
Abstract
A congenital mastoid cholesteatoma (CMC) is a keratinizing epithelium originating from embryological epithelial tissue of the mastoid. It is often not diagnosed until it becomes large because of its rarity and indolent nature. Although there are a few reports on giant CMC, its exact extensions have not been well described, and detailed information regarding surgical methods is lacking, especially in giant CMC involving the occipital condyle and the middle and posterior cranial fossae. In this article, we report a case involving a 70-year-old woman with a giant CMC that extended inferiorly to the occipital condyle. The CMC eroded the middle and posterior cranial fossae, sigmoid sinus plate, and fallopian canal of the facial nerve. For complete removal, we used a subtotal petrosectomy in conjunction with an exposure of the cranial cervical junction and a wide decompression of the suboccipit. The boundaries of exposure were similar to those of a petro-occipital transsigmoid approach which is usually used for management of tumor involving the jugular foramen. The wide exposure allowed for complete removal of the lesion without any complications. Thus, we recommend this surgical approach for management of the giant CMC involving the occipital condyle and the middle and posterior cranial fossae.
Keywords
Introduction
A congenital cholesteatoma is an epidermoid cyst originating from residual squamous epithelium in the temporal bone. The middle ear, petrous apex, and external auditory canal (EAC) are common sites of origin. Rarely, it can originate from the mastoid of the temporal bone. 1 The congenital mastoid cholesteatoma (CMC) may not produce symptoms until it becomes very large. Therefore, it is often diagnosed as a giant mass extending beyond the mastoid into adjacent neurovascular structures. Although there are a few reports on giant CMC, its exact extensions have not been well described and detailed information regarding surgical methods is lacking. In addition, to the best of our knowledge, there is no study reporting a giant CMC inferiorly extended to the occipital condyle.
We, herein, present a case of a giant CMC extending inferiorly to the occipital condyle and eroding the middle and posterior cranial fossae. The lesion also caused erosions of the sigmoid sinus plate and fallopian canal of the mastoid segment of the facial nerve. A subtotal petrosectomy in combination with an exposure of the cranial cervical junction and a wide decompression of the suboccipit was performed to remove the giant CMC.
Case Report
A 70-year-old woman presented with otorrhea from her left ear that had started approximately 7 months previously. There was no previous history of otologic trauma or surgery. The patient also complained of ear fullness and hearing impairment in her left ear. On otoscopic examination, the tympanic membrane of her left ear was normal, but destruction of the posterior wall of the EAC was observed. Pure tone audiometry showed a mixed hearing loss with an air-conduction threshold of 36 dBHL and bone-conduction threshold of 74 dBHL in the left ear. The hearing level of her right ear was normal. On computed tomography (CT) of the temporal bone, an expansive soft tissue lesion occupying the mastoid was observed. Erosions of the posterior wall of the EAC, bony plate of the sigmoid sinus, fallopian canal of mastoid segment, and middle and posterior cranial fossae were also noted. The ossicles, except for the malleus, were missing. The cochlea and semicircular canals did not show any involvement. Postcontrast T1-weighted magnetic resonance imaging (MRI) of the lesion revealed a hypointense signal intensity without enhancement (Figure 1A). On T2-weighted MRI, the lesion exhibited a hyperintense signal intensity, which extended inferiorly to the occipital condyle (Figure 1B, C). Diffusion restriction was observed on diffusion-weighted imaging (DWI; Figure 1D). These imaging features were consistent with cholesteatoma.
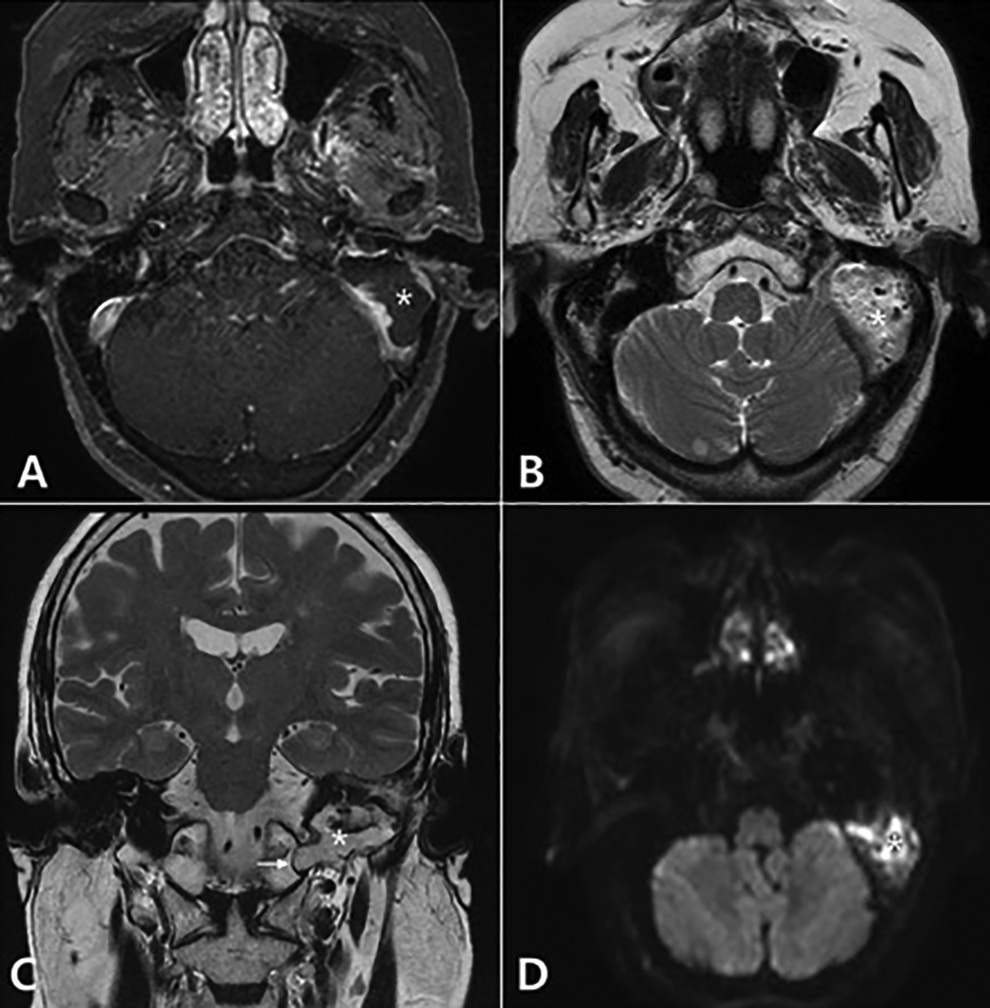
Brain MRI. A, Axial gadolinium enhancement T1-weighted MRI shows a low signal intensity without enhancement on the mastoid of left side (asterisks). B, Axial T2-weighted MRI shows a high signal intensity on the same lesion. C, Coronal T2-weighted imaging shows inferior extension to the occipital condyle (arrow) as well as superior extension to the middle cranial fossa (asterisks). D, Diffusion-weighted imaging shows restriction of diffusion on the same lesion (asterisks). MRI, magnetic resonance imaging.
The lesion could not be reached using only conventional transmastoid approach. For complete removal, we used a subtotal petrosectomy approach in conjunction with exposure of the cranial cervical junction. The middle and posterior cranial fossae as well as the suboccipit were decompressed. The cholesteatoma filled the mastoid (Figure 2A and B) and eroded the middle and posterior cranial fossae. The cholesteatoma also involved the middle ear cavity anteriorly (Figure 2C), and erosion of the mastoid segment of the facial nerve was observed. The cholesteatoma was completely removed after exposure of the posterior condylar emissary vein and the third part of the vertebral artery inferiorly and the suboccipit posteriorly (Figure 2D). Then, the wide surgical cavity was obliterated using inferior rotation of the temporalis muscle. The patient was discharged on postoperative day 9 without any complications, such as facial paralysis. The patient was followed up with clinical evaluations every 6 months. Postoperative MRI showed no evidence of recurrence.
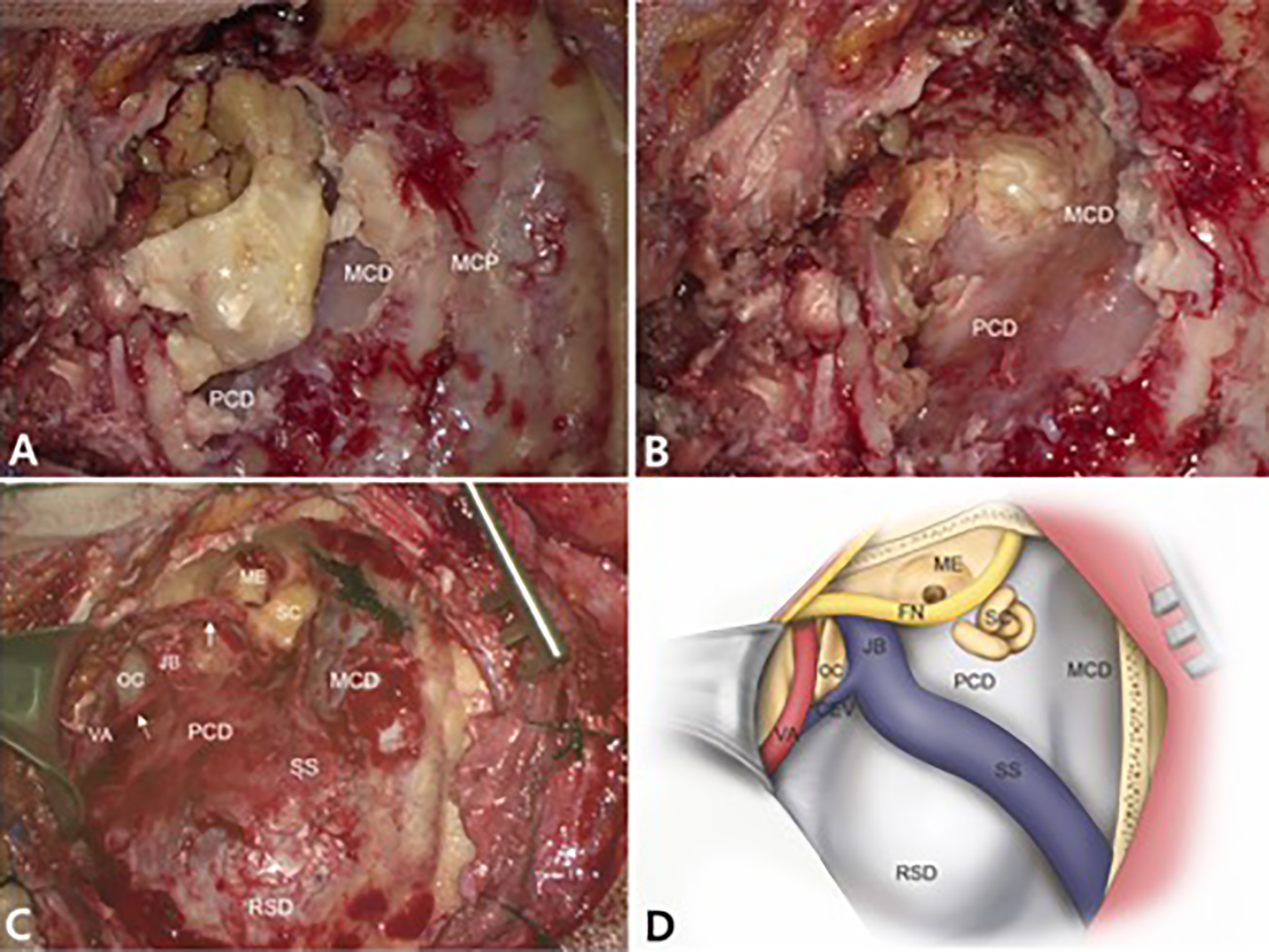
Intraoperative photographs and a schematic drawing of a petro-occipital condylar approach. A, Cholesteatoma (asterisks) erodes the MCP and posterior cranial fossa plates. B, Cholesteatoma (asterisks) extends to the ME as well. The MCD and PCD are exposed widely. C, Cholesteatoma is completely removed after exposing the OC, CEV (broken arrow), the first cervical vertebra, and the third part of the VA. Dehiscence of the facial nerve is also observed (arrow). D, A schematic illustration of the approach used for the present case. It not only decompresses the MCD, PCD, and suboccipit widely but also fully exposes the OC and the VA by extension of a subtotal petrosectomy into the cranial cervical junction region. CEV indicates condylar emissary vein; JB, jugular bulb; MCD, middle fossa dura; MCP, middle cranial fossa plates; ME, middle ear; OC, occipital condyle; PCD, posterior fossa dura; RSD, retrosigmoid dura; SC, semicircular canals; SS, sigmoid sinus; VA, vertebral artery.
Discussion
The mastoid bone is a rare site of congenital cholesteatoma formation. Early diagnosis of CMC can be difficult because of its indolent nature. Symptoms of CMC vary from none to obstructive hydrocephalus, depending on the extent of the lesion. In children, it is often found incidentally on imaging studies, without any specific symptoms. On the other hand, adult patients with CMC present with otologic symptoms, such as otorrhea, ear pain, hearing loss, and retroauricular swelling. 2 In the present case, otorrhea resulted from a destruction of the posterior wall of the EAC by expansion of the CMC. The hearing loss noted was due to ossicular erosion. Interestingly, headache and neck pain were not observed, despite erosion of the cranial fossae and inferior extension of the CMC to the occipital condyle.
Thorough examination, including the patient’s history, otoscopy, and imaging studies, is important for the diagnosis of CMC. 3 When a normal tympanic membrane is visualized on otoscopy, without a history of otologic disease, the cholesteatoma is considered to have a congenital origin. A cholesteatoma can be distinguished from other diseases, such as cholesterol granuloma, mucocele, and endolymphatic sac tumor, using imaging studies. A cholesteatoma demonstrates a hypodense and well-marginated expansive lesion on CT scan. On MRI, a cholesteatoma shows a low signal intensity on TI-weighted images and a high signal intensity on T2-weighted images. On T1-gadolinium enhancement MRI, it does not show an enhancement. Diffusion restriction is observed on DWI.1,3 In the present case, results of the otoscopic examination and imaging were consistent with the diagnostic criteria for a congenital cholesteatoma.
The treatment goal is to completely eliminate the lesion with minimal morbidity. If the CMC is limited to the mastoid, conventional tympanomastoidectomy can be sufficient for removal. When it progresses and spreads beyond the mastoid, the tympanomastoidectomy needs to be extended. In addition, appropriate obliteration is required, since the surgical defect is large after removal of the lesion. Cvorovic et al reported that a CMC with erosion of the bony plate of the posterior cranial fossa was removed through a transmastoid-perilabyrinthine approach, and the surgical cavity was obliterated using the temporalis fascia and muscle. 1 Cazzador et al removed a huge CMC using a combined microscopic and endoscopic approach. They were able to achieve minimal morbidity and avoid radical surgical using the endoscope. 4 In the present study, we performed a subtotal petrosectomy in conjunction with an exposure of the cranial cervical junction and a wide decompression of the suboccipit for removal of a giant CMC extending to the occipital condyle. This surgical procedure extended a radical mastoidectomy into the cranial cervical junction region to expose the occipital condyle inferiorly. The boundaries of exposure are similar to those of a petro-occipital transsigmoid approach which is usually used for management of tumor involving the jugular foramen. 5 Accordingly, it not only decompresses the middle and posterior cranial fossae widely but also fully exposes the occipital condyle and the third part of the vertebral artery (Figure 2C, D). This wide exposure allowed a giant CMC to be removed completely. Hearing rehabilitation, such as a bone anchored hearing aid, was not considered because hearing in the opposite ear was normal, and the patient declined it.
In conclusion, CMC can be diagnosed at various sizes because of their indolent nature. Congenital mastoid cholesteatoma in children is often diagnosed incidentally at an early stage, with a small size that can be removed with a conventional tympanomastoidectomy. On the contrary, in adult patients with CMC, the conventional approach may be insufficient, as they are often not diagnosed until the CMC progresses to a giant size, like that of the present case. Therefore, it is important to understand the progression of CMC for appropriate management. In particular, CMC with inferior extension to the occipital condyle and erosions of the middle and posterior cranial fossae can be successfully treated using a subtotal petrosectomy in conjunction with an exposure of the cranial cervical junction and a wide decompression of the suboccipit, which allows the occipital condyle, suboccipit, first cervical vertebra, and vertebral artery to be exposed widely.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.