
Abstract
Primary vocal cord aspergillosis is extremely rare in immunocompetent individuals, in whom lesions are mainly confined to the larynx, with the possibility of tracheal and bronchial infection largely ignored. In this article, we present a case of primary vocal cord aspergillosis involving the trachea and bronchus in a previously healthy 55-year-old woman. Our case highlights that vocal cord aspergillosis can involve the trachea and bronchus and that laryngoscopy alone may be insufficient to secure a comprehensive diagnosis in healthy patients presenting with hoarseness, pharyngalgia, and normal chest radiography. Furthermore, influenza B virus infection may be a risk factor for this rare disease.
Introduction
Vocal cord aspergillosis is rare, mainly occurring secondary to severe and invasive aspergillosis of the pulmonary and tracheobronchial tree in immunocompromised patients, such as those with diabetes, malignancy, tuberculosis, AIDS, or receiving long-term antibiotics, immunosuppressants, or radiotherapy.1,2 Primary vocal cord aspergillosis is even rarer in immunocompetent individuals, with case descriptions usually only describing the vocal cord lesions seen by laryngoscopy and not the distal trachea and bronchus, since these individuals have otherwise normal imaging findings. Here we present a rare case of primary vocal cord aspergillosis involving the trachea and bronchus in an immunocompetent host, which was successfully treated with itraconazole. Presenting this case—to our best knowledge the first to report primary vocal cord aspergillosis involving the trachea and bronchus in a previously healthy patient—allows us to discuss the possible etiopathogenesis of this extremely rare manifestation of the disease.
Case Report
A 55-year-old woman presented with a 10 day history of hoarseness, pharyngalgia, and dry cough. She was initially treated with a 5 day course of oseltamivir in a local hospital after nucleic acid testing for upper respiratory tract infections indicated positivity for influenza B virus. Her cough improved, but her hoarseness and pharyngalgia deteriorated. The patient was then given intravenous antibiotics for 5 days, but this failed to improve her symptoms. She was therefore referred to the otolaryngology department of our hospital for further treatment.
Laryngoscopy revealed white plaques on both her vocal cords and the initial tracheal segment, so she was referred to respiratory medicine. The patient was a housewife without any history of generalized immune deficiency, tuberculosis, diabetes, malignancy, leukemia, asthma, chronic obstructive pulmonary disease, hypertension, or other chronic diseases. She did not use any immunosuppressants or corticosteroids, and she never smoked or drank alcohol. General physical examination revealed nothing of significance. All routine blood and urine examinations were within normal limits. She was seronegative for HIV, hepatitis B virus, and hepatitis C virus. High-resolution computed tomography of the paranasal sinus and chest were unremarkable. Electronic bronchoscopy revealed irregular white plaques on the anterior half of both vocal cords, with a few plaques on the initial tracheal segment, the left main bronchus, and the right median bronchus (Figure 1).
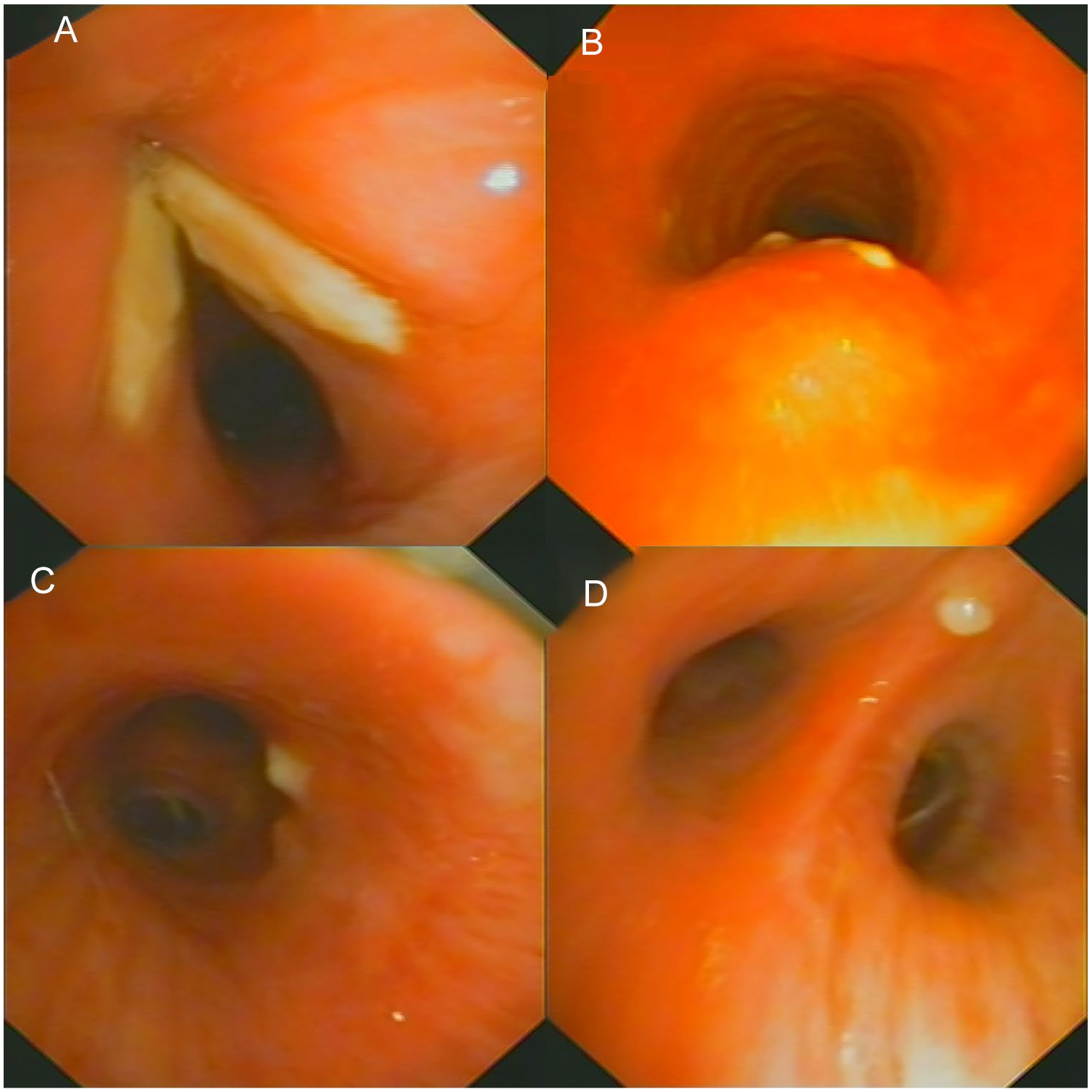
Electronic bronchoscopy images showing irregular white plaques on the anterior half of both vocal cords, with a small number of plaques on the initial tracheal segment, the left main bronchus, and the right median bronchus. (A) Glottis. (B) Initial tracheal segment. (C) Left main bronchus. (D) Right median bronchus.
The lesions were removed as completely as possible using biopsy forceps at bronchoscopy, and the obtained samples were sent for histopathological examination, which showed coagulative necrotic tissue with numerous hyphae with dichotomous branching at 45° angles (Figure 2). There was no evidence of tuberculosis or malignancy. Aspergillus fumigatus was diagnosed by next-generation sequencing of vocal cord samples. The patient was treated with oral itraconazole 200 mg once daily with instructions for vocal hygiene. After 10 days of medication, her voice significantly improved, and repeat electronic bronchoscopy identified only a few remaining white lesions on the vocal cords and none on the trachea and bronchi. Follow-up bronchoscopy 1 month later showed apparently normal vocal cords, trachea, and bronchus. The patient reported no adverse reactions to her medications.
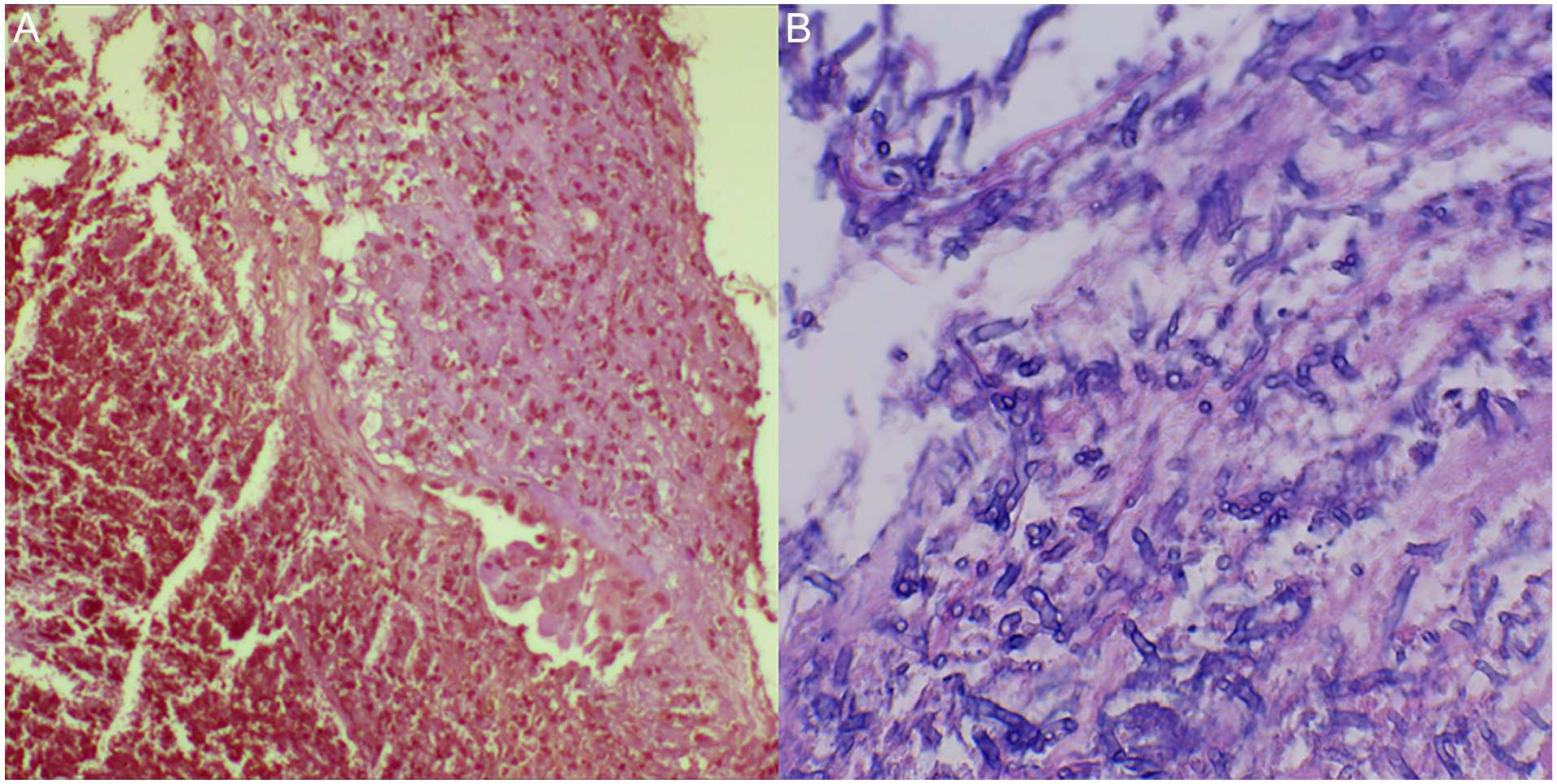
Histopathological examination of biopsy tissue showed abundant hyphae within coagulative necrotic tissue (×200), and the hyphae had septate branches at 45° angles (×400). (A) Coagulative necrosis tissue. (B) Hyphae with septate branches at 45° angles.
Discussion
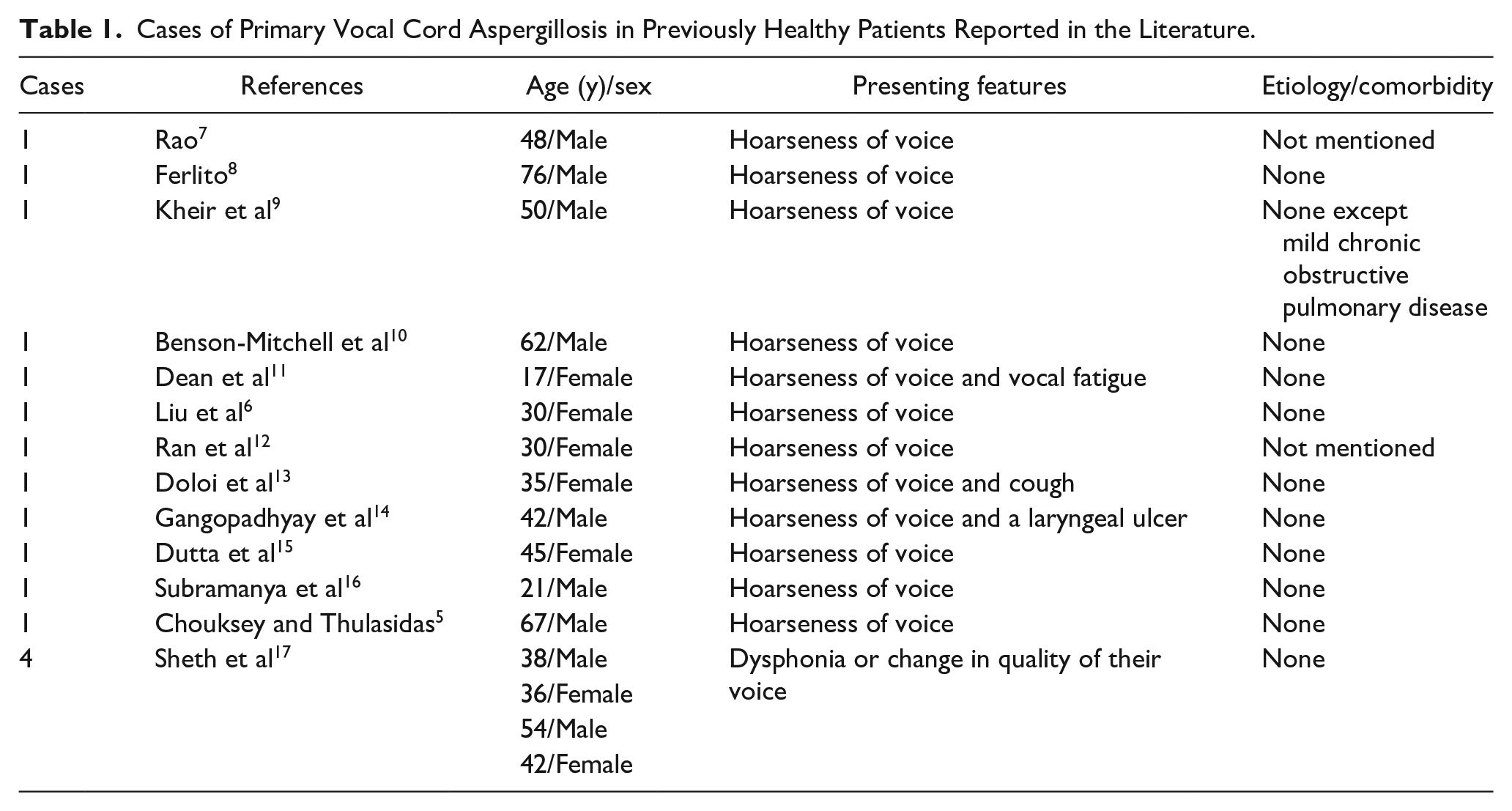
Although some cases of vocal cord aspergillosis have been reported, there remain gaps in our understanding of this rare condition. Aspergillus is usually an opportunistic pathogenic fungus of the immunocompromised. While infection can occur at various sites, primary vocal cord infection is rare, especially in immunocompetent individuals. Several factors are thought to be associated with primary vocal cord aspergillosis, including vocal cord abuse, smoking, long-term inhaled corticosteroid use,3,4 prolonged neutropenia, severe gastroesophageal reflux, laryngeal radiation, intubation-related microtrauma of the vocal cord surface,1,2 and exposure to a large amount of fungal spores. 5 Our patient had flu-like symptoms, including hoarseness, pharyngalgia, and dry cough at the early stages of the disease, which responded poorly to anti-influenza treatment. Our detailed history-taking revealed that the patient had not been unduly exposed to fungal spores (such as by cleaning an old house, touching old clothes, or visiting anywhere with a high burden of mycotic spores) before the onset of vocal cord aspergillosis. Antibiotic abuse can alter the local bacterial flora and disturb the ecological balance between bacteria and fungi, 6 thereby causing Aspergillus overgrowth but, in our patient, 5 days of antibiotic therapy did not constitute antibiotic abuse. Therefore, our case differs from all the other reported cases of vocal cord aspergillosis, where symptoms developed after prolonged corticosteroid therapy, systemic antibiotic therapy, or many years of vocal abuse. Indeed, an extensive search of the PubMed/MEDLINE database revealed fewer than 50 cases of primary laryngeal or vocal cord aspergillosis, 16 of which occurred in previously healthy subjects like our patient with no obvious predisposing factors (Table 1). However, we are the first to report that primary vocal cord aspergillosis can also involve the trachea and bronchus in previously healthy patients.
Cases of Primary Vocal Cord Aspergillosis in Previously Healthy Patients Reported in the Literature.
While vocal cord aspergillosis is nearly always secondary to severe and invasive broncho-pulmonary aspergillosis,14,18 the present case highlights that primary vocal cord aspergillosis can involve the trachea and bronchus, which prompted suspicion of bronchial and laryngeal tuberculosis until excluded by biopsy. The vocal cord lesions were the most severe, while those on the trachea and bronchus were less so. Given the characteristics of the lesion distribution and severity, it is reasonable to hypothesize that the tracheal or bronchial infections were secondary to the vocal cord aspergillosis, not vice versa. On the other hand, it may also be a disease that involves both the vocal cords and the trachea and bronchus, or the lesions at different sites are independent of each other. Even so, this is still a rare case of concern, because the concurrent tracheobronchial infection has never been mentioned in previous reports of vocal cord aspergillosis in previously healthy people. Such patients are more likely to be referred to the otolaryngology department for their pharyngeal symptoms such as hoarseness and pharyngalgia, where otolaryngologists rule out lung lesions by chest radiography and thus only usually perform laryngoscopy to investigate the disease. Although the pathoetiology of vocal cord aspergillosis can be established, this limited approach might mean that infection of the trachea and bronchus is missed. In addition, our patient tested positive for influenza B nucleic acid, and hoarseness and pharyngalgia are common symptoms of influenza,19,20 so vocal cord aspergillosis may be masked by influenza. This is especially noteworthy during the winter season when influenza, common colds, and, more recently, SARS-CoV-2are prevalent. We also speculate that if incorrectly treated, our patient’s vocal cord aspergillosis may have progressed to mycotic pneumonia, where the 2 presentations represent different stages of the same disease. Furthermore, Aspergillus has other clinical implications, producing carcinogenic compounds that may play a role in the development of lung squamous cell carcinoma and hepatocellular carcinoma by mutating codon 249 of the p53 tumor suppressor protein, although the direct role of Aspergillus in these tumors remains unclear. 21
Influenza B virus has never been reported as a predisposing factor for primary vocal cord aspergillosis in previously healthy patients. In our patient, who had no obvious known risk factors despite careful clinical and laboratory investigation, the acute upper respiratory infection caused by influenza B virus may have been responsible for the fungal colonization and invasion of the vocal cord membrane and deep tissues. Influenza B virus is a negative-sense single-stranded virus belonging to the Orthomyxoviridae family. 22 By attaching to the host cell and penetrating the membrane, influenza virus infects and damages airway epithelial cells mediated by hemagglutinin and neuraminidase encoded by its single-stranded RNA.20,23,24 Through altered neutrophil recruitment and function, diminished macrophage production, 25 and inhibition of T cell-mediated immunity, influenza virus impairs innate and adaptive host defenses.26,27 Thus, influenza virus can amplify microbial adherence and impair microbial clearance, 23 thereby increasing the likelihood of fungal infection. In addition, the respiratory tract harbors a diverse community of commensal, opportunistic, and pathogenic microorganisms.28,29 There is increasing evidence that, in addition to classic secondary infections, influenza virus interacts with other pathogens colonizing or infecting the human respiratory tract, which may alter normal colonization or infection processes. 30 We hypothesize that the vocal cord aspergillosis in our patient developed through these mechanisms, even though no studies have reported a direct relationship between influenza virus and Aspergillus.
Conclusions
Primary vocal cord aspergillosis is extremely rare and its exact etiology remains elusive. This case highlights that aspergillosis lesions may also involve the trachea and bronchus and not be solely confined to the vocal cords. Therefore, for previously healthy patients presenting with hoarseness and pharyngalgia, even if their chest radiography is unremarkable, bronchoscopy may be necessary in addition to laryngoscopy to establish whether lesions are present in the trachea and bronchi. Our case also suggests that influenza B virus infection may be a risk factor for this rare disease.
Footnotes
Acknowledgements
This work is supported by Otolaryngologist Dan Xu and Pathologist Yali Xu.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Consent
Written informed consent was obtained from the patient(s) for their anonymized information to be published in this article.