-cell dependent. Instead, it is associated with an overexpression of type I interferons (IFNs), resulting in acute inflammation.2,3 Typically, TNF-α promotes the maturation of plasmacytoid dendritic cells to limit production of type I IFN. Inhibition of TNF-α consequently results in type I IFN overproduction that may drive the exacerbation of pre-existing psoriasis or trigger new lesions. 3 However, it is important to recognize that IFN also plays a role in classical psoriasis, as the cytokine profile of Th1 includes IFN-γ, TNF-α, and IL-2. Therefore, paradoxical and classical psoriasis may be overlapping conditions with shared IFN-driven mechanisms.
This case is notable for the rapid onset of paradoxical psoriasis, with eruptions occurring within 24 hours of both infliximab infusions. A systematic review found a mean onset of 14 months after TNF-α inhibitor initiation, though most cases involved non-dermatologic autoimmune conditions such as Crohn’s disease and rheumatoid arthritis. 1 The acute onset in this patient may be associated with long-standing severe pustular psoriasis, predisposing her to a more immediate reaction.
An important differential diagnosis was acute generalized exanthematous pustulosis (AGEP), a severe cutaneous drug reaction characterized by sudden onset of pinpoint, non-follicular pustules on an erythematous base, typically associated with fever, neutrophilia, and in some cases, systemic involvement.6,7 Distinguishing AGEP from pustular psoriasis can be challenging, as they share clinical and histopathological features. Importantly, AGEP is usually self-limiting, resolving within 1 to 2 weeks following offending agent discontinuation. By contrast, our patient remained afebrile, showed a lack of improvement with infliximab discontinuation alone, and ultimately required secukinumab treatment. Given this clinical course, paradoxical psoriasis was favored.
Corticosteroid withdrawal may have exacerbated the patient’s reaction, as systemic corticosteroid tapering can trigger pustular psoriasis. 8 She transitioned from intravenous hydrocortisone to oral prednisone, tapering at the time of the first infusion, and remained on the taper schedule during the second infusion. This highlights that careful tapering is crucial when initiating biologic therapies for severe psoriasis to minimize flare risk. In our patient, this was managed by adjusting her taper from 10 to 5 mg weekly.
There are no validated guidelines for managing TNF-α inhibitor-induced paradoxical psoriasis. Reported strategies include treatment discontinuation and intraclass switching to another TNF-α inhibitor or a different biologic class, or continuing treatment with additional adjunctive treatment. 2 We demonstrated successful management through infliximab discontinuation and switching to an alternative biologic agent, secukinumab. Secukinumab, which is approved for the treatment of moderate-to-severe plaque psoriasis, directly targets IL-17A, a key proinflammatory cytokine in psoriasis pathogenesis. 9
This case emphasizes that while TNF-α inhibitors are frequently used to treat psoriasis, they can also, paradoxically, exacerbate the disease. Although corticosteroid tapering and other factors may have contributed, infliximab remains the most likely trigger. Clinicians should remain vigilant for paradoxical reactions during TNF-α therapy and consider switching to an alternative biologic class, such as IL-17 inhibitors.
Footnotes
Consent for publication
Written informed consent was obtained from the patient for their anonymized information and images to be published in this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.