
Abstract
Objective:
The presence of clinically detectable papillary thyroid carcinoma (PTC) metastases in the lateral neck is an indication for neck dissection (ND) and thyroidectomy. Although there is a consensus regarding the importance of therapeutic selective ND of involved levels II to IV in patients with clinically evident locoregional metastatic disease, the prognostic benefit of level V prophylactic ND remains debatable.
Methods:
All patients who underwent thyroidectomy with ND for metastatic PTC between 2006 and 2019 were included in a single-institution retrospective study. Preoperative characteristics at initial presentation, imaging workup, intraoperative findings, and the final histopathological reports were retrieved from the institutional database.
Results:
A total of 189 patients with locally advanced PTC were identified, of whom 22 (11.6%) patients underwent therapeutic selective ND at levels II to IV together with level V dissection due to clinical involvement. Comparison of the patients who were operated on level V to those who were not revealed no significant difference. The disease recurrence rate was 20.1% throughout an average follow-up of 5.1±3.1 years. No significant differences in recurrence rate were found between patients who underwent and those who did not undergo level V ND (22.7% vs 19.8%, P = .648). No recurrence at resected level V was detected during follow-up, while recurrence at level V was found in 4 (2.1%) patients who did not undergo level V dissection. Evidence of macroscopic and microscopic extrathyroidal extension was significant predictors of disease recurrence risk.
Conclusion:
There were no significant associations between level V dissection and risk for recurrence. Recurrence at level V was rare (4/189 patients, 2.1%). Our study’s findings suggest a low prophylactic benefit of an elective level V ND. Elective level V ND should not be done routinely when lateral ND is indicated but should rather be considered after careful evaluation in high-risk patients.
Keywords
Introduction
The presence of clinically evident metastases in the lateral neck among patients with papillary thyroid carcinoma (PTC) correlates with higher rates of disease recurrence 1 and mortality, 2 therefore necessitating extensive surgical intervention consisting of a thyroidectomy with therapeutic neck dissection (ND) 3 followed by adjuvant treatment with radioactive iodine. 4 However, the extent of the lateral ND remains controversial. 5 On the one hand, removal of all metastatic tissue seems to improve postoperative iodine ablation and has been shown to reduce recurrence and mortality rates. 6,7 On the other hand, the extent of ND correlates with postoperative complications, gravely impacting patients’ quality of life, 8 most notably due to the risk of intraoperative injury to the spinal accessory nerve 9 and causing frozen shoulder syndrome. 10
There is ongoing debate over the benefits of elective dissection of level V lymph nodes (LNs). The literature mostly addresses issues about the rate of occult metastases at level V. In the past 2 decades, the reported findings of many centers have reflected a wide range of level V involvements. In a meta-analysis by Eskander et al 11 that included 18 studies and the findings on 1298 comprehensive ND (levels II-IV or II-V), the involvement rate of level V was 25.3% compared to the involvement rates of levels II, III, and IV (53.4%, 70.5%, and 66.3%, respectively). Interestingly, the level V involvement rate was highly variable in the different studies included in that meta-analysis, ranging from 15% to 53%. 11 Centers that reported a high-level V involvement prevalence rate of occult metastasis, such as the M.D. Anderson Cancer Center, Texas, USA (53%) 12 and Johns Hopkins University School of Medicine, Maryland, USA (40%) 13 claimed that a comprehensive elective level V ND is routinely necessary. Other studies that reported much lower rates of level V involvement, such as the Regina Elena National Cancer Institute, Italy (8%) 14 and the West China Hospital, Sichuan University, China (12.3%) 15 recommended level V ND only therapeutically, based on preoperative evaluation of disease extensiveness, in order to avoid potential operative complications.
The guidelines have followed a more conservative trend over the past few decades, in favor of less extensive thyroidectomy and ND. 16 This trend is reflected in the American Thyroid Association (ATA) guidelines for adult patients with thyroid nodules and differentiated thyroid cancer. In 2012, the ATA guidelines 17 specified level Vb elective dissection alone, corresponding to the findings by Kupferman et al. 12 Interestingly, the 2015 ATA guidelines recommend therapeutic dissection to level V without a clear recommendation regarding the extent of the routine selective NDs of levels II to VI. 5
In order to tailor an optimal personalized treatment, several studies sought possible predictors for level V involvement. Yang et al 15 examined 220 patients with PTC who underwent selective II to IV ND that included level V and showed that the only predictor for level V LN metastasis in a multivariate analysis was contralateral central LN metastasis. Wang et al 18 reported additional predictors and proposed a normogram for assessing the necessity of elective ND. The following parameters were found to be significant predictors for level V metastasis among patients who underwent a lateral ND: unilateral central LN metastasis and positive LNs in levels II/III/IV, extranodal extension, and LNs larger than 2 cm. These were all independent predictive factors for recurrence at level V among patients who underwent ND that included levels II to V.
The clinical implication of an elective level V ND in terms of decreasing recurrence rate is rarely discussed. We did not find any reports on parameters that can be used as predictive factors for level V disease recurrence and thus may mandate a more extensive dissection. The main aim of this study is to assess the recurrence rate to level V among patients who underwent therapeutic levels II to IV ND, without prophylactic level V dissection. This study assessed the rate of recurrence in level V among patients undergoing a therapeutic selective II to IV ND with a therapeutic level V ND and patients undergoing a therapeutic selective II to IV ND without a level V ND. We also aimed to identify unique characteristics of patients that required a therapeutic level V ND so that they can be used as additional assessment tools when evaluating the required extent of treatment.
Materials and Methods
Study Design and Patient Population
This study is a retrospective cohort study. All patients who underwent thyroidectomy and ND with a final diagnosis of PTC at the Tel-Aviv Sourasky Medical Center (TLVMC) between January 1, 2006, and December 31, 2019, were retrieved from the institutional electronic database. Data on initial preoperative presentation, including demographic data, clinical and physical examination findings, preoperative imaging (ultrasound [US], fine-needle aspiration [FNA], computed tomography [CT], magnetic resonance imaging [MRI], positron emission tomography [PET]), as well as intraoperative findings, postoperative final histopathology reports, adjuvant treatments, and long-term follow-up, were extracted.
Institutional research ethics board approval was obtained (IRB: TLV-0704-16). Inclusion criteria were PTC diagnosis with local neck metastasis upon initial presentation, a total or a subsequent completion thyroidectomy including ND, and a follow-up duration longer than 3 months at the otolaryngology and/or endocrinology departments at the TLVMC. Exclusion criteria were insufficient follow-up (fewer than 3 months), lack of neck metastasis upon initial presentation, tumors other than PTC, and lack of histopathological or surgical reports.
Selective therapeutic II to V ND extent was documented according to the current ATA guidelines at the time of surgery and based on the anatomical description as recorded on the operative report. No prophylactic lateral NDs were performed. Complimentary treatment was considered for all patients, except for those who refused treatment or were not found suitable candidates due to their medical background. Remission was determined according to clinical presentation, physical examination, US of the neck (with FNA when indicated), and thyroglobulin (Tg) levels. Disease recurrence was defined by either elevated serum Tg levels (Tg > 20), evidence of structural recurrence by US, an FNA positive for malignancy or for Tg, or malignancy histopathology in revision ND.
Statistical Analysis
Categorical variables are presented as numbers and percentages. Continuous variables were evaluated for normal distribution using a histogram and Q-Q plot. Data with normal and near-normal distributions are presented as mean ± SD, and those with non-normal distributions as median and interquartile range (IQR). The compression of categorical variables between the 2 groups was by the χ2 testor Fisher exact test. Continuous variables were compared with the independent samples t test or Mann-Whitney U-test. Kaplan-Meier curves were used to describe disease recurrence and mortality during the follow-up period, and the log-rank test compared between groups. The multivariate Cox regression evaluated the association between groups and the studied outcomes. The forward stepwise method was applied for the variables such as sex, age at surgery, subjective dyspnea, subjective hoarseness, dysphagia, familial history of thyroid malignancy, radiation exposure, smoking, preoperative US/FNACT/MRI/PET-CT performance and findings, vocal cord hypomobility, LN metastasis on imaging, intraoperative impression of extrathyroidal extensions (ETEs) to various anatomic subsites, histopathological findings such as vascular invasion & perineural invasion, multifocality tumor size LN ratio, I131 treatment dosage, and other treatment such as external radiation beam treatment and were considered for inclusion in the regression. A P value <.05 was used as criteria for inclusion. All statistical tests were 2 sided, and a P value <.05 was considered to indicate significance. SPSS software was used for all statistical analyses (IBM SPSS Statistics for Windows, version 25).
Results
Records of all 1719 patients who underwent thyroidectomy at the Otolaryngology, Head & Neck Surgery Department at the TLVMC between January 1, 2006, and December 31, 2019, were retrospectively reviewed. A total of 249 patients were diagnosed as having locoregional neck metastatic PTC upon initial presentation, for which they underwent total thyroidectomy with ND, and 189 of those patients met study inclusion criteria. Our cohort included 72 (38.1%) males and 117 (61.9%) females, with a mean ± SD age of 46.8 ± 17.7 years (median: 45.6, IQR [32.8-60.6], range 12.8-85.9 years). The mean follow-up period was 5.1 ± 3.1 years (median: 4.52 [2.62-7.33], range 0.33-13.05 years). Surgical treatment of the neck required therapeutic lateral and central compartment ND in 100 (52.9%) cases, therapeutic lateral ND alone in 55 (29.1%) cases, and central compartment ND in 34 (18%) cases (Table 1).
Comparison of Patients Who Underwent Selective II to IV Neck Dissection With Therapeutic Level V Neck Dissection and Patients Who Underwent Selective Therapeutic II to IV Neck Dissection Who Did Not Undergo Therapeutic Level V Dissection (N = 155).a
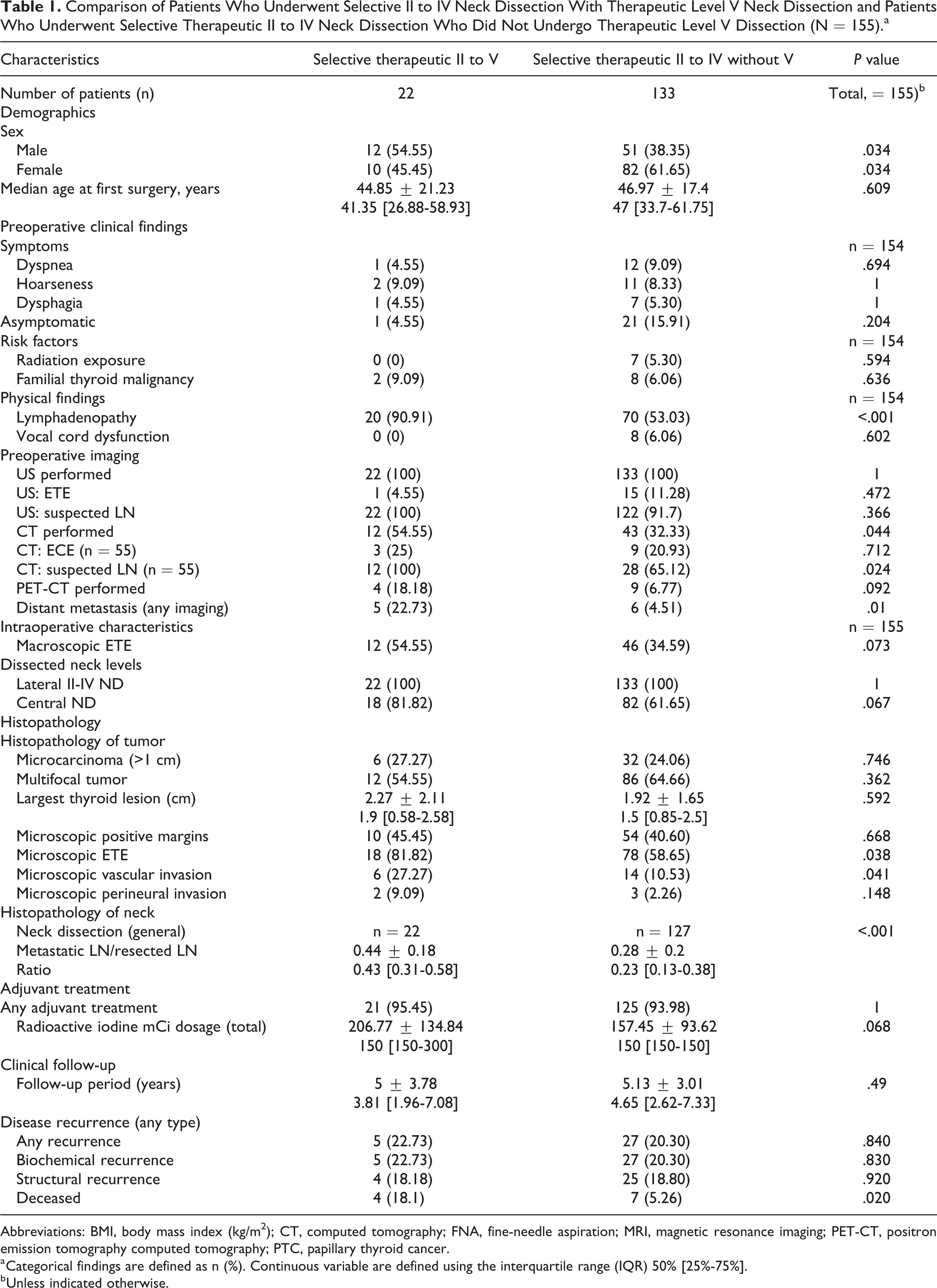
Abbreviations: BMI, body mass index (kg/m2); CT, computed tomography; FNA, fine-needle aspiration; MRI, magnetic resonance imaging; PET-CT, positron emission tomography computed tomography; PTC, papillary thyroid cancer.
a Categorical findings are defined as n (%). Continuous variable are defined using the interquartile range (IQR) 50% [25%-75%].
b Unless indicated otherwise.
In order to define the unique characteristics of patients with clinical involvement of level V, we compared the characteristics of the patients who underwent a level V ND to those of the patients who required a selective therapeutic II-IV ND and also to those of the entire cohort of patients with advanced locoregional disease (data not shown). We selected the patients with II to IV compartment locoregional disease as representing a more appropriate cohort for comparison to those with level V involvement; thus, the following results will pertain to these groups.
Of the 155 patients who underwent a selective therapeutic II to IV ND (with and without central compartment ND), 133 (85.8%) patients did not undergo a level V dissection and 22 (14.2%) patients underwent a therapeutic ND that included level V. Of the latter, 20 (90.9%) patients required a unilateral ND and 2 (9.1%) patients required a bilateral ND. Of the 22 patients who underwent a therapeutic level V ND, 12 (54.5%) were males and 10 (45.5%) were females, with a mean age of 44.9 ± 21.2 years (median: 41.4, IQR [26.9-58.9], range: 16.5-81.6 years). The mean follow-up period was 5 ± 3.8 years (3.8 [1.9-7.1], range: 0.8-13 years; Table 1).
Of the 133 patients who underwent a selective therapeutic II to VI compartment ND without therapeutic level V dissection, 51 (38.4%) were males and 82 (61.6%) were females, with a mean age of 46.97 ± 17.4 years (median: 47 [33.7-61.75], range 13.1-84.7 years). The mean follow-up period was 5.1 ± 3 years (median: 4.65 [2.625-7.335], range 0.33-13.04 years; Table 1).
Group differences in when comparing the initial presentation and demographic characteristics, gender holds a level of significance, with 54.5% of patients who underwent a level II to IV selective therapeutic ND, with a level V ND being males compared to 38.35% of the patients who did not require a therapeutic level V ND (P = .034). No other demographic characteristics (including age) or subjective complaints at initial presentation were significantly different. The preoperative physical examination findings at initial presentation of palpated neck region lymphadenopathy were recorded in significantly more patients who required a therapeutic level V ND (90.9% compared to 52.6% of patients who underwent a lateral ND without a level V ND, P = .001).
The patients who required a therapeutic level V ND underwent more CT scans as part of their preoperative assessment (54.5%) than patients who underwent a lateral ND without a level V ND (32.3%; P = .004). Distant metastases upon initial presentation were more frequent in the group of patients who underwent a therapeutic level V ND (22.7%) compared to those who underwent a selective therapeutic II to IV ND without a level V ND (4.5%; P < .01). There were no significant group differences in the rates of intraoperatively detected extrathyroidal macroscopic extension (Table 1).
There was a higher rate of microscopic ETE among patients who required a therapeutic level V ND (81.8% compared to 58.6%, P = .038). There was also a higher rate of vascular invasion among patients who required a therapeutic level V ND (27.3% compared to 10.5%, P = .041). The average number of resected LNs was not significantly higher among patients requiring a therapeutic level V ND (32.8 ± 21.2; median: 26 [20.75-40.25]), compared to those who did not (29.45 ± 15.67; median 28 [17.5-40.5]; P = .384). There was a significantly higher rate of metastatic LNs in patients who required a therapeutic level V ND (14 ± 9.2; median:12 [7.5-19.3]), compared to those who did not (7.9 ± 8.3; (median 6 [2-11.5]; P < .001), and a corresponding significantly higher ratio of metastatic to resected LNs among patients who required a therapeutic level V ND (0.4 ± 0.2; median 0.4 [IQR: 0.3-0.6]), compared with 0.3 ± 0.2 for those who did not (median: 0.2 [IQR: 0.1-0.4]; P < .001). No significant group differences were found in terms of adjuvant treatment with I131, including treatment dosage (Table 1).
Disease recurrence occurred in 5 (22.7%) of the 22 patients who required a therapeutic level V ND, and 4 (18.2%) of them had a structural recurrence. None of the recurrences involved level V. Recurrences to level V were sustained by 4 (3%) of the 133 patients who underwent a selective II to IV ND without a level V ND. Three of those patients were treated with I131 and did not require a level V revision ND (1 of them underwent a revision level V ND at another institute). None of the patients had a level V seroma or accessorial injury.
We performed a Kaplan-Meier curve in order to compare recurrence rates between patients who did and did not require a therapeutic level V ND. The Kaplan-Meier curve showed no significant difference between them in overall disease recurrence rates (Figure 1) and biochemical and structural recurrences (Figures 2 and 3). We performed an additional multivariate analysis in order to detect the prognostic implications of a therapeutic level V ND and it showed that a therapeutic level V ND (P = .422) was not a predictor for worse outcome. Interestingly, symptoms of dysphagia, intraoperative characteristics of a macroscopic ETE, and histopathological findings of microscopic perineural invasion (P = .037) were all found to be significant risk factors for disease recurrence (HR: 2.75, 3.69, and 2.49, respectively; Table 2).
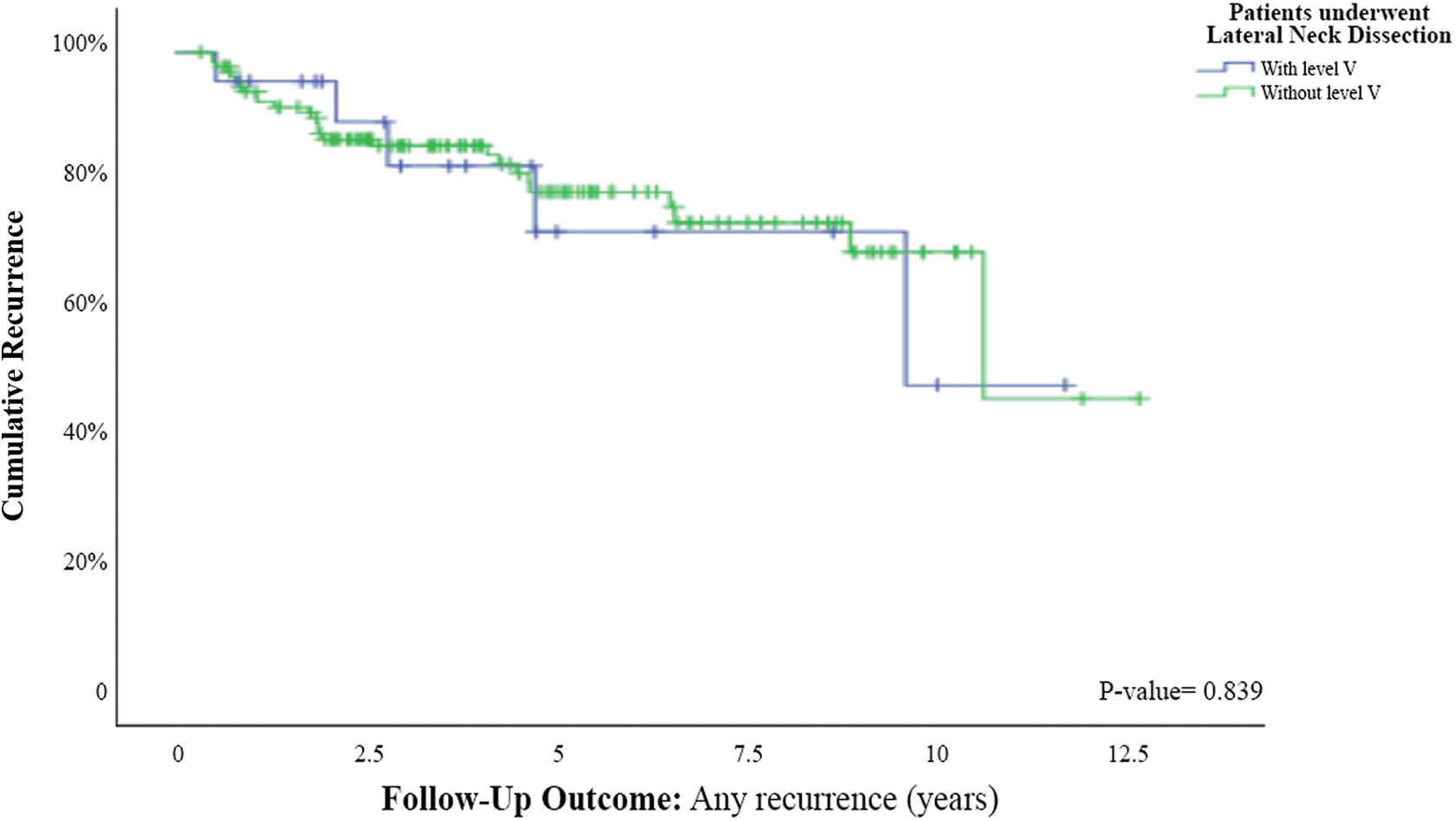
Kaplan-Meier curve for recurrence (biochemical and structural) among patients who underwent lateral neck dissection with or without level V neck dissection.
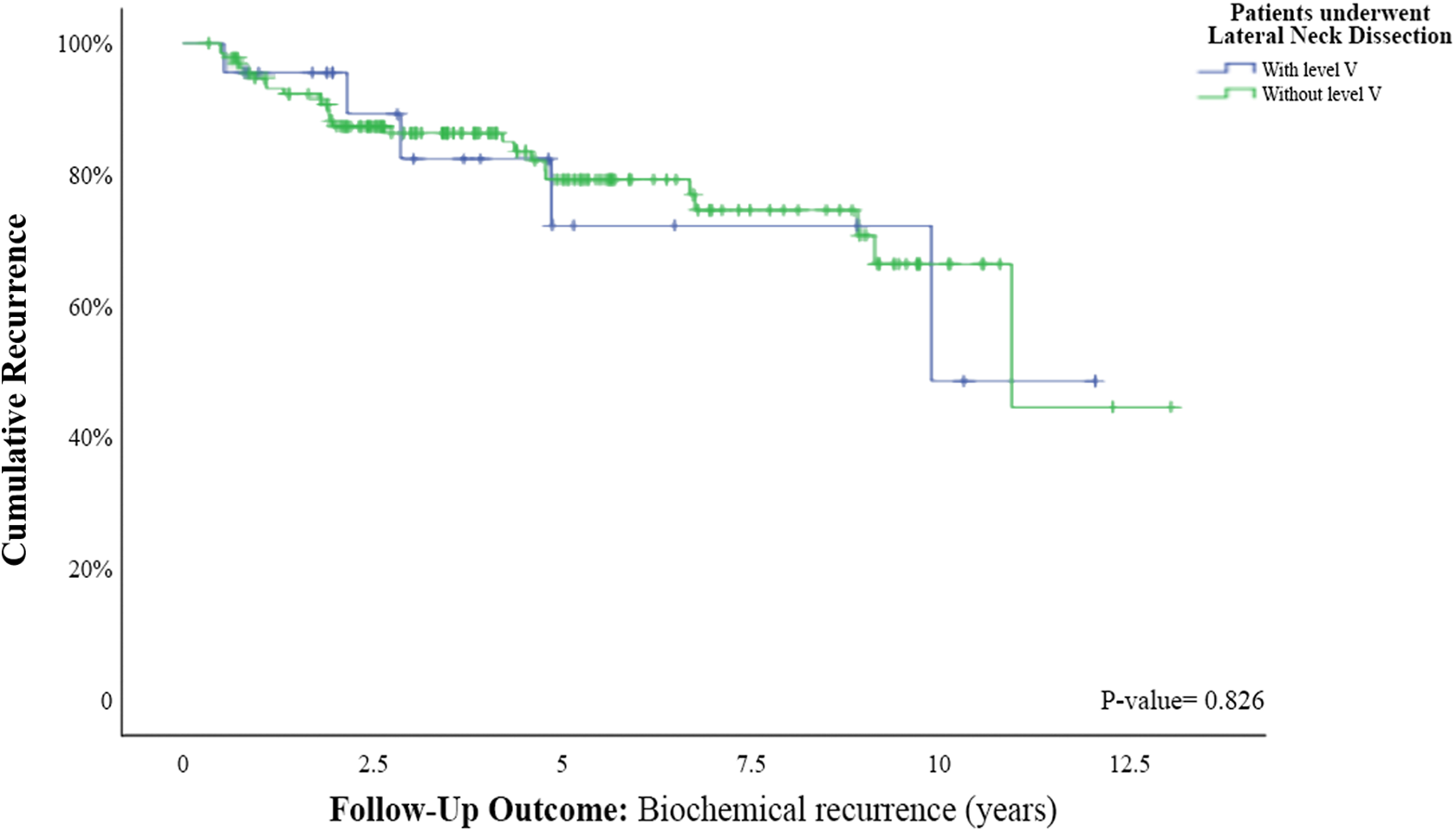
Kaplan-Meier curve for biochemical recurrence among patients who underwent lateral neck dissection with or without level V neck dissection.
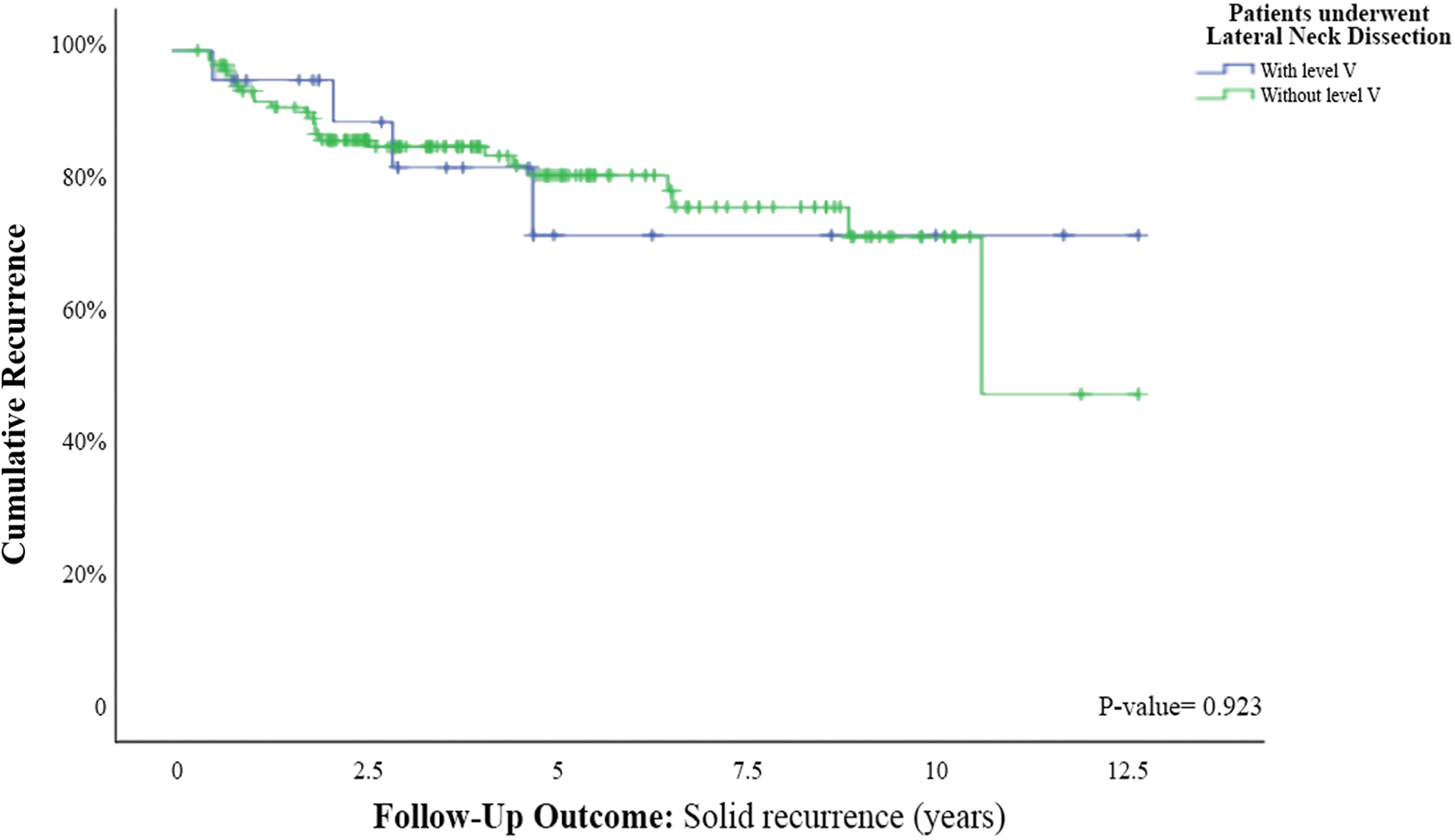
Kaplan-Meier curve for structural recurrence among patients who underwent lateral neck dissection with or without level V neck dissection.
Cox Regression and Multivariate Analysis: Predictors (Clinical, Preoperative Evaluation, Intraoperative Findings, and Histopathological Findings) for Risk of Recurrence (N = 155).
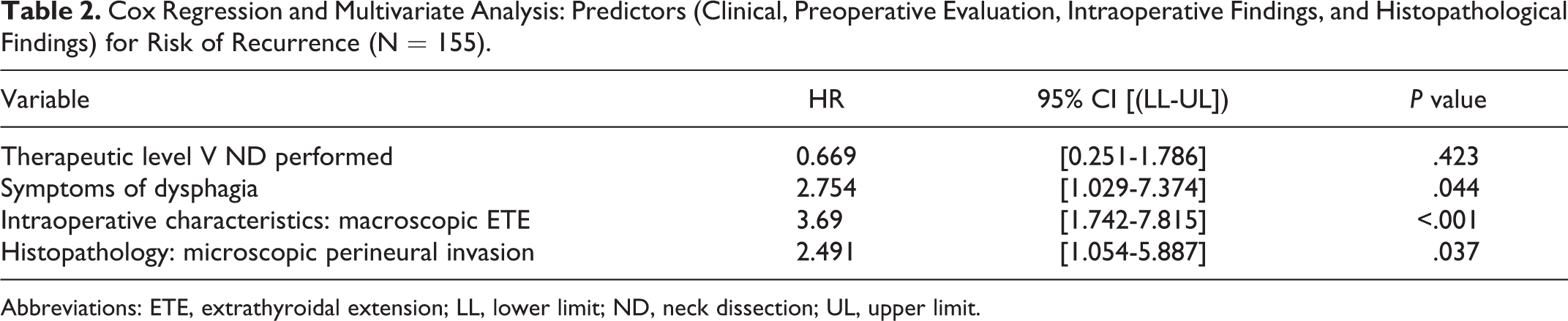
Abbreviations: ETE, extrathyroidal extension; LL, lower limit; ND, neck dissection; UL, upper limit.
Discussion
The prognostic benefit of a level V prophylactic ND in patients with PTC continues to be a matter of controversy. Our study included 155 patients who underwent total thyroidectomy and a therapeutic ND due to advanced locoregional disease and otherwise met study inclusion criteria. Twenty-two (11.6%) patients required a therapeutic level V ND, and they differed from those who did not in several characteristics: significantly more males, more patients with palpable lymphadenopathy at initial presentation physical examination, more patients who underwent preoperative CT imaging studies, and more patients who had distant metastasis upon initial presentation (Table 1). As for their tumor histopathological characteristics, more patients who underwent total thyroidectomy and a therapeutic ND had microscopic ETE and vascular invasion, increased numbers of resected LNs, and a higher metastatic LN and LN ratio as would be expected due to the larger volume of their NDs. They did not differ in recurrence rates, provision of adjuvant therapy, or length of follow-up. Examination of the pattern of recurrence to level V revealed that only 4 (2.4%) patients who underwent a therapeutic selective II to IV ND without level V ND sustained a recurrence. Unlike the findings in previous studies, 19 our multivariate analysis showed that level V metastases were not a significant risk factor for disease recurrence (Table 2).
The trend of PTC management is toward a more conservative approach in an attempt to avoid possible surgical complications. The risk for spinal accessory nerve injury, for example, should be taken into account when considering a level V ND. 16 The question of whether to routinely perform a level V prophylactic ND or not has not been conclusively resolved in the current guidelines, which still include level V along with the lateral II to IV traditional ND. This issue may be addressed by number approaches. The majority of studies cite the rates of microscopic metastases in level V as reported in centers that used to perform routine level V ND and those rates ranged between 5.7% and 34.5%. 20,21 A meta-analysis by Eskander et al 11 concluded that the involvement of microscopic metastasis to level V was 25.3% (range: 15%-53%). Kupferman et al12 showed a high rate (53%) of microscopic nodal involvement of level V, and they reported that the majority of the involved nodes were found at level Vb.
Studies that focus on correlations between predictors of clinically evident disease in level V and preoperative predictors and patient characteristics are scarce. One might aim to assess the extent of selective II to IV ND to level V via utilizing “off-label” the ATA risk-stratification scheme, claiming that evidence of lateral neck metastasis is considered to be a disease recurrence predictor. However, the system is referring only to LNs size and number, while the involved nodes’ location does not play any clear role. 5
Interestingly, the literature is conflicting regarding the pattern of lymphatic spread to level V. Some studies emphasize the roll of level IV, while others do not support such concept. 22 Previous studies have shown that the pattern of spread of PTC metastasis in the neck is not necessarily linear nor continuous. The involvement of level V does not necessarily come directly after involvement of level IV. Level V can also be involved when level IV is spared, while only levels II to III or only level III are involved. 5,23 Thus, according to the recent ATA guidelines, levels II to IV are considered one compartment and most surgeons operate on this compartment as one unit when indicated, such as in the case of metastases to 1 or more of the levels II to IV, and this dissection is considered a therapeutic lateral ND. 4,5,23 In a normogram performed for level V recurrence, Wang et al 18 demonstrated level II/III/IV metastasis found to be independent predictive factors for level V metastasis (P < .05). Interestingly, this statistical model calculated the specific contribution of each level metastases, and the lateral compartment was found significant contributor. However, no specific contribution was found to be a robust predictor of level V involvement.
Several studies have raised concerns about the capability of preoperative US to detect a level V metastasis, 24,25 thus pointing to the need to provide additional assessment tools for guiding decision-making with regard to the extension of an ND. However, current studies disagree about the predictive value of level V microscopic involvement, and the question about the clinical significance of that involvement is seldom discussed. Xu et al 26 did not find any significant difference in the rate of recurrence between patients who underwent a level V ND and those who did not (8% vs 9% of recurrence). Similar findings were noted by McNamara et al 27 (7.4% vs 9%). Interestingly, the rate of recurrence to level V was also relatively low in the study by Xu et al, with only 4.8% (n = 5) of their patients having experienced a level V recurrence.
Our study has several limitations worth mentioning. It is retrospective in design, and it was conducted in a single institution. The limited size of the entire cohort restricted the number of patients who sustained a recurrence. The policy of our institute was to perform a therapeutic level V ND; therefore, we could not determine the value of an elective level V ND in patients who had no clinical evidence of disease. It is also important to take into account that our patients were treated according to the different ATA guidelines that were in place over time. Another limitation is that a minority of the patients (N = 13) had a follow-up period of less than 1 year. Moreover, due to limited amount of recurrences, we did not perform a subgroup analysis according to the initial clinical presentation of the different levels involved in the lateral compartment (levels II-IV separately).
In conclusion, patients with PTC with advanced locoregional disease to the lateral neck who underwent thyroidectomy with or without a therapeutic level V ND did not have significant histopathological characteristics other than microscopic ETE. There were more males and more patients with palpable neck lymphadenopathy at initial physical examination among those who required a therapeutic level V ND. More patients who required a therapeutic level V ND had microscopic ETE and vascular invasion, increased numbers of resected LNs, and a greater ratio of metastatic to resected LNs. The recurrence rate to level V was very low throughout follow-up and did not differ between those who did and did not undergo a therapeutic level V ND. A multivariate analysis with a regression model did not detect therapeutic level V as being a significant risk factor for an increased recurrence rate. Our experience stresses the need for careful preoperative evaluation of patients in order to better assess the potential prophylactic benefit of an elective level V ND. Further larger multicenter studies on the indications and guidelines of an elective level V ND are required to validate our findings in order to refine patient selection according to individual risk of recurrence and disease aggressiveness.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.