
Abstract
Importance
Galvanic vestibular-evoked myogenic potential (gVEMP) elicited by galvanic stimuli to assess the audiovestibular disorders has garnered less attention.
Objective
This systematic review aims to explore the clinical application of the gVEMP test in audiovestibular disorders, with the potential for widespread promotion in the future.
Design
This review was developed from peer-reviewed articles published in those journals listed on Journal Citation Reports.
Setting
University hospital.
Participants
Articles were collected from the PubMed database of the US National Library of Medicine, Scopus, Embase, Google Scholar, and Cochrane Library.
Intervention
Results of vestibular-evoked myogenic potential (VEMP) elicited by either acoustic, vibratory, or galvanic mode were compared.
Main Outcome Measures
Based on the guidelines (PRISMA 2020 statement) for reporting reviews.
Results
Initially, 1076 articles were retrieved from 1994 to 2023. Following the exclusion of duplicate reports, unrelated articles, non-SCI journals, and papers covering a similar topic published in a later period, 43 relevant papers were ultimately selected.
Conclusions and Relevance
The ocular and cervical VEMP testing using galvanic stimuli should be accompanied by testing with acoustic or vibratory stimuli to precisely delineate the affected receptors and/or afferents in audiovestibular disorders. Clinical application of the gVEMP test in audiovestibular disorders includes: (1) Evaluating the involvement of vestibular afferents; (2) Assessing the residual function of the vestibular system; and (3) Predicting the outcome of audiovestibular disorders.
Keywords
Introduction
History Background
In 1964, Cohen et al 1 utilized electrical stimulation on the ampullary nerve of the semicircular canal (SCC) in animals to explore the enigma of eye movement. Later, Suzuki et al 2 applied high-frequency galvanic current to stimulate a single utricular nerve. This elicited excitatory activities in the inferior oblique and rectus muscles on the contralateral side, and in the superior oblique and rectus muscles on the ipsilateral side, resulting in conjugate eye movements in both eyes. These significant animal experiments served as the foundation for the idea of investigating the activity of the inferior oblique muscle opposite to the stimulated side, which later contributed to the recording of ocular vestibular-evoked myogenic potential (oVEMP).3,4
In 1994, under click stimulation on the ears, Colebatch et al 5 successfully captured the VEMP response on the contracted cervical muscles, which was later termed as cervical VEMP (cVEMP). The first positive and second negative polarities of the cVEMP, occurring at the latencies of 13 to 23 ms, were defined as waves p13 and n23, respectively. It originates at the saccular macula, then via the sacculo-collic reflex, ultimately terminating on the motor neurons of the cervical muscles. 6 In 1998, Watson and Colebatch 7 introduced the galvanic VEMP (gVEMP) test to detect retro-labyrinthine lesions using brief galvanic stimulation.
In 2005, Rosengren et al 3 reported that VEMP can also be obtained on the extraocular muscles, referred to as oVEMP. The initial negative-positive biphasic waveform, occurring at the latencies of 10 to 15 ms, comprised the nI and pI peaks of the oVEMP, respectively. 4 The oVEMP has been primarily associated with utricular function. 8 It follows the crossed vestibuloocular reflex (VOR) via the superior vestibular nerve to the extraocular muscles of the opposite side. 9 Thereafter, there are 3 modes of stimulation used to induce cVEMP and oVEMP, namely acoustic, vibratory, and galvanic stimuli. 10
In animal experiments, Murofushi et al 11 utilized acoustic stimuli on guinea pigs to elicit cVEMPs. This was based on the irregular saccular neurons, primarily originating from the striola of the saccular macula, which are particularly responsive to acoustic stimuli and activated by linear acceleration.12,13 In contrast, low-intensity vibratory stimuli have been shown to selectively activate irregular afferents from the saccular and utricular macula in animals.14 -16 Curthoys 17 reported that both acoustic and vibratory stimuli are potent activators for the type I hair cells at the striola. This is because the endolymph displacement caused by sound or vibration deflects the type I hair cells at the striola, leading to activation of the irregular afferents that innervate them. In other words, the otoliths function as seismometers at high frequencies and as accelerometers at low frequencies, with VEMPs being predominantly an otolith-driven response. 17
Rationale and Objective
Over the past 3 decades, basic research has laid the foundation for using cVEMP and oVEMP tests to assess audiovestibular disorders. 18 This approach has quickly gained popularity in clinical practice.19 -21 However, the absence of cVEMP by acoustic/vibratory mode suggests a lesion along the sacculo-collic reflex pathway; it does not specify whether the lesion is at the saccule itself or along its afferent pathways. Similarly, the absence of oVEMP in response to acoustic or vibratory stimulation may indicate a lesion along the utriculo-ocular reflex pathway. However, it remains unclear whether the lesion is located at the utricle or higher up in the pathway. Therefore, VEMP testing using galvanic stimulation has been adopted for clarifying this distinction. 22
Although cVEMP and oVEMP tests using acoustic or vibratory stimuli are widely adopted in clinical practice,23,24 gVEMP testing for assessing audiovestibular disorders has garnered less attention. This systematic review aims to explore the clinical application of the gVEMP test in audiovestibular disorders, with the potential for widespread promotion in the future.
Methods
Study Design
This review enrolled articles published in journals listed on Journal Citation Reports, and the methodology was based on the guidelines proposed by Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA 2020 statement). 25
Search Strategy
Literature written in English from 1994 to 2023 was initially surveyed by 2 independent reviewers through the PubMed database of the US National Library of Medicine, Scopus, Google Scholar, and the Cochrane Library. The search terms from databases comprised VEMP, galvanic vestibular stimulation, galvanic cervical VEMP, and galvanic ocular VEMP. The initial search in each database yielded 1076 articles.
Inclusion Criteria
- Galvanic cervical or ocular VEMP in audiovestibular disorders.
- Galvanic VEMP in basic research.
Exclusion Criteria
- Studies unrelated to audiovestibular disorders.
- Studies without mentioning inner ear test results.
- Reports in a non-English language or published in non-SCI journals.
- Duplicate articles or case reports.
Data Extraction
Each article was thoroughly reviewed to extract the most relevant information in line with the objective of this review. Two independent neurotologists examined the titles and abstracts of the selected articles to assess their eligibility. There was no disagreement between the 2 reviewers.
Data Analysis
The inner ear test battery is essential for diagnosing audiovestibular disorders. Results of cVEMP/oVEMP elicited by either acoustic, vibratory, or galvanic mode were compared.
Certainty Assessment
Papers demonstrating a clear resolution of gVEMP were considered for the certainty assessment. A third specialist was involved in discussions to resolve any disputes that arose between the 2 reviewers during the quality assessment process.
Results
Literature Search
Initially, 1076 articles were retrieved, spanning from 1994 to 2023. Following the exclusion of duplicate reports (n = 129), unrelated articles (n = 786), non-SCI journals (n = 19), and papers on similar topics published in later periods (n = 95), the remaining articles were considered for review. As a result, 43 relevant papers were ultimately selected (Figure 1).
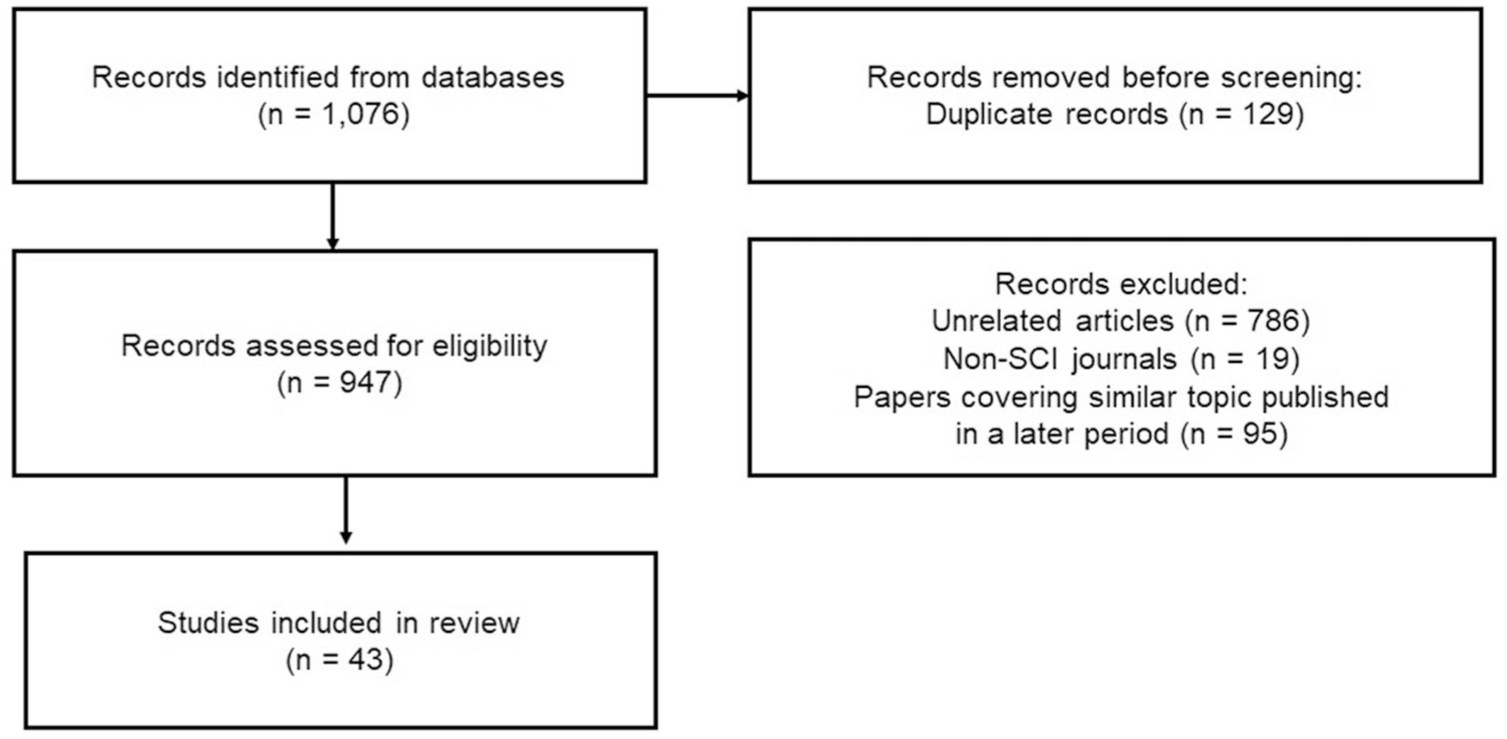
Illustration of how the selection of articles is made, with additional details of the number of studies.
Quality Assessment
Electrodes placement
For galvanic stimulation, selectivity is influenced by the electrode placement and the stimulation waveform. Bipolar electrodes are the most selective. Electrodes with a large surface area were used on both mastoid sites, delivering a low galvanic current. 22 The electrodes for administering galvanic stimuli were placed on both mastoid sites (cathode) and forehead (anode). During galvanic cVEMP test, the active electrodes were positioned on the upper half of the bilateral sternocleidomastoid (SCM) muscles, while a reference electrode was on the suprasternal notch, and a ground electrode on the forehead. 26 For eliciting the galvanic oVEMP test, the active electrode was positioned around 1 cm below the lower eyelid, the reference electrode was placed about 2 cm below the lower eyelid, and the ground electrode was located at the sternum. 10
Stimulation waveform
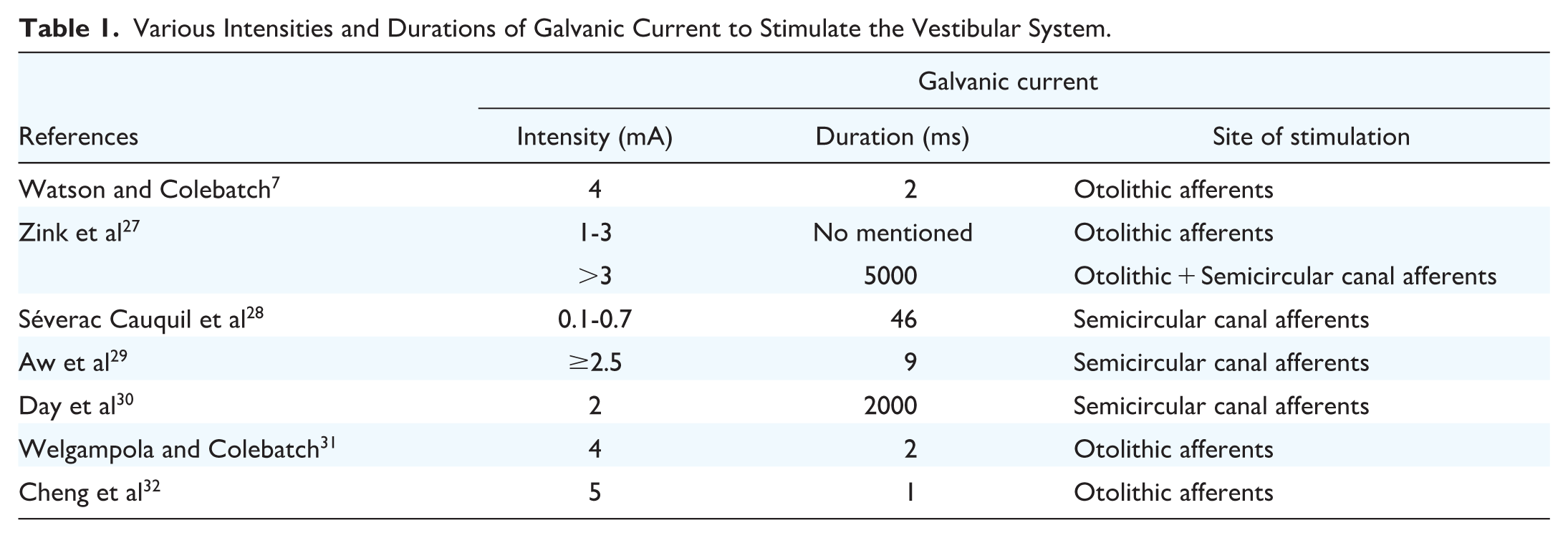
Watson and Colebatch 7 used a galvanic current with an intensity of 4 mA and a duration of 2 ms to assess the otolithic afferents. Zink et al 27 suggested that galvanic vestibular stimulation at low current intensities (1-3 mA) is particularly effective for exciting otolithic responses. When higher current intensities (>3 mA) for 5 s were adopted, additional SCC responses were elicited, resulting in the horizontal-rotatory nystagmus superimposed on static torsional deviation.28,29 Day et al 30 utilized low current intensity (2 mA) but lasting for a long duration (2 s) to excite the SCC. As a result, elevating intensity or extending the duration of the galvanic current may increase the amplitude of gVEMP until it achieves saturation.7,31 Thus, afferents in the otolithic transient and sustained systems exhibit distinct responses to stimulus onset and continuous stimulation. They likely have different projections and, most importantly, different activation thresholds for electrical stimulation as well as varying adaptation rates to sustained stimulation. 22
Cheng et al 32 compared galvanic cVEMPs using various current intensities (1-5 mA) and durations (0.1-1.0 ms), and found that galvanic stimulation at 5 mA/1.0 ms yielded higher response rates and larger p13-n23 amplitude than those in groups of 5 mA/0.5 ms and 3 mA/1.0 ms. Table 1 summarizes the intensities and durations of galvanic current to stimulate the vestibular system utilized at various laboratories.
Various Intensities and Durations of Galvanic Current to Stimulate the Vestibular System.
Nonetheless, it is important to consider the potential adverse reactions from galvanic stimulation, which may include a strong sensation of spinning or falling, nausea, a metallic taste, or increased pain due to higher levels of electrical energy exposure. 33 Cheng et al 32 reported that a 5 mA intensity for a duration of 1.0 ms of galvanic current is suggested to elicit a large galvanic cVEMP amplitude without exceeding subject pain tolerances.
Furthermore, Ozeki et al 34 suggested an ideal repetition rate of 5/s for consistent gVEMP, just like the 5/s repetition rate for inducing cVEMP by click stimuli. 35
Obtaining galvanic cVEMP and oVEMP
To reduce the substantial electrical artifact present in the original galvanic cVEMP waveform, Watson and Colebatch 7 proposed a method for obtaining galvanic cVEMP with minimized artifacts. The subject received galvanic stimulation with and without SCM muscle contractions for obtaining a galvanic cVEMP. Responses elicited without SCM muscle contraction were subtracted from those obtained with SCM muscle contraction to yield the final galvanic cVEMP (Figure 2). Similarly, the galvanic oVEMP responses obtained during gaze down were subtracted from those obtained during gaze up to produce the final galvanic oVEMP (Figure 3).
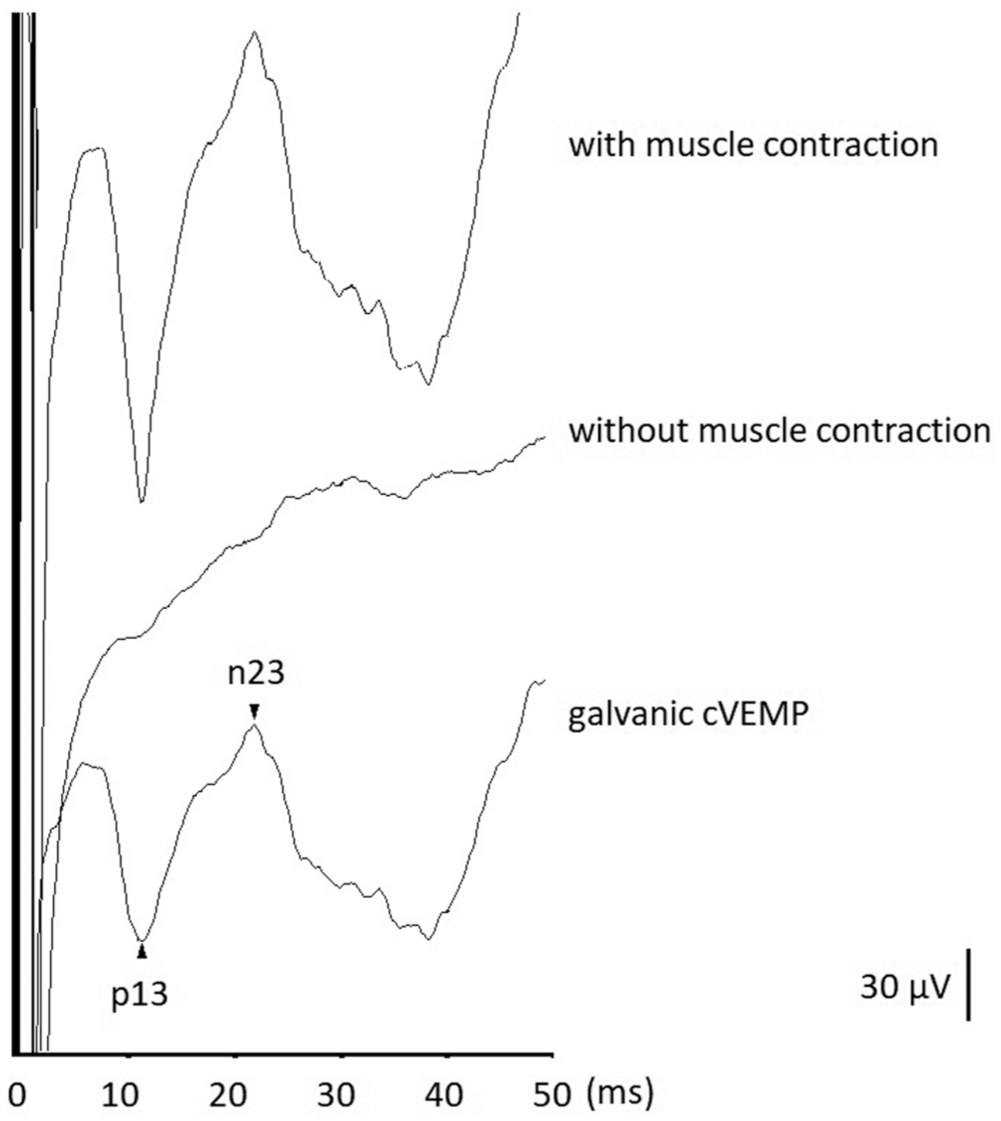
Illustration of how the galvanic cVEMP is obtained. To remove electrical artifacts, the responses without sternocleidomastoid muscle contraction are subtracted from those with sternocleidomastoid muscle contraction, and a galvanic cVEMP waveform is derived after subtraction. cVEMP, cervical vestibular-evoked myogenic potential.

Illustration of how the galvanic oVEMP is obtained. To remove electrical artifacts, the responses by gaze down are subtracted from those by gaze up, and a galvanic oVEMP waveform is derived after subtraction. oVEMP, ocular vestibular-evoked myogenic potential.
Discussion
Advantages of Each Stimulation Mode
There are 3 stimulation modes to elicit cVEMP and oVEMP: acoustic, vibratory, and galvanic. 10 Clinically, disorders affecting the cVEMP responses highlight the significance of selectively stimulating a single saccule and its afferent, emphasizing its primary importance. This preference arises from the advantage of the acoustic mode, which allows for the separate stimulation of each ear.
The advantage of the vibratory mode is that the oVEMP elicited by the vibratory mode is larger than that by the acoustic mode. Although the specific contribution of the saccular/inferior vestibular nerve versus the utricular/superior vestibular nerve to the VEMP response under vibratory mode is not yet well-defined, vibratory mode offers clinical advantages in detecting mass lesions, whereas the acoustic mode provides more precise site-specific information. 36 Restated, the acoustic mode offers unilateral stimulation at the receptor level, and the vibratory mode provides bilateral stimulation at the receptor level. In contrast, the galvanic mode delivers unilateral stimulation at the afferent level. Thus, galvanic mode combined with acoustic/vibratory mode to elicit VEMPs enables a more comprehensive understanding of whether the lesion is at the receptor and/or its afferent.37,38 Next, the application of the gVEMP test in various audiovestibular disorders was discussed.
Vestibular Neuritis
Vestibular neuritis (VN) is a disorder caused by selective viral inflammation of the vestibular nerve. Halmagyi et al 39 proposed 3 clinical patterns of VN: superior VN, inferior VN, and a combined pattern involving both superior and inferior VN, accounting for the prevalence of 37.5%, 17.5%, and 45%, respectively. 40 Temporal bone histopathological study in VN donors demonstrated total or partial degeneration of the vestibular nerves and ganglia. 41 Hence, using galvanic mode to study VEMP responses may aid in determining the residual function of affected afferents in VN patients. 42
For instance, VN patients displaying absence in both galvanic cVEMP and oVEMP, it may indicate complete atrophy of the vestibular nerve, leading to the inability to induce vertigo thereafter. In contrast, VN patients who show an absent galvanic oVEMP but have a present galvanic cVEMP may indicate partial atrophy of the vestibular nerve, potentially leading to a recurrence of vertigo in the future. 43 Hence, the role of the gVEMP test in VN patients is to evaluate the affliction of vestibular afferents, assess the residual function of the vestibular nerve, and predict the likelihood of recurrent vertiginous attacks.
Herpes Zoster Oticus
Herpes zoster oticus (HZO), also known as Ramsay Hunt syndrome, is characterized by peripheral facial nerve paresis accompanied by a red, blistering rash on the ear or inside the mouth. Histopathological studies of the temporal bone in HZO patients with inner ear symptoms have revealed inflammatory lesions located in the nerve bundles within the internal auditory canal. 44 As the virus disrupts the blood-nerve barrier, it increases the permeability of the contrast agent. Consequently, gadolinium-enhanced images reveal changes in cranial nerves (CNs) VII and VIII. 45 However, the grading system of facial nerve paralysis proposed by House and Brackmann 46 fails to predict the outcome of HZO, primarily due to its oversight of the involvement of CN VIII.
The VEMP test through galvanic mode surpasses acoustic or vibratory mode in cases of HZO because it assesses afferent function. Therefore, when absent oVEMP/cVEMP by acoustic or vibratory mode occurs, subsequent oVEMP/cVEMP test by galvanic mode should be performed to precisely map the extent of lesions in CN VIII.47,48
Meniere’s Disease
A growing incidence of geriatric Meniere’s Disease (MD) was noted over the past 2 decades.49,50 Ballester et al 51 classified the geriatric MD into 2 types, de novo MD (onset after 65 years old) and long-term MD (reactivation of longstanding MD 1 year or decades before the age of 65 years). A histopathological study in a late-stage MD donor demonstrated degenerative changes in both the vestibular nerve and ganglion. 52 These findings may explain the spontaneous resolution of vertigo observed in long-term MD patients.
The gVEMP test can help distinguish between the de novo and long-term MD, particularly in elderly patients who cannot recall the onset of their symptoms (Meniere’s triad). As a result, the gVEMP test can help predict the potential relief of vertiginous episodes in long-term MD patients when an absent gVEMP response is detected. 53 Thus, the gVEMP test serves as a valuable tool for assessing residual function of the vestibular system in elderly MD patients and predicting the recurrence of vertigo.
Sudden Sensorineural Hearing Loss
Sudden sensorineural hearing loss (SNHL) is a syndrome encompassing diverse entities, arising from a variety of underlying causes. An inner ear test battery comprising audiometry, and cVEMP, oVEMP, and caloric tests has been utilized in sudden SNHL to identify its underlying etiologies and offer comprehensive insights into the affected territory in the inner ear.54,55
Iwasaki et al 56 reported that in cases of sudden SNHL with vertigo, the lesion is more frequently localized at the inner ear endorgans rather than the afferent pathways, as indicated by normal gVEMP results. Similarly, Chang et al 57 combined 3 stimulation modes to elicit VEMPs and found that patients with sudden SNHL who have normal gVEMP responses are likely to experience a higher rate of hearing recovery compared to those with abnormal gVEMP results.
Benign Paroxysmal Positional Vertigo
Benign paroxysmal positional vertigo (BPPV) is defined by short episodes of vertigo accompanied by characteristic nystagmus, triggered by specific provoking positions. Dislodged otoconia stemming from degeneration of the utricular/saccular macula yield abnormal results in the oVEMP/cVEMP test, respectively.58 -61 Chang et al 62 reported that higher abnormality rates were noted in acoustic cVEMP (62%), followed by galvanic cVEMP (36%), vibratory oVEMP (36%), and galvanic oVEMP (14%), indicating that BPPV has a lesser impact on the vestibular afferents.
Auditory Neuropathy
Auditory neuropathy is characterized by normal otoacoustic emissions or cochlear microphonic responses, yet exhibiting abnormal auditory brainstem responses. 63 Kaga et al 64 referred to this condition as “auditory nerve disease of unknown cause,” whereas Starr et al 63 coined the term “auditory neuropathy.” Subsequently, numerous analogous cases have been documented. Of them, some patients also had abnormal vestibular test results. 65
Chen et al 66 performed VEMP testing using both acoustic and galvanic stimuli in 14 patients with auditory neuropathy. They found higher rates of abnormalities in acoustic cVEMP (93%) and acoustic oVEMP (86%) compared to galvanic cVEMP (68%) and galvanic oVEMP (54%). These results suggest that patients with auditory neuropathy exhibit concurrent dysfunction in both vestibular receptors and afferents.
Bilateral Vestibulopathy
Bilateral vestibulopathy is defined as a decrease or absence of horizontal canal VOR in both ears, which can be evaluated by caloric, rotational, or video head impulse testing. 67 Patients typically exhibited instability while walking or standing, exacerbated in darkness and/or on uneven ground, or during head movements, a phenomenon termed “oscillopsia.”
Patients with bilateral vestibulopathy may exhibit abnormal cVEMP/oVEMP regardless of stimulation by either acoustic, vibratory, or galvanic mode. These abnormalities likely arise from the diversity of etiologies, which cause damage to the otolithic receptors and/or their afferents, leading to the abnormalities in VEMP response.68 -70
Aging Effect
Degenerative change in the vestibular endorgans typically begins after age 40. In addition, beyond age 60, there is a significant decline in the number of ganglion cells, with a 37% reduction in vestibular afferent neurons observed in elderly individuals. 71 Hence, prolonged p13, n23 latencies and reduced p13-n23 amplitude of galvanic cVEMP were noted in those aged >60 years, when compared with those aged 20 to 59 years. 72 Likewise, the group over 60 years had significantly longer nI, pI latencies, and smaller nI-pI amplitude when compared with those under 60 years. 73 To distinguish absent VEMP of pathological change from aging effect, using the opposite ear as a control may prove valuable.
Role of the gVEMP Test in Audiovestibular Disorders
Table 2 provides a summary of the VEMP testing using various modes in patients with audiovestibular disorders and in healthy controls, as detailed across 43 pertinent research papers. It is clear that both the cVEMP test, conducted in 38 (88%) out of 43 studies, and the oVEMP test, conducted in 32 (74%) out of 43 studies, employing acoustic and/or vibratory modes, have been widely utilized in assessing various audiovestibular disorders. However, the utilization of the galvanic cVEMP (18/43, 42%) and oVEMP (14/43, 33%) tests for evaluating audiovestibular disorders has received comparatively less focus. While the majority of audiovestibular disorders exhibit lesions localized in the inner ear endorgans, it remains uncertain whether retrograde degeneration into the vestibular afferents occurs. It is important to note that the galvanic VEMP test should not be performed as the initial test, as it bypasses the receptor level. Instead, the acoustic or vibratory mode should be performed first to elicit VEMP. If the VEMP result is absent, a galvanic VEMP test can then be conducted to assess potential issues with distal afferents. This approach allows for the assessment of residual function in the vestibular nerves and aids in predicting outcomes. 74
Listing of Various Modes of VEMP Testing Utilized in Audiovestibular Disorders and Healthy Controls.
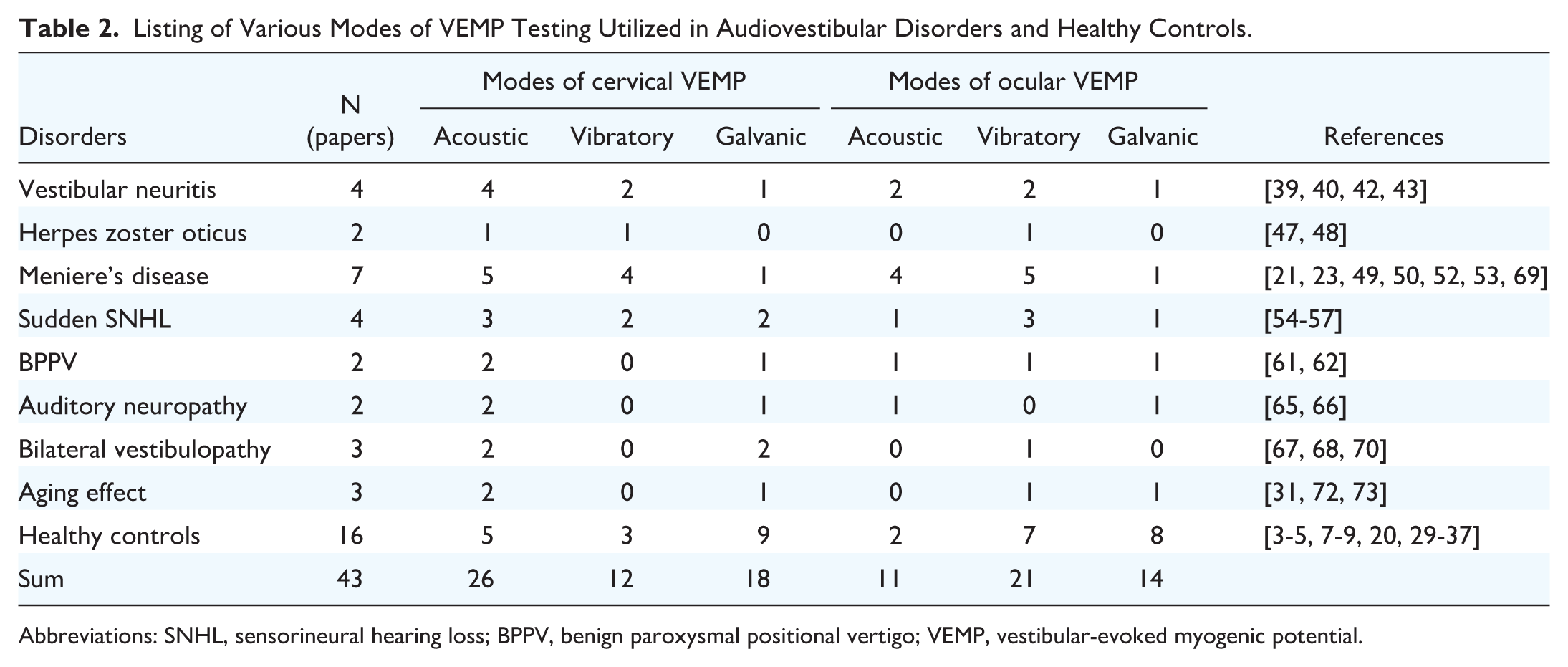
Abbreviations: SNHL, sensorineural hearing loss; BPPV, benign paroxysmal positional vertigo; VEMP, vestibular-evoked myogenic potential.
Conclusion
The ocular and cervical VEMP testing using galvanic stimuli should be accompanied by testing with acoustic or vibratory stimuli to precisely delineate the affected receptors and/or afferents in audiovestibular disorders. Clinical application of the gVEMP test in audiovestibular disorders includes: (1) Evaluating the involvement of vestibular afferents; (2) assessing the residual function of the vestibular system; and (3) predicting the outcome of audiovestibular disorders.
Footnotes
Author Contributions
Yi-Ho Young: Corresponding author, data analysis, drafting, final approval, accountability for all aspects of the work; Chih-Ming Chang: data analysis, final approval, accountability for all aspects of the work; Po-Wen Cheng: data analysis, final approval, accountability for all aspects of the work.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: National Science Council, Taipei, Taiwan (Grant no. NSTC 113-2314-B418-004), and Far Eastern Memorial Hospital (FEMH 113-2314-B418-004).
Ethics Approval
This study was approved by the institutional review board of the National Taiwan University Hospital (202111060RIND).
Availability of Data and Materials
All data and materials support the published claims and comply with field standards.