
Abstract
Introduction:
Incidental papillomas of the pharynx can be found while examining the nasopharynx, oropharynx, and hypopharynx for other disorders of the head and neck. Purpose of the study is to explore the location, biopsy protocol, and decision to perform office-based versus operative management via potassium titanyl phosphate (KTP) laser when an oropharyngeal papilloma is discovered incidentally.
Methods:
A retrospective review of the senior author’s patient population was performed using Current Procedural Terminology and/or International Classification of Diseases codes to identify patients who had KTP laser removal of incidental oropharyngeal papillomas. Patients were included based on the incidental nature of the papilloma and confirmed pathology report of squamous papilloma. Demographics, presenting complaint, lesion location, pathological analysis, type of intervention, and outcomes were recorded. When available, human papillomavirus (HPV) subtype was noted.
Results:
A total of 26 cases were identified, 13 females and 13 males. The median age at time of surgery was 58 years (range: 21-77). The most common presenting symptoms were difficulty swallowing and throat pain. The most common locations were the base of tongue, uvula, tonsils, and the soft palate. Of the 26 patients, 23 patients received KTP laser ablation therapy as an office-based procedure, while the remaining 3 were performed under general anesthesia in the operating room. Only 5 patients had a recorded recurrence that required reoperation. There were no operative or postoperative complications. There were 16 biopsy samples tested for HPV, where 12 were negative for HPV and 4 were positive for HPV.
Conclusion:
Oropharyngeal papillomas, when present, can be found incidentally during examination of the oropharynx for other symptoms. Office-based biopsy and KTP laser is a safe and efficient means of identifying and removing most oropharyngeal papillomas.
Introduction
Over the past decade, office-based procedures have grown in popularity in the laryngology community. 1 Specifically, potassium titanyl phosphate (KTP) laser therapy provides a safe, cost-effective means for in-office management of laryngopharyngeal and intraoral lesions. 2 -4 Although the exact mechanism of KTP laser ablation is unclear, current theory points to targeting microcirculation, as the laser’s frequency is selectively absorbed by hemoglobin and not by water, making it an ideal tool for removing highly vascular lesions such as papillomas. 5 This fundamental principle of selective radiation of hemoglobin by the KTP laser provides effective hemostasis, allowing a relatively low-risk office-based procedure performed under local anesthesia. The KTP laser has multiple clinical uses including the treatment of vascular malformations, cholesteatomas, acne, and benign prostatic hyperplasia. 6 -12 Specifically, in the laryngology community, the KTP laser has been used for recurrent respiratory papillomatosis (RRP), vocal cord ectasia/varices, microvascular lesions, glottic carcinoma, and other benign pathologies and mixed lesions. 13 -21
Although the efficacy of the KTP laser in treating head and neck lesions is well established, current literature describing its use in the oropharynx to treat papillomas upon incidental discovery is limited. Many studies have focused on its use in tonsillectomies and uvulopalatopharyngoplasty. 22 -25 Similarly, the use of KTP and other technologies such as the CO2 laser or pulsed dye laser (PDL) therapies in the management of laryngeal lesions is well-documented. In particular, multiple studies by Zeitels et al demonstrated the value of office-based KTP laser ablation for the treatment of RRP. 4,5,15,26 -28 In another study, office-based KTP laser ablation for the treatment of benign laryngeal conditions such as hemorrhagic polyps showed statistically significant reduction in the size of these lesions. 21 In a multi-institutional retrospective study, office-based KTP laser ablation induced a significant reduction in the size of various laryngeal lesions. 29 Thus, the KTP laser in the office setting has been shown to be efficacious in a variety of head and neck lesions. To our knowledge, this is the first study describing the implications and management of oropharyngeal papillomas using the KTP laser.
Standard procedure for the management of benign oropharyngeal lesions such as papillomas is typically surgical excision or laser ablation using CO2, PDL, or more recently, KTP—although the natural history of these lesions is unknown. The risk of progression to malignancy is unknown until after the lesion is removed, and serotyping has been performed with a potentially increased risk of developing malignancy in the setting of high-risk human papillomavirus (HPV) phenotype. 30 This retrospective review aims to document the safety and efficacy of the use of KTP laser to manage these types of lesions, specifically incidental papillomas of the oropharynx. It also includes data on HPV strains associated with these lesions when available.
Methods
A broad search using Current Procedural Terminology (CPT) and International Classification of Diseases (ICD) codes (ICD9/10: C06.9, D10.3, D10.5, D10.6, D10.9, D38.0, D37.05, D10.9, D14.1, R22.1, J38.7, J38.02; CPT: 31576, 42100, 42160, 42800, 42808, 42870) for patients diagnosed with oropharyngeal papillomatosis was performed between the years 2013 and 2015. Chart review of patients found to have incidental papillomas of the pharynx was evaluated for demographic data including age and sex. Patients were included for oropharyngeal papillomas found on oral/oropharyngeal examination or flexible laryngoscopy while evaluating patient for complaint not caused by the lesion itself. Patients with nonincidental papilloma referred for removal or papillomas of the larynx were excluded.
Patients were stratified based on method of excision used to remove the lesion(s). The incidence of recurrence and procedural complications was evaluated for each treatment modality. All lesions were excised and biopsied transorally or transnasally with a flexible laryngoscope following previously published biopsy protocols and were identified as squamous papilloma. 31 For transnasal biopsies, 2 sprays of 50:50 mixture of 1% phenylephrine and 1% pontocaine were sprayed into each nasal cavity. Once the scope was passed, 3 mL of 1% pontocaine was dripped into the lesion while the patient was phonating. Human papillomavirus subtype, recurrence rate, complications, and symptoms were evaluated. Human papillomavirus status was determined using p16 immunohistochemistry and HPV polymerase chain reaction. Human papillomavirus types were stratified as the following: HPV-6 and -11 as low-risk types, and HPV-16, -18, -31, -33, -35, -39, -45, -51, -52, -56, -58, -59, -66, and -68 as high-risk types. 32
Results
Search criteria yielded 26 patients who were found to have incidental oropharyngeal papillomas treated with KTP laser. Of these patients, 23 were treated in the office and the remaining 3 in the operating room (OR). Of the 23 in-office patients, there were 12 males and 11 females with median age of 58 years (range: 21-77). Of the 3 patients treated in the OR, there were 1 male and 2 females, with median age of 48 years (range: 35-61; Table 1).
Clinical Features of Incidental Oropharyngeal Papillomas.
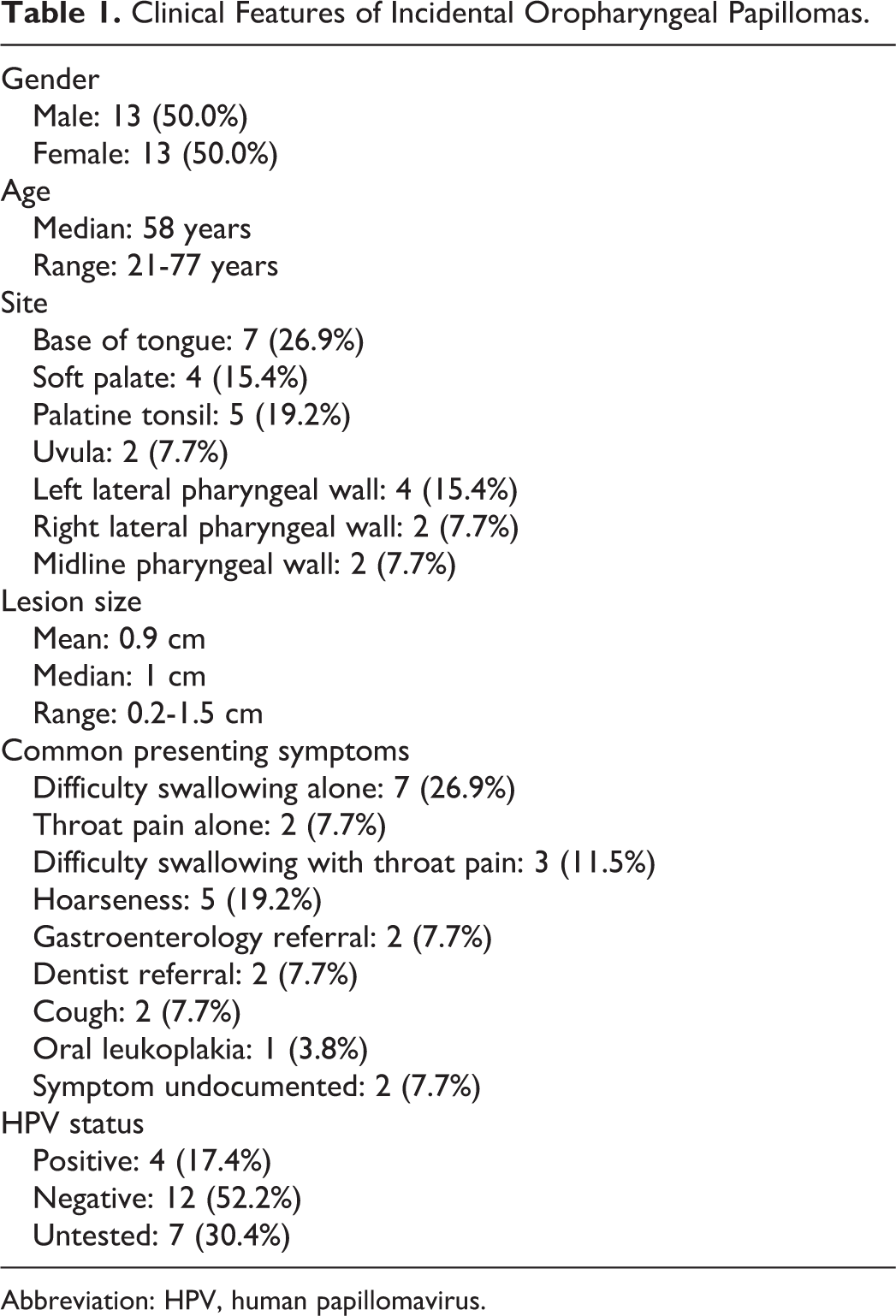
Abbreviation: HPV, human papillomavirus.
All of the patients in our study had lesions found incidentally during workup for another symptom. Difficulty swallowing and throat pain were the most common presenting symptoms, as 7 patients presented with difficulty swallowing alone, 2 patients with throat pain alone, and 3 patients with both. Following that 5 patients presented with hoarseness, 2 presented with cough, 2 lesions were found and referred by dentists, 2 lesions were found and referred by a gastroenterologist after esophagogastroduodenoscopy, 1 presented with oral leukoplakia, and 2 patients did not have a presenting symptom listed in the chart.
The lesions removed in the office ranged in size from 0.2 to 1.5 cm (mean 0.9 cm) and were located in the oropharynx. Specific location of the lesions included 7 on the base of tongue, 5 on the palatine tonsil, 4 on the soft palate, 4 on the left lateral pharyngeal wall, 2 on the right lateral pharyngeal wall, 2 in the midline pharyngeal wall, and 2 on the uvula (Figure 1). There were no complications.

Incidental left-sided pharyngeal papilloma of low-risk subtype biopsied in the office setting. Patient was being evaluated for chronic dysphonia (left); incidental base of tongue papilloma of high-risk subtype (HPV 16) in a woman being evaluated for chronic cough (right). HPV indicates human papillomavirus.
All patients were diagnosed with squamous papilloma on histopathology. Among all patients, 16 had their lesions sent for HPV testing in addition to histopathology. Of the 16, 12 were negative for both high- and low-risk HPV strains, 2 were positive for high-risk strains, 1 was positive for both high- and low-risk strains, and 1 was HPV positive without specific strain data found in the chart.
There were a total of 5 recurrences, consisting of 3 in-office patients and 2 patients treated in the OR. Of the 3 in-office patients who had recurrent lesions, 2 patients had recurrence on the soft palate, and the remaining patient on the right lateral pharyngeal wall. Average time from the first operation to initial recurrence ranged from 35 to 505 days. Of the patients who have documented return visits without noted recurrence of disease, the average time from surgery to their most recent appointment was 300.5 days (range: 14-1313).
Among the 3 patients treated under general anesthesia, one was taken to the OR for recurrent diffuse nasopharyngeal papillomatosis and one was taken directly to the OR for diffuse disease but tolerated a subsequent reoperation in the office. Only 1 patient was unable to tolerate the initial procedure in the office and had to be subsequently taken to the OR for surgery under general anesthesia; however that patient had recurrent disease and was able to tolerate a later operation in the office. There were no postoperative complications.
Discussion
Given the location and size of oropharyngeal papillomas, most are asymptomatic, especially when small and slow growing. The discovery of oropharyngeal papillomas in our cohort was incidental, with the majority being found on workup for other unrelated symptoms of difficulty swallowing, throat pain, or hoarseness. During the biopsy, patients are awake in the sitting position, and local anesthesia is administered to retrieve the tissue sample transorally or transnasally using a flexible laryngoscope and forceps through the channeled scope. The remainder of the lesion can then be ablated using the KTP laser. Thus, such lesions can be easily biopsied and excised in 1 setting in the otolaryngologist’s office. Of the 3 patients who were taken to the OR for surgery under general anesthesia, only 1 patient was taken to the OR because of inability to tolerate in-office KTP laser excision due to discomfort. That patient had recurrent disease after the first procedure and was able to tolerate a subsequent procedure attempted in the office under local anesthesia. Overall, all patients were able to tolerate the procedure at some point. With zero reported complications among the patients in our study, KTP offers a low-risk, efficient in-office treatment modality for these lesions.
In regard to recurrence in our patient cohort, it must be noted that recurrence of oropharyngeal papillomas after resection is uncommon. Reasons for recurrence in our patients may due to original lesions being diffuse, multicentric, and scattered throughout the pharyngeal wall. During removal of these lesions, some of the numerous lesions may be missed or the patient may be in an active phase of disease and have regrowth after complete removal. Lastly, presenting symptoms such as sore throat is not a common presentation in patients with oropharyngeal papillomas. In these patients, they may have other underlying causes of sore throat such as laryngopharyngeal reflux, tonsil stones, or esophageal hypersensitivity.
Although there is limited information published on the costs and benefits of office-based management of oropharyngeal squamous papillomas, we extrapolate based on the management of RRP with KTP laser to predict outcomes for oropharyngeal papillomas. Office-based management of RRP is preferred by patients because it saves time, avoids the risks of general anesthesia, and is cost-effective in comparison to the OR. 33 A study by Rees et al also found that patients who had undergone procedures both in the office and in the OR under general anesthesia prefer the in-office management due to increased comfort, decreased recovery time, decreased operative time, avoiding risk of general anesthesia, and cost. 34 The ability to perform in-office procedures also decreases the time from diagnosis to treatment, an important factor when dealing with lesions that have possible but unknown malignant potential. 33 In terms of safety of the KTP laser, only a few studies report on complication rates, and some authors suggest that the KTP laser may be safer than other commonly used lasers such as the PDL. 4,13,14,17 However, no studies have been done comparing the differences in complication rates after treatment using KTP to other lasers. Therefore, more studies, such as a randomized controlled trial, would be ideal in firmly answering the question of efficacy and safety of the KTP laser compared to others.
Currently, while considerable data exist describing HPV oncogenesis in the uterine cervix, the literature detailing the mechanism by which HPV causes tumorigenesis of the head and neck is still underway. 35 -38 It is theorized that infections, particularly those with high-risk HPV type 16, persist in the oropharynx, incorporate into host DNA, and produce oncogenic proteins E6 and E7 that allow them to progress to oropharyngeal squamous cell carcinoma (OPSCC) in a similar fashion to the progression of cervical cancer. 38 More recent research has implicated the HPV E6 protein in the deregulation of the Hippo pathway, causing epithelial to mesenchymal transition in infected cells and promoting oncogenic progression. 39 This progression from initial infection to malignancy takes decades, and our understanding as to why some infections progress while others are cleared is limited. Certain factors, such as smoking and HIV infection, diminish an individual’s ability to clear the initial infection and therefore naturally increase the oncogenic risk. Moreover, it is well established that HPV can be sexually transmitted to the oropharynx via oral–genital contact, but not through nonsexual modes of contact. 40 Given this nature of sexual transmission, HPV may affect both young and older patients.
In our cohort of patients, these lesions were identified and removed as the natural history of identified papillomas has not been determined. Similar to how HPV-related OPSCC tends to favor specific areas of the oropharynx such as the base of tongue and tonsils, our patient cohort had squamous papillomas in these locations. 41 However, it must be noted that most patients in our cohort were HPV negative. Just as many HPV infections are cleared, papillomatous lesions might also resolve spontaneously. However, at this time, there is no means to determine which will regress, which will progress to carcinoma, or which will remain unchanged. Additionally, the HPV status and type are unknown upon finding these lesions. The presence of these lesions could signify a more active state of HPV infection increasing the risk of oropharyngeal transmission, although this too is currently unknown. Although there were no complications in our cohort of patients with high-risk HPV types detected from biopsy, we suggest these patients to follow-up annually to ensure regrowth has not occurred. Given the ease of biopsy and removal in the office setting, we advocate removal when found incidentally.
Lastly, screening for detection of malignant lesions in the oral cavity or oropharynx deserves attention. It has been shown that routine visual screenings reduce oral cancer mortality in populations at high risk for non-HPV OPSCC. 42 However, unlike the cervical Pap test, which is used to detect cervical epithelial dysplasia in order to prevent progression to cervical cancer, there is no universal screening test to detect early HPV-related changes in the oral or oropharyngeal mucosa. One study attempted a “Pap-test equivalent” using brush cytology samples from tonsillar tissue but was unable to find correlation between HPV status and cytologic abnormalities in healthy individuals. 43 This is due to the fact that HPV only rarely causes cellular changes, and when it does, it only occurs in a finite location that is not always easily accessible to brush biopsy, making this method of screening ineffective. For now, routine visual inspection, usually performed by a dentist, is the best method to decrease oral cancer mortality. More research is needed to develop a method of identifying premalignant changes in the oral epithelium. Also, patients may be advised on the benefit of receiving HPV vaccinations, as research has shown a significant decrease in prevalence of oral HPV types 16 and 18, 4 years after vaccination with the bivalent vaccine. 44
The current study is not without limitations. It was retrospective and limited in sample size. Because of the retrospective nature of the study, not all biopsies obtained were evaluated for HPV status. Thus, external validity of the study is limited. However, our study provided broad sampling given the rare nature of these incidental lesions, which were evaluated in a tertiary laryngology center.
Conclusion
Potassium titanyl phosphate laser surgery is widely recognized as an appropriate method for treatment of RRP and other vascular lesions. Our case series confirms that KTP laser surgery is a safe and effective method for removal of oropharyngeal papillomas that is well tolerated in the office under topical anesthesia.
Footnotes
Authors’ Note
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee (Institutional Review Board 11279-101) and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. This study was approved by the college’s institutional review board.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.