
Abstract
Introduction:
Enhanced recovery after surgery (ERAS) protocols are a series of perioperative care to optimize preoperative preparation, prevent postoperative complications, minimize stress, and speedup recovery. Tympanoplasty and mastoidectomy are common surgical procedures for chronic suppurative otitis media.
Objective:
To compare the efficacy and safety between ERAS and conventional recovery after surgery in the perioperative period of chronic suppurative otitis media.
Methods:
From April 2018 to February 2019, a total of 84 patients scheduled for tympanoplasty and/or mastoidectomy due to chronic suppurative otitis media were involved and randomly divided into the ERAS group and the control group. The patients’ preoperative anxiety, postoperative pain, and comfort level were determined by comparing the results of Self-Rating Anxiety Scale (SAS), Visual Analog Scale (VAS) and General Comfort Questionnaire (GCQ). The postoperative complications, postoperative hospital stay, and hospitalization cost were calculated.
Results:
The ERAS group showed a lower SAS score (30 [28-31.5] vs 35 [30-43], P < .05], a higher GCQ score (88 [84-100] vs 83 [78.25-92.25], P < .05), and a lower VAS score (0 [0-0] vs 1 [0-2], P < .05] after surgery. No significant difference (P > .05) was observed between the ERAS group and the control group in postoperative complications, postoperative hospitalization time, and hospitalization cost, respectively.
Conclusion:
Enhanced recovery after surgery can reduce pain and improve comfort in the perioperative period of chronic suppurative otitis media.
Introduction
Enhanced recovery after surgery (ERAS) is a series of multidisciplinary initiatives adopted in the perioperative phase to improve the perioperative patient experience and outcomes and to reduce psychological and physical stress reactions. 1 Enhanced recovery after surgery was originally described as a method for managing the patients following colorectal surgery, and its application has been gradually extended to urology, orthopedics, and gynecology surgery. Meanwhile, ERAS protocols are still being developed for otolaryngology, especially otology. Our study was designed to explore the effectiveness and benefits of ERAS protocols in patients with chronic suppurative otitis media undergoing tympanoplasty or mastoidectomy.
Methods
Ethical Approval
The study was approved by the Ethics Committee of the Third Affiliated Hospital of Sun Yat-sen University (No.[2018]02-240-01). Informed consent forms were obtained from all patients.
Participants
Eighty-four patients undergoing tympanoplasty and/or mastoidectomy in the Third Affiliated Hospital of Sun Yat-sen University from April 2018 to February 2019 due to chronic suppurative otitis media were enrolled. The participants were randomly divided into the ERAS group and the control group using a random number table. The ERAS group included 10 males and 32 females between 18 and 65 years of age with an average age of (36.7 ± 11.2) years, while the control group included 11 males and 32 females between 19 and 63 years of age with an average age of (35.6 ± 10.3) years.
Inclusion criteria: (1) Willing to accept the ERAS protocols after propaganda; (2) No mental disorder; (3) No surgical contraindication based on preoperative examination; (4) Age of 18 years old or above.
Exclusion criteria: (1) Failure to understand and cooperate with the ERAS protocols; (2) Mental disorders; (3) Serious chronic diseases such as high blood pressure, tuberculosis, and heart disease; (4) Age younger than 18.
Withdrawal criteria: In the implementation process of ERAS and the control group, failure to carry out the implementation process in accordance with the implementation scheme due to human factors and exit midway.
Protocols for ERAS Group
Preoperative treatment
The preoperative propaganda and explanation of ERAS, including the anesthesia, surgery, postoperative recovery, and preoperative psychological counseling were given to each patient in this group. If the patient had no contraindications, a nonsteroidal anti-inflammatory drug (NSAID; ie, 60 mg of loxoprofen) was administered the night before surgery to induce preventive analgesia. Before transferred to the operating room, the patients fasted for 8 hours from solids and 2 hours from fluids and had a carbohydrate drink (outfast, 300 mL or 5 mL/kg) 2 hours before surgery.
Intraoperative treatment
Short-acting sedatives and short-acting opioid analgesics were given during surgery. Local infiltration anesthesia with 5 mL/0.1 g lidocaine was applied to the opisthotic incision before surgery by the surgeon. The body temperature was monitored to avoid intraoperative hypothermia (<36 °C). The intraoperative fluid volume was also restricted. The crystalloid solution was reduced when moderate colloid fluid was given.
Postoperative treatment
Bed rest, electrocardiograph monitoring, and oxygen inhalation therapy were administered for 2 hours. A NSAID (ie, 50 mg of flurbiprofen) for preventive analgesia was given by intravenous injection at 2 hours and 12 hours postoperatively. After 2 hours, the patients were encouraged to have liquid or soft food and were allowed to increase the amount and frequency of food intake according to their gastrointestinal tract tolerance. They were also encouraged to engage in out-of-bed activities guided according to their recovery conditions.
Protocols for Control Group
Preoperative treatment
A routine presurgical explanation about operation and postoperative treatment was given to each patient in this group. Psychological counseling and antianxiety drugs were administered to improve sleep when necessary. No preventive analgesia measures were taken. According to the routine preoperative fasting guidelines, the patients fasted from both food and fluids for at least 8 hours before surgery.
Intraoperative treatment
Long-acting sedatives and opioid analgesics were given during the operation. The body temperature was not monitored intraoperatively. The fluid volume was not restricted and intraoperative infusion of crystalloid solution or colloid fluid was determined by the anesthesiologist.
Postoperative treatment
Bed rest, electrocardiograph monitoring, and oxygen inhalation therapy were given for at least 6 hours. No preventive analgesia was given after the operation except when necessary. After 6 hours, the patients were allowed to take food and fluids and engage in out-of-bed activities under guidance according to their conditions.
Observation Indices
Questionnaires
The preoperative questionnaire included the Self-Rating Anxiety Scale (SAS), while the postoperative questionnaires included the Kolcaba General Comfort Questionnaire (GCQ) and the Visual Analog Scale (VAS). The same guidance was offered. The data were collected after the questionnaires were completed.
Hospitalization data
Postoperative complications, such as nausea/emesis, dizziness, and hematoma formation, were treated and recorded once observed. The length of postoperative hospital stay and the hospitalization expenses were calculated upon discharge.
Statistical Analysis
Values were expressed as mean ± standard deviation, median (quantile) or n. The IBM SPSS v.22 statistical software package was used for data processing and analysis. Normal distributed continuous variables were expressed as mean plus standard deviation, and group differences were evaluated through independent sample t test. Otherwise, median and interquartile range and nonparametric test were used. P < .05 was considered statistically significant.
Results
Preoperative Psychological States
The ERAS group received propaganda before surgery. Then, they were informed of the detailed process of ERAS and were offered psychological counseling. Self-Rating Anxiety Scale was used to assess the patients’ preoperative psychological states. Patients in the ERAS group showed significantly improved psychological states than those in the control group (30 [28-31.5] vs 35 [30-43], Z = −4.403, P < .05; Table 1).
General Information of Patients and Recovery Indicators of the ERAS Group the Control Group in the Perioperative Phase.a
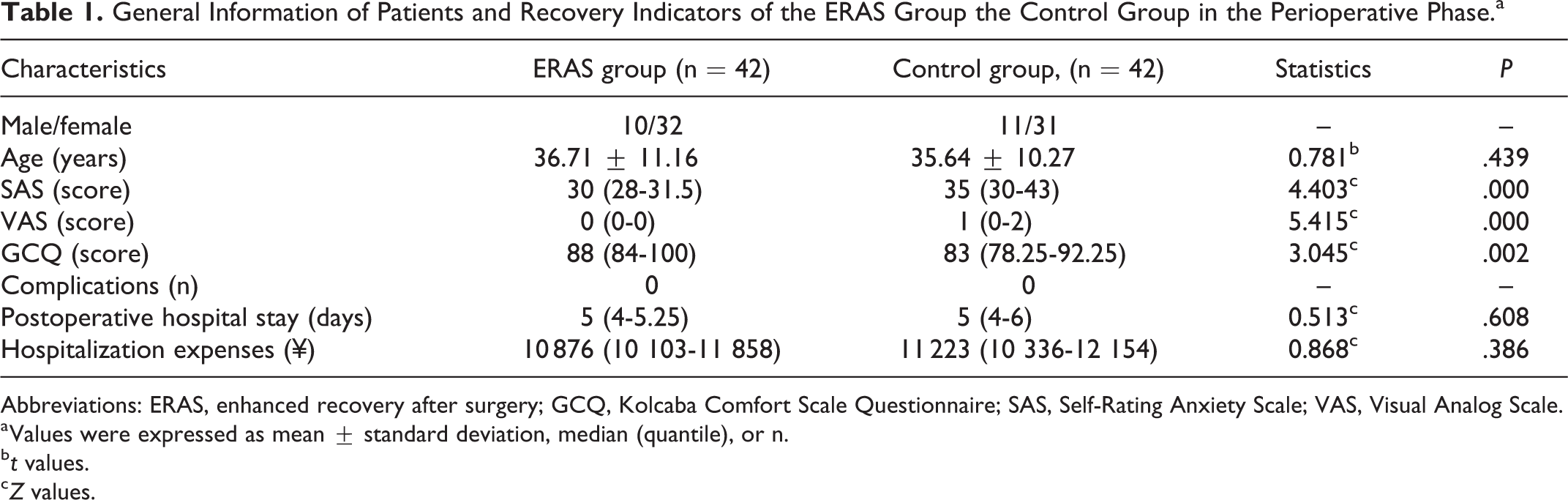
Abbreviations: ERAS, enhanced recovery after surgery; GCQ, Kolcaba Comfort Scale Questionnaire; SAS, Self-Rating Anxiety Scale; VAS, Visual Analog Scale.
a Values were expressed as mean ± standard deviation, median (quantile), or n.
b t values.
c Z values.
Postoperative Pain Level
The ERAS group received strengthened pain management and timely analgesia throughout the perioperative period. The VAS was used to evaluate the patients’ pain levels. Patients in the ERAS group experienced less pain compared with those in the control group (0 [0-0] vs 1 [0-2], Z = −5.415, P < .05; Table 1).
Postoperative Comfort Level
The ERAS group received strengthened perioperative pain management, psychological counseling, and family support. The GCQ includes physical, psychological, spiritual, sociocultural, and environmental dimensions, with a total of 28 items. The higher the score, the more comfortable the patient feels. The ERAS group showed significantly higher scores than the control group (88 [84-100] vs 83 [78.25-92.25], Z = −3.045, P < .05; Table 1).
Postoperative Complications
After bed rest with electrocardiograph monitoring and oxygen inhalation therapy for 2 hours, the patients in the ERAS group were encouraged to engage in out-of-bed activities and enjoy soft and warm food according to their recovery status. In contrast, the control group received traditional postoperative treatment. Complications such as nausea/emesis, hematoma formation, aspiration pneumonia, and dizziness may occur during this period. In this study, no complication was observed in both groups (Table 1).
Length of Hospital Stay and Hospitalization Expenses
There was no significant difference between the ERAS group and the control group in the length of postoperative hospital stay (5 [4-5.25] days vs 5 [4-6] days, Z = −0.513, P > .05). The hospitalization expenses of the ERAS group and control group were ¥10 876 (10 103.25-11 858.25) and ¥11 222.5 (10 336.25-12 154; Z = 0.868, P > .05), indicating no significant difference between both group (Table 1).
Discussion
The concept of ERAS was pioneered by Kehlet in Denmark in the 1990s and aims at faster recovery and shorter hospital stay, as well as improved patient’s sense of well-being. 1 Although the contents of different fast track programs vary, common factors include the individualized preoperative propaganda, introduction of short-acting anesthetic, optimal pain management, and aggressive postoperative rehabilitation, which includes early oral nutrition and ambulation. Several studies have indicated that the implementation of ERAS protocol can accelerate recovery and reduce postoperative complications, thus shortening the length of hospital stay.2,3
Recently, the applications of ERAS protocols have been extended to head and neck oncological patients undergoing surgery,4-7 functional endoscopic sinus surgery, 8 as well as tonsillectomy and adenoidectomy in children. 9 However, the application of ERAS in tympanoplasty and mastoidectomy for chronic suppurative otitis media has not been reported previously. According to the different types and stages of chronic suppurative otitis media, tympanoplasty or mastoidectomy is appropriately selected to remove the lesion and to preserve or improve hearing. The anxiety regarding the uncertainty of postoperative hearing improvement and the pain resulting from postoperative incision can easily affect postoperative recovery and prolong the length of hospitalization. In this study, the implementation of ERAS can help alleviate the anxiety of patients and reduce postoperative pain.
The patients’ experience varied degrees of anxiety and fear due to preoperative concerns about the risks of surgery and anesthesia, which will induce adverse stress reactions and affect postoperative recovery. Previous studies have shown that the patients’ understanding of perioperative pathophysiology and effective implementation of nursing programs can reduce surgical stress. 10 In addition, individualized education in the perioperative period can greatly affect the effective implementation of ERAS. 11 In this study, ERAS propaganda was given to the patients before the operation to explain the pathophysiological process of the disease. Meanwhile, preoperative anesthesia, postoperative pain relief, and minimally invasive methods were introduced in the operation. Personalized comfort was given to alleviate the anxiety and tension of the patients. SAS, which is suitable for adults, is a self-assessment tool for analyzing patients’ anxiety symptoms. The main statistical index of SAS is the total score, which is calculated by adding up the scores for 20 items. The higher the total score, the more severe the symptoms. Based on the preoperative SAS score, the ERAS group was found to have less preoperative anxiety than the control group.
Under traditional anesthesia, the patients need to fast for longer than 8 hours preoperatively and for 6 hours postoperatively. For selective operation patients, long ban diet may lead to adverse reactions such as thirst, hunger, anxiety, and hypoglycemia, greatly reducing the comfort levels and inducing metabolic stress state in the patients. The application of ERAS can optimize the plan and shorten the fasting time so as to promote the recovery of gastrointestinal function and reduce the stress response due to hunger. More and more studies have shown that a small amount of liquid diet 2 hours before surgery does not increase the risk of adverse reactions including intraoperative reflux and aspiration.12,13 No increase in postoperative complications was found in this study. Early postoperative feeding is a key factor for assessing the effectiveness of ERAS. 14 Enhanced recovery after surgery can optimize the preoperative intestinal preparation and postoperative intestinal recovery. In our study, patients in ERAS group fasted for 8 hours for solids and 2 hours for fluids preoperatively and were given a carbohydrate drink 2 hours before the surgery. Intake of oral liquid or soft food is encouraged 2 hours after surgery according to the patient’s conditions. Through those improvements, ERAS can effectively alleviate the starvation, improve the irritability and anxious mood before and after surgery, promote the early recovery of gastrointestinal function, and increase the postoperative comfort level of the patients.
Incision pain and pressure dressing tenderness are the main sources of postoperative pain following middle ear tympanotomy or mastoidectomy. Perioperative pain management represents an important subject in medical research and an important embodiment of humanism. Perioperative multimode analgesia is an important measure of ERAS. 15 This study included preoperative application of oral nonsteroidal analgesics, intraoperative local infiltrative anesthesia, and regular postoperative use of nonsteroidal analgesics. Analgesics were administered throughout the perioperative period, and the traditional on-demand analgesics were replaced by timely analgesics. The VAS was used to evaluate the degree of pain. Numbers from 0 to 10 represented the degree of pain (ranked as 0 no pain, 1-3 mild, 4-6 moderate, and >6 severe). In this study, the VAS pain score of the ERAS group was lower than that of the control group, and the difference was statistically significant. The pain management lowered the pain level. Effective pain control can enable the patients to access early oral nutrition and ambulation. The early postoperative ground activities are also key factors in judging the ERAS effect.14,16 Early ambulation can reduce complications such as pressure sores, limb venous thrombosis, and hypostatic pneumonia, while promoting the recovery of gastrointestinal function.
The original intention of the ERAS concept is to accelerate postoperative rehabilitation of patients, so as to shorten the length of hospitalization and reduce the cost of hospitalization. However, the ERAS group and the control group showed no significant difference in postoperative complications, total hospital stay, and hospitalization costs. This finding may be due to the fact that tympanoplasty and mastoidectomy are relatively mature and associated with less postoperative adverse reactions and short postoperative hospital stay. At the same time, there may be some problems regarding the utilization rate and turnover rate of wards, leading to reduced intergroup differences. Although the promotion of ERAS in multiple disciplines and fields does not result in significant shortening of hospitalization time and reduction in hospitalization cost, more attention should be focused on the comfort level and psychological and emotional states of patients during hospitalization. Enhanced recovery after surgery has entered a new era, which should be extended to minimally invasive surgery. In minimally invasive surgery, the pain management and emotional state of patients during their hospitalization should be paid more attention to.
Conclusions
In conclusion, the application of ERAS in the perioperative period of chronic suppurative otitis media can optimize the surgical scheme, shorten the fasting time, reduce the pains, and increase the postoperative comfort of the patients. In the meantime, no complication was found. However, individual differences should be considered in the implementation of perioperative accelerated rehabilitation programs to avoid stereotyping. Therefore, additional clinical data and longer postoperative follow-up are still needed for more comprehensive evaluation.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Science and Technology Program of Guangzhou [201803010093] and the Special Cultivation Project of Sun Yat-sen University [2018122819965].