
Abstract
A petrous bone cholesteatoma (PBC) is a rare epidermoid cyst of the petrous portion of the temporal bone. The main treatment is subtotal petrosectomy (SP), which generally involves sacrificing the chorda tympani. We report a case of extensive supralabyrinthine PBC in an elderly patient undergoing hemodialysis that was treated by SP with anatomical preservation of the chorda tympani. To the best of our knowledge, preservation of the chorda tympani during SP has not been previously reported. For maintenance of postoperative taste and appetite, preservation of the chorda tympani is a meaningful maneuver whenever possible.
Introduction
Petrous bone cholesteatoma (PBC) is a rare epidermoid cyst affecting the petrous portion of the temporal bone. 1 Several surgical approaches are possible, but selection of the most appropriate technique is made on a case-by-case basis according to the anatomical extension of the PBC and the patient’s residual inner ear function. 1
Subtotal petrosectomy (SP) is a procedure that involves removal of all air cells of the temporal bone, including the middle ear and mastoid, followed by blind sac closure of the external auricular canal and obliteration of the cavity with abdominal fat.2,3 The otic capsule may be removed or spared depending on each case. The incus and malleus are removed, and the chorda tympani is generally sacrificed. Subtotal petrosectomy is routinely used in the management of chronic otitis media (with or without cholesteatoma) and is an effective solution for well-selected cases, such as chronically draining ears that have already undergone multiple operations, with profound hearing loss or low remaining inner ear function.4,5 The procedure may also be indicated for extensive cholesteatomas, including PBCs.
We report a case of extensive supralabyrinthine PBC in an elderly patient undergoing hemodialysis that was successfully treated by SP with preservation of the chorda tympani.
Case Report
An 81-year-old man was referred to our department with a 1-week history of dizziness. He had suffered from right hearing loss for many years but had no history of otorrhea, facial nerve palsy, or surgical interventions such as myringotomy or ventilation tube insertion.
The patient had a significant medical history, including hypertension and diabetes mellitus requiring treatment for over 30 years. He had twice undergone percutaneous coronary intervention (with multiple stent placements) due to stable angina pectoris, and his antiplatelet therapy included clopidogrel (75 mg/d) and aspirin (100 mg/d). The patient had stage 5D chronic kidney disease and had been undergoing conventional hemodialysis 3 times a week for over 7 years. He ambulated with a walking stick following left total hip arthroplasty 2 years previously.
Clinical examination on presentation showed that the right tympanic membrane had no perforation or discharge, but a retraction was noted in the pars flaccida. The left tympanic membrane had no retraction (Figure 1A and B). Pure-tone audiometry revealed right mixed hearing loss with an air-bone gap of more than 30 dB (Figure 1C).
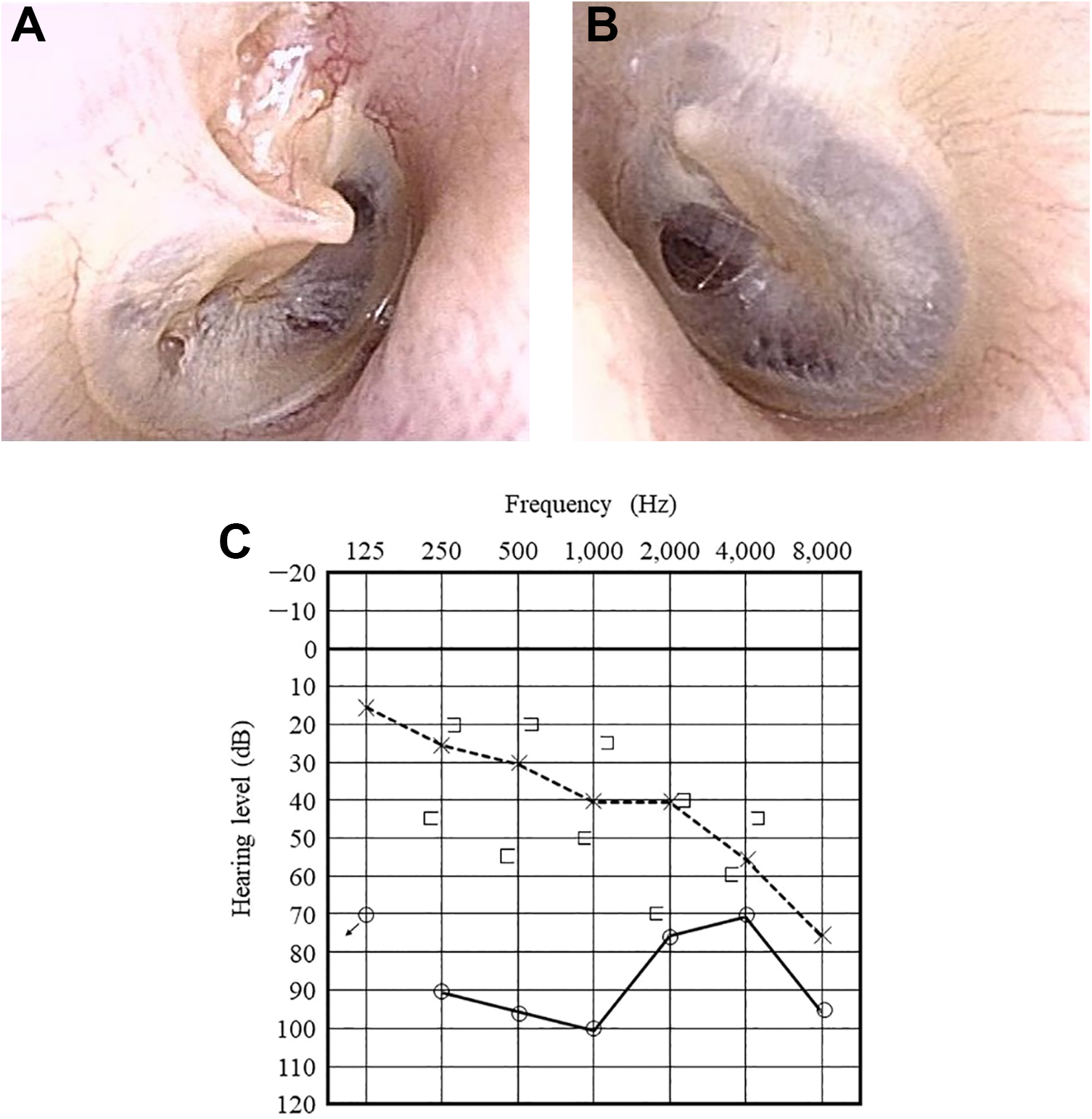
A and B, The tympanic membrane in the right ear is dry without perforation, and middle ear effusion is not observed. There is a retraction in the pars flaccida but no tympanic retraction in the left ear. C, Preoperative pure-tone audiogram shows mixed hearing loss with an air-bone gap of more than 30 dB.
Computed tomography (CT) demonstrated an expansive and destructive lesion mainly located in the mastoid, extended medially to the superior semicircular canal with a possible fistula. The posterior wall of the external auditory canal was unaffected, but there were large bony erosions toward the middle and posterior cranial fossae in the area of the tegmen and sigmoid sinus, laterally toward the mastoid cortex. The malleus and incus were slightly eroded superiorly, but the stapes was not affected by the cholesteatoma (Figure 2A-C).
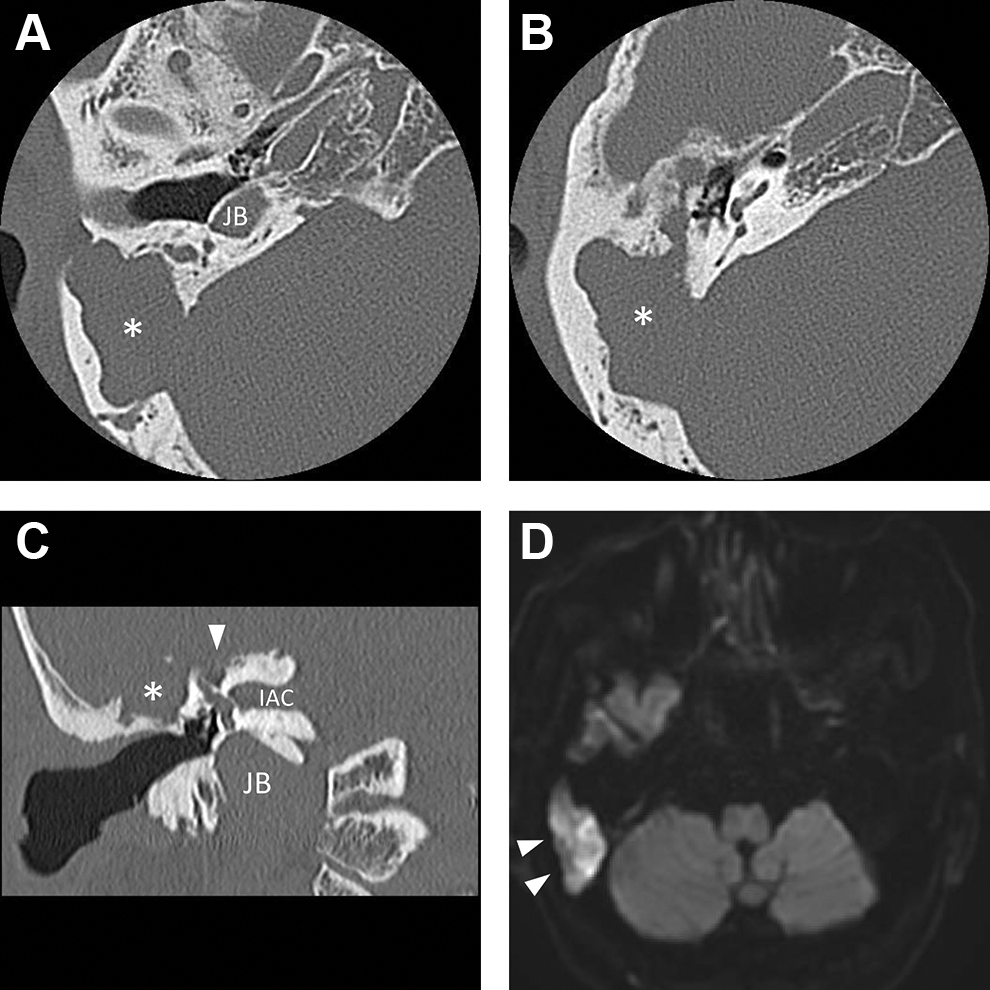
Preoperative CT of the right side shows a destructive lesion (*) in the temporal bone. A, The mastoid cortex and posterior fossa dura are eroded, while the posterior wall of the external auditory canal is intact. B, Although the lesion is extended superolaterally to the incus, the low-density area is not observed in the mesotympanum. C, A possible superior semicircular canal fistula (white arrow) is identified (c). D, DW MRI shows increased signal intensity in the temporal bone. CT indicates computed tomography; DW, diffusion weighted; MRI, magnetic resonance imaging.
On magnetic resonance imaging (MRI), the lesion was hypointense or isointense on T1-weighted images and hyperintense on T2 images. However, diffusion-weighted (DW) MRI showed increased signal intensity in the temporal bone (Figure 2D). A gadolinium contrast MRI was not performed due to the kidney disease and hemodialysis.
We diagnosed the patient with a supralabyrinthine cholesteatoma. After discussing the risks and benefits of the treatment options, surgery was selected in accordance with the patient’s preference. The patient’s clopidogrel was temporarily stopped 1 week before surgery, but the aspirin continued perioperatively.
At surgery, a postauricular skin incision was completed under general anesthesia. The cholesteatoma was identified from the bony erosion of the mastoid cortex. Canal wall down mastoidectomy and blind sac closure of the external auditory canal were performed (Figure 3A). The cholesteatoma in the temporal bone was extended posteriorly to the sigmoid sinus, inferiorly to the mastoid tip, and medially to the labyrinthine segment of the facial nerve; however, it did not extend into the mesotympanum. The malleus and incus were removed, with preservation of the stapes and the chorda tympani (Figure 3B). Extradural removal of the cholesteatoma from the middle and posterior fossae dura was performed. The cochlear aqueduct was not transected and was preserved. To maintain inner ear function, the medial portion of the cholesteatoma was removed endoscopically without labyrinthectomy (Figure 3C-E). The sigmoid sinus was widely exposed, but the sigmoid sinus vessel wall was preserved without laceration.
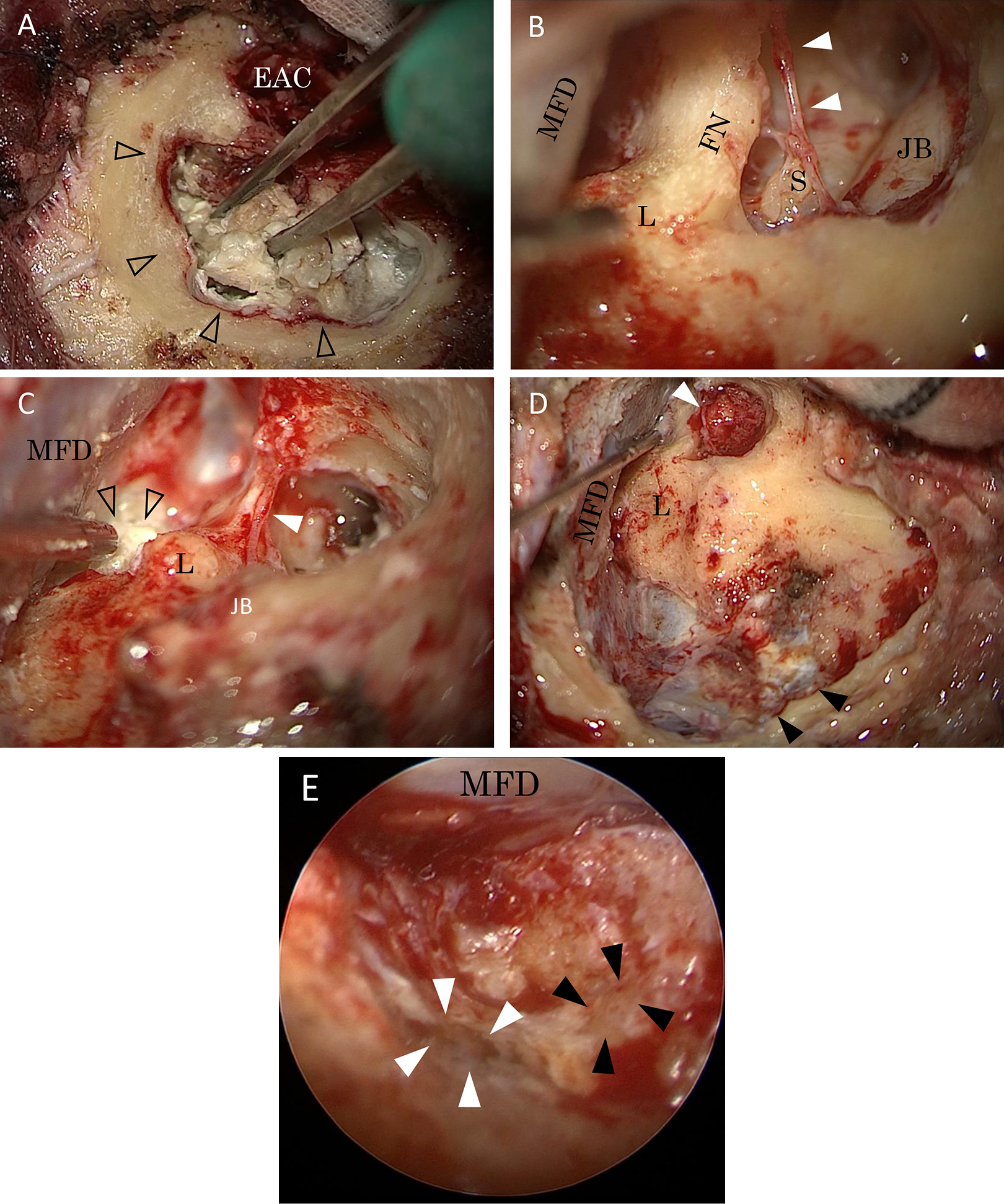
A, A massive cholesteatoma (open arrows) is identified in the temporal bone. Blind sac closure is completed. B, In the middle ear cavity, the stapes and chorda tympani are identified and preserved (white arrows). The malleus, incus, and tympanic membrane are removed. C, After SP without labyrinthectomy, the cholesteatoma (open arrows) medial to the otic capsule is identified. Preserved chorda tympani is identified (white arrow). D, Cholesteatoma is removed with preservation of chorda tympani (white arrow). A piece of muscle is placed in the tympanic cavity to close the Eustachian tube. Sigmoid sinus covered with scar tissue is identified (black arrows). E, Endoscopic view shows the superior semicircular canal fistula (white arrows). The labyrinthine segment of the facial nerve (black arrows) is exposed following cholesteatoma removal. In the upper side, the MFD is widely uncovered following cholesteatoma removal. EAC indicates external auditory canal; FN, facial nerve; JB, jugular bulb; L, labyrinth; MFD, middle fossa dura; S, stapes; SP, subtotal petrosectomy.
The patient’s postoperative clinical course was uneventful, with no dizziness, vertigo, facial nerve palsy, or taste disturbance. Postoperative CT demonstrated removal of the middle fossa tegmen and anatomical preservation of the otic capsule (Figure 4A-C). Diffusion weighted MRI showed no signal intensity at 1 month (Figure 4D) but continued follow-up is necessary. Regardless of the effort to preserve the patient’s inner ear function, postoperative pure-tone audiometry showed deafness of the ipsilateral side as a result of the surgical manipulation of the superior semicircular canal fistula.
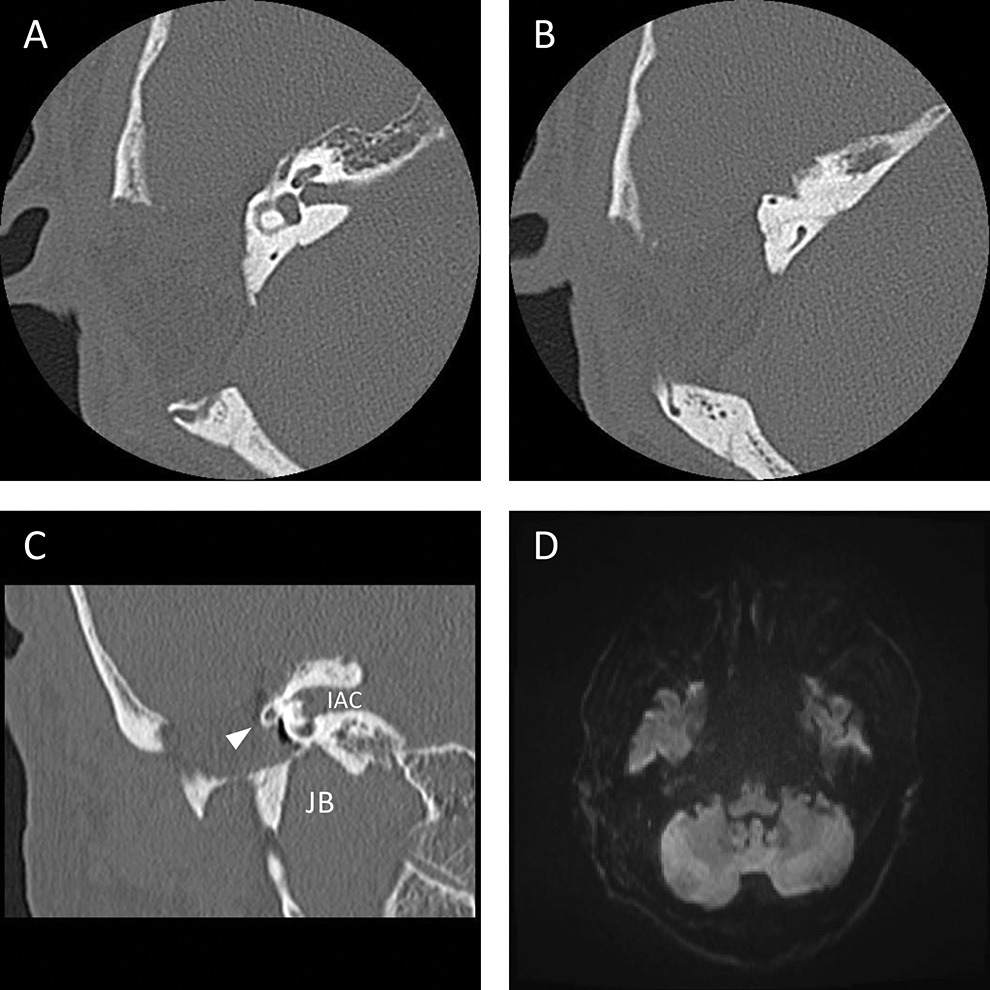
A-C, Postoperative CT shows that the middle fossa tegmen is removed and the otic capsule is anatomically preserved. White arrow indicates the facial nerve. D, Postoperative DW MRI demonstrates no signal intensity in the temporal bone 1 month after SP. CT indicates computed tomography; DW, diffusion weighted; IAC, internal auditory canal, JB, jugular bulb; MRI, magnetic resonance imaging; SP, subtotal petrosectomy.
Discussion
Petrous bone cholesteatomas are mostly slow-growing lesions in the petrous portion of the temporal bone. Because of the insidious course of PBCs, a considerable number of patients are misdiagnosed and present late with complications; therefore, the age at diagnosis covers a wide range, including up to octogenarians. 1
Cholesteatomas are considered congenital when there is no previous history of tympanic disease, such as tympanic membrane retractions or ear discharge, and no previous ear surgery. 6 This case could not be diagnosed as a congenital cholesteatoma because of the tympanic retraction, although it exhibited congenital characteristics, such as the minimal ossicular chain erosion, lack of previous ear surgery and discharge, and intact external auditory canal.
Surgery is the mainstay treatment for PBCs. The surgical choice has evolved from petromastoid exteriorization with drainage of the cavity to complete radical excision following obliterative techniques 7 with efforts to protect the facial nerve and inner ear. 8 Despite great advancements in microscopic skull base surgical techniques, PBC surgery is still a challenge for otologists, and postoperative morbidity remains an issue.
For our patient, SP was selected because of the risk of postoperative cerebrospinal fluid leakage and peri- and postoperative bleeding due to antiplatelet therapy. Although complete excision of the cholesteatoma should be the primary surgical goal, quality of life issues are also important to consider, including preservation of taste,9,10 facial nerve function, and hearing. Management of the chorda tympani is not specifically mentioned in SP surgical techniques,3,11,12 but the nerve is generally sacrificed in the removal of PBCs. However, in the case of middle ear cholesteatomas, the chorda tympani should be preserved whenever possible, especially in elderly patients who have a lower rate of taste recovery after middle ear surgery. 13 We treated our case of supralabyrinthine subtype PBC with SP and anatomical preservation of the chorda tympani. During SP, careful manipulation is necessary in order not to damage the chorda tympani, especially when drilling in the petrous bone with water irrigation, and cottonoids are useful on occasion to protect the nerve.
Involvement of the venous system of the temporal bone requires the utmost care in the treatment in cholesteatomas and other diseases like carcinomas. 14 Although complete resection of the cholesteatoma is theoretically desirable over the sigmoid sinus and/or jugular bulb, preservation of the anatomic integrity of the sinus becomes almost impossible if the dural layer is destroyed or thinned by disease. 15 In this case, preoperative imaging showed that the ipsilateral sigmoid sinus was dominant and not occluded; thus, complete removal of the cholesteatoma with preservation of the sigmoid sinus was performed instead of scarification of the sigmoid sinus.
After SP for an extensive cholesteatoma, long-term MRI follow-up is mandatory 4 because of the large variation in the growth rate of residual cholesteatomas. 5 Although the postoperative DW MRI showed no apparent residual cholesteatoma in our patient, even if residual disease is detected, a wait-and-scan policy can safely be considered after SP, especially in complicated elderly cases.
We report a case of supralabyrinthine subtype PBC treated by SP with anatomical preservation of the chorda tympani. To the best of our knowledge, preservation of the chorda tympani during SP has not been previously reported. In order to maintain postoperative taste and appetite, preservation of the chorda tympani is a meaningful maneuver whenever possible.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.