
Abstract
Objectives:
To present the value of office-based laryngological procedures as an effective alternative method to the treatment of benign and malignant laryngeal pathologies.
Methods:
We have reviewed the technological advancements of fiber-guided laser systems, fiberoptic endoscopes, and high-definition imaging systems that have enabled office-based laryngological procedures. We describe the importance of case and patient selection, the available laser systems, and the technique applied.
Results:
Several benign and malignant pathologies can be now treated in the office under local anesthesia with angiolytic or thermocoagulative lasers and with success rate comparable to that of general anesthesia. Safety guidelines and laser precautions must be implemented invariably to protect the patient and caregivers from the untoward effects of laser. Although there is considerable reduction of cost with office procedures, there are risks of undertreatment, increased repeatability, as well as tissue edema from the burning effect.
Conclusions:
The low learning curve, high patient satisfaction rate, and excellent results indicate that in-office laser procedures have become an effective weapon in our armamentarium.
Introduction
Office-based laryngeal procedures are not a novelty. Even in the 19th century, such procedures were performed in the office or outpatient area under local anesthesia. However, improvement in the safety of general anesthesia, the introduction of modern anesthetic equipment and ventilation systems, the use of the microscope, and the development of phonomicrosurgical techniques had shifted the preference of doing these procedures under general anesthesia.
The recent advances in laser fiber systems and fiberoptic endoscopy with high definition chip tip flexible fiberoptic endoscopes with working channel have enabled laryngologists to perform procedures in the office setting with accuracy comparable to the ones in the operating room. The benefits are numerous; fewer anesthesia-related complications, shorter recovery times, ability to return to work almost immediately, 1 as well as easier planning, reduction in operating time, ability to assess patients phonatory outcome in real time, inclusion of patients not suitable for general anesthesia, reduction of operational cost. A cost analysis on office-based laser procedures for recurrent respiratory papillomatosis demonstrated a significant cost-effectiveness of office than operating room procedures. 2 Although this may be true in the hospital setting, it may not be so in the private office. In another review, 3 procedures in the office under topical anesthesia showed a hospital cost reduction of up to 95% per procedure compared to similar done under general; however, there is still large variability due to different coding systems, equipment and consumables availability, reimbursement levels, safety issues, and physician training level. Nevertheless, 93% of patients would be willing to undergo a second awake procedure, thus indicating high patient satisfaction. 4
Case selection
Currently, most of benign vocal fold and laryngeal pathologies can be treated in the office setting. These include most lesions with high vascularity, due to the photoangiolytic properties of the laser being used, such as vocal fold telangiectasia, laryngeal papilloma, Reinke’s edema, hemorrhagic polyp, contact granuloma. Additional pathologies that have been attempted with variable success include anterior glottic web, sulcus vocalis, chronic laryngitis, laryngeal cyst, and dysplastic lesions including early glottic cancer. 2, 5 -8
Anesthesia and Patient Selection
In order to achieve a successful result, patient selection plays a very important role. Personality traits, lack of familiarization or bad experience with local anesthesia procedures, different tolerance to the local anesthetic are some of the factors that discourage patients to agree to it. Moreover, the physician should be able to identify these patients who are suitable for an office procedure. Given the fact that a laser procedure will result in destruction of the lesion, the need of pathologic specimen may preclude the use of this technique for exclusive treatment of dysplastic, papillomatous, or other distinctive lesions where histopathology is necessary. 5 Moreover, hemodynamic status is infrequently monitored in the office, unlike in the operating theater. Morisson et al 9 have found severe hypertension in 21% of patients undergoing in-office procedures and tachycardia in 40% of patients. This risk appears to increase with advancing age. 9 It is, therefore, imperative to consider these physiologic effects as risks for potential complications in the office setting. Furthermore, there is emerging data that patients who remain on anticoagulation or antiplatelet therapy appear to be at no increased risk for complications and have comparable voice outcomes compared with patients not on therapy during and after awake in-office laryngeal procedures. 10
Suitable Laser Systems
Technologies compatible with in-office procedures include flexible fiberoptic high-definition chip tip endoscopes and fiber-based laser systems, such as pulsed-dye laser (PDL), pulsed potassium titanyl phosphate (KTP) laser, CO2 laser, thulium: yttrium aluminum-garnet, and TruBlue laser. Each laser has a unique wavelength. For example, KTP’s wavelength is 532 nm, PDL’s 585 nm, and TruBlue’s at 445 nm. The energy from these wavelengths is absorbed selectively by oxyhemoglobin, allowing the laser to preferentially cause photoangiolysis of blood vessels. When the exposure time of the tissue to the PDL, TruBlue, and/or KTP are pulsed, the usual zone effect of destruction is minimized, thus protecting the surrounding tissues. On the other hand, CO2 laser has a wavelength of 10.6 µm and is absorbed in water, making it more of a cutting and coagulative rather than an ablative instrument. With currently several types of flexible CO2 laser fibers commercially available, its indications surpass previous restrictions and extend to supraglottic malignant tumors or those glottic where the superficial lamina propria has already been damaged by prior surgery or local invasion. 11 Regarding tolerance, a comparison between a more traditional ablative laser, that is, PDL, and the flexible CO2 was very similar in the office setting 12 and suggested that it may also be applied in the office setting in selected cases where healing from thermal injury is not of paramount importance for optimal phonatory outcome. The decision to use one laser versus another varies based on the characteristics of the lesion and optimal wavelength, as well as availability; however, for most practices, it is impractical to purchase and maintain several lasers for a relatively small volume of in-office therapies.
Application of Laser Precautions
Whether in the operating room or the office setting, laser precautions must be applied invariably. The current guidelines from the US Center for Disease Control for surgical smoke and respiratory protection in health care facilities 13 advise health care personnel to wear appropriate personnel protective equipment, including N95 or N100 respirators, to minimize exposure to laser plumes in settings where surgical lasers are used. They also recommend to use central wall suction units with in-line filters to evacuate minimal laser plumes and to use a mechanical smoke evacuation system with a high efficiency filter to manage the generation of large amounts of laser plume, when ablating tissue infected with human papilloma virus. These recommendations are in line with the US National Institute for Occupational Safety and Health 14 and the Association of Perioperative Registered Nurses. 15 The patient and all present personnel must wear the appropriate protective eye goggles. Laser signage must be present at the door to prevent unwanted entry into the room. Proper ventilation and normal room air O2 of the office or clinic room must be ensured.
Although there are no published guidelines in laryngology, several authors have recommended some measures to promote patient safety. A cardiovascular pre-screening tool for high risk patients to prevent avoidable complications was proposed by Madden et al, 16 consisting of measuring vital signs at the preoperative appointment to screen patients and refer to the appropriate physician before exposing patients to avoidable risks. Yung and Courey also suggested the monitoring of vitals during these procedures after reporting significant changes in blood pressure and heart rate. 1
Technique
The success of the procedure relies significantly on careful patient selection and appropriate laser settings. The patient is brought in the office or procedure room and is sat in the procedure chair. The patient’s most patent nasal cavity is properly decongested and anesthetized with a phenylephrine/lidocaine spray or cotton pledgets that are well impregnated with the decongestant/anesthetic solution. After allowing enough time for maximum action, a flexible endoscope with working channel is gently introduced to the well prepared nasal cavity and up to 5 mL of 4% lidocaine mucosal solution are instilled onto the glottis, while the patient is called to phonate or gargle simultaneously to allow for spillage of the topical anesthetic on the entire glottic and supraglottic surfaces. Alternatively, and mostly for subglottic lesions. The anesthetic can be injected into the trachea through the cricothyroid membrane, which will make the patient to cough and spill the material over the subglottic and glottic area. The laser cable is then introduced through the endoscope’s working channel and is visualized at the distal end of the endoscope at a secure distance of more than 1 cm, in order to prevent thermal damage of the distal tip. The preferred laser system is set on the selected settings and the laser is fired either in contact or distant mode until the desirable outcome is achieved (Figures 1, 2, and 3). The settings and delivered energy are recorded at the end of the procedure.
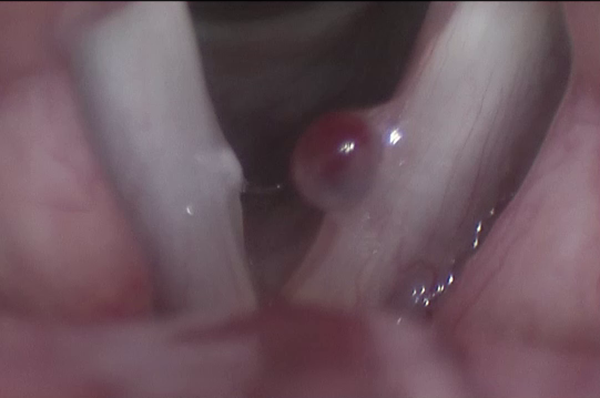
Preoperative image of a hemorrhagic polyp of the left vocal fold.

Potassium titanyl phosphate laser is used both in contact and distant mode; after adequate ablation, the laser fiber is placed on the lesion and is used to detach it from the vocal fold surface.
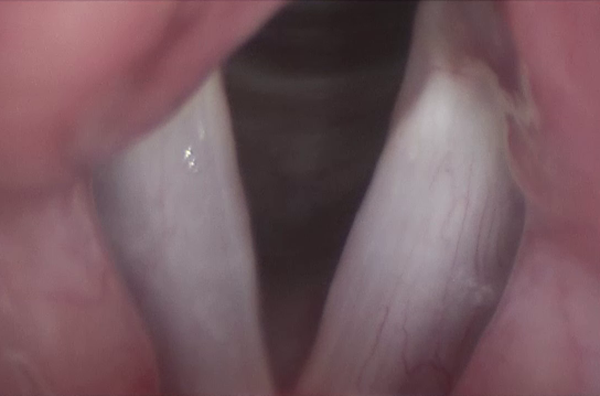
One-month postoperative image with excellent epithelialization of the vocal fold free edge.
Challenges and Complications
Despite the undisputable benefits, office-base procedures have significant disadvantages that have to be considered during the decision-making process. The potential reduction in surgical precision due to patient or operator movement and the subsequent inability to manage intraoperative complications adequately 10,17,18 are limiting factors that depend on the physician’s expertise and patient’s tolerance. This may additionally lead to increased repeatability of the same procedure, resulting in increased estimated cost; nevertheless, this remains substantially lower than that of the same procedure under general anesthesia in the operating room. Moreover, the lack of clear end points in the use of office-based laser surgery for treatment is one of the challenges of office-based treatment of benign mucosal lesions where preservation of function is critical. Given the fact that the laser fiber distance and angle from the lesion cannot be objectively measured, laser fluence and delivered laser energy cannot be standardized for the various laryngeal pathologies, thus leading to vast interrater variability. Moreover, the surgeon prefers to be more conservative in the first session, choosing to minimize scarring from excessive burning and risking treatment inadequacy. 19 In a retrospective study of 255 in-office angiolytic laser procedures, the authors conclude that 20% of these may require additional treatment within 12 months. 19 Unfavorable lesions are those below the free margin of the vocal fold, diffuse lesions, and bulky lesions. With some of the complications encountered with office angiolytic laser treatments being submucosal hemorrhage, vocal fold atrophy, scar and hyperemia with edema, we can better counsel patients on the selection of treatment modality between office and operating room interventions by differentiating them based on lesion size, type, and anatomic position.
Conclusion
Office laser procedures are gaining popularity due to the technological advances in laser systems, optics, and high-definition cameras. A significant number of laryngeal pathologies can be successfully treated in the office setting, with minimal requirements on support from ancillary personnel and hospital resources. The significant reduction in cost and increased patient satisfaction make them more attractive. However, laser safety precautions must be applied invariably to minimize risk exposure of the patient and caregivers. Proper patient and laryngeal pathology selection are very important to minimize unfavorable outcomes and repeatability of the procedure.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.