
Abstract
Background:
Tracheobronchopathia osteochondroplastica (TO) is a rare idiopathic disease with a stable course that involves the mucous membrane of the tracheobronchial tree. Most cases present no specific symptoms, and there are currently no established guidelines for diagnosis and treatment. In this report, we discuss a single case of a patient with TO who was diagnosed based on clinical imaging and histopathology.
Case Summary:
A patient with a history of smoking and alcohol consumption, but no specific clinical symptoms, was diagnosed with TO after undergoing fiber-optic bronchoscopy. Nodular processes with smooth surface mucosa and detached bronchial mucosa were observed. The presence of TO was confirmed by pathological examination.
Conclusion:
The diagnosis of TO is difficult, and early fiber-optic bronchoscopy and pathological examination should be performed to facilitate the diagnosis.
Core tip: In this case, a patient was diagnosed with miliary shadows in the lungs after undergoing chest computed tomography examination during physical examination. Lung function showed mild obstructive ventilation dysfunction. Consequently, the patient was diagnosed with tracheobronchopathia osteochondroplastica (TO) via bronchoscopy and pathological examination. At present, the detection rate of TO is very low; therefore, doctors should consider TO in clinical assessment. The diagnosis of TO is difficult, and fiber-optic bronchoscopy and pathological examination should be performed promptly to facilitate the diagnosis. Key points: Research has not yet been conducted to explore whether there is a specific genetic problem with TO tissue hyperplastic disorder.
Introduction
Tracheobronchopathia osteochondroplastica (TO) is defined as a benign airway disease of the trachea and bronchial mucosa with multiple bone or cartilage tissue nodular hyperplasia prominent to the lumen of the airway lesions. It has been reported that TO, with unknown etiology, is characterized by congenital tracheobronchial dysplasia, long-term exposure to lampblack, chronic inflammation of the tracheobronchial mucosa, metabolic disorder, physical and chemical stimulation, degeneration, endocrine hormone level, or abnormal calcium and phosphorous metabolism. 1 In this report, we discuss a single case of a patient with TO who was diagnosed based on clinical imaging, bronchoscopy, and histopathology. The purpose of this case report is to summarize the important clinical, imaging, and histopathological characteristics of the disease and to provide a basis for the development of consensus on and guidelines for TO.
Case Report
Chief Complaints
A 53-year-old man, who had undergone chest computed tomography (CT) examination revealing diffuse miliary lung shadows for a week, presented to our department.
History of the Present Illness
The patient, who had been engaged in gas welding work for more than 20 years, was referred to the hospital without cough, expectoration, shortness of breath after activity, chest pain, chest tightness and dyspnea, fever, night sweats, wasting or fatigue, hemoptysis, rash and skin lesions, pain of joint migration, deformity and dysfunction, dry eyes and mouth, facial stiffness, tolerance and emaciation, or other symptoms. Chest CT on July 2, 2018, revealed diffuse miliary lung shadows, mostly in the upper and middle lungs, with thickening of the interlobular space and solid nodules under the left pleura.
History of the Past Illness
The patient had been diagnosed with meningitis and was cured at age 12. He had a history of smoking (20 cigarettes per day for 20 years) and a history of alcohol consumption (100 g of wine per day for a total of 2 years). His family history was negative.
Physical Examination
The patient’s body temperature, respiratory rate, blood pressure, and heart rate were all within normal range. The patient presented with good spirits, good general condition, no swollen superficial lymph nodes, and clear lung sounds. No obvious dry and wet rales were observed. In addition, other physical examinations were unremarkable.
Laboratory Examination and Lung Function
Laboratory examination revealed negative results for ferritin (1866 ng/mL), while the results for liver and kidney function, blood routine, blood sugar, electrolytes, blood sedimentation, C-reactive protein, immunoglobulin A (IgA), IgG, IgE, complement C3, complement C4, serum tuberculosis antibody, urine routine, stool routine, hepatitis B and hepatitis C virus antibody, HIV, purified protein derivative test, 1,3-beta-d-glucan (G test), total IgE, respiratory tract pathogen spectrum, and hemagglutination were all within normal range. Lung function showed mild obstructive ventilation with FEV1/FVC (forced expiratory volume in 1 second/forced vital capacity) of 66.59%.
Imaging Examinations
The patient underwent chest CT examination on July 2, 2018. Imaging results revealed diffuse miliary lung shadows, mostly in the lower and middle region, with thickening of the interlobular space and solid nodules under the left pleura (Figure 1).
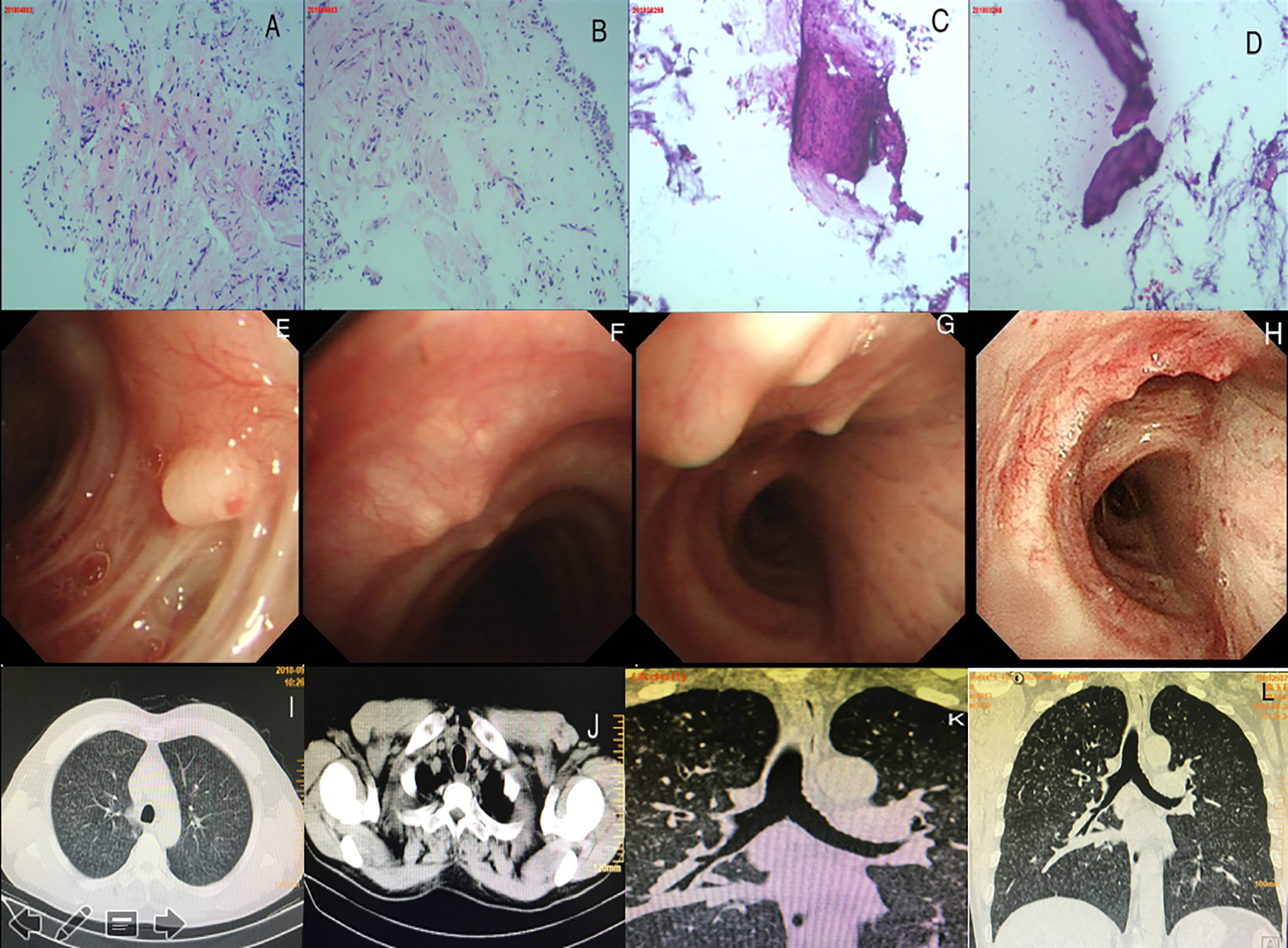
Typical characteristic images from the patient examinations. Dual images from different parts of the imaging analysis are shown in (A), (B), (C), and (D); (E) to (H) and (I) to (L). A and B, Mild infiltration of inflammatory cells. C and D, Gross view of a tissue biopsy of the diseased lesion showing presence of bone tissue. E and H, Bronchoscopy view confirming the nodular processes with smooth surface mucosa in the trachea and port of the left upper lung, left upper lobe, and right upper lobe. I to L, Computed tomography imaging results showing the diffuse miliary lung shadows, located mostly in the lower and middle regions, with thickening of the interlobular space and solid nodules under the left pleura. K, Three-dimensional reconstruction of the airway showing that the tracheobronchial membrane was smooth and multiple nodules were protruding into the lumen.
Further Diagnostic Workup
After undergoing the second chest CT examination, including 3-D reconstruction of the airway, the patient was diagnosed with scattered or multiple plaques of tubercles protruding into the lumen under the mucosa of the anterior wall of the trachea and bronchus with some calcified nodules, which accounted for the misdiagnosis. The patient was further evaluated with bronchoscopy and histopathology. The first bronchoscopy confirmed nodular processes with smooth surface mucosa in the trachea, port of the left upper lung, left upper lobe, and right upper lobe. Fiber-optic bronchoscopy biopsy in the middle and lower trachea and left upper lobe was also performed. Microscopically, the ossified tissue size 0.2 cm × 0.2 cm × 0.1 cm and detached bronchial mucosa were observed. The pathology features of these cells were consistent with the characteristics of TO. Moreover, the patient did not show signs of clinical discomfort and abnormal physical examination. Therefore, treatment was not required. When comparing the chest CT on July 2, 2018, with the chest CT on September 25, 2018, there was no change. Three-dimensional reconstruction of the airway showed that the tracheobronchial membrane was smooth, and multiple nodules were protruding into the lumen. The results of the second fiber-optic bronchoscopy were the same as those of the first one.
Discussion
The patient was diagnosed with miliary lung shadows after undergoing chest CT examination during physical examination. Smoking habits and exposure to dust and certain odors while working may be the major causes of the patient’s long-term chronic inflammatory stimulation. Lung function showed mild obstructive ventilation dysfunction. In addition, the bronchoscopy results confirmed nodular processes with smooth surface mucosa in the trachea, port of the left upper lung, left upper lobe, and right upper lobe. In addition, fiber-optic bronchoscopy biopsy in the middle and lower trachea and left upper lobe was performed. Histopathologic biopsy suggested fibrosis with ossification, with very little inflammatory cell infiltration between tissues and no bone and cartilage tissue, which may be related to the difficulty in obtaining deep tissue by performing a biopsy. Consequently, the patient was diagnosed with TO. Existing literature suggests that the positive rate of primary biopsy is only 55%, while the positive rate of secondary biopsy can reach 70%. 2 Typical pathological findings usually show fibrous tissue accompanied by ossification, very few inflammatory cells, cartilage foci or ossification foci, and even hematopoietic bone marrow infiltrating into the trachea and bronchial mucosal epithelium. 3
It has been reported that among 52 patients who underwent chest CT examination, 44 showed scattered or multiple plaques of tubercles protruding into the lumen under the mucosa of the anterior wall of the trachea and bronchus with some calcified nodules; 8 cases (including the patient in our case) showed no abnormalities in the tracheal wall but had lung inflammation. Some patients were misdiagnosed with trachea, intima tuberculosis and tuberculosis, tracheal bronchus diffuse papillary adenoma, pneumonia, trachea tumor, trachea amyloidosis, asthma, trachea stone, or right middle syndrome. Patients with tuberculosis, lung adenocarcinoma, pneumonia, and bowel cancer experienced complications. 4
This patient had been engaged in gas welding work for more than 20 years. Some of his colleagues underwent incomplete screening and did not develop the disease. Therefore, there is no proof that the disease could be associated with the patient’s occupational history. All patients diagnosed with TO have no specific clinical symptoms, such as cough, expectoration, blood in the sputum, shortness of breath after activity, fever, hemoptysis, chest pain and pharyngeal discomfort, and physical examination findings. In this case, the patient had no clinical symptoms but presented with typical TO pathology. His clinical data were not typical. However, bronchoscopy showed multiple beaded smooth nodules of different sizes (3-6 mm in diameter) protruding into the lumen of the trachea and bronchial wall, not involving the endotracheal. The imaging findings were typical.
The present case might develop into tube wall stiffness, tube cavity stenosis, or even obstructive atelectasis in the near future, 5 which is why the patient is being monitored.
Conclusion
The diagnosis of TO is difficult, and fiber-optic bronchoscopy and pathological examination should be performed promptly to facilitate the diagnosis.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.