
Abstract
We propose middle ear implants (MEI) as alternative hearing restoration option for patients with fibrous dysplasia of the temporal bone (FDTB). A 60-year-old man presented with unilateral right-sided conductive hearing loss (CHL) and FDTB. The Vibrant Soundbridge (VSB) MEI was implanted in the right ear. Preoperatively, the right side had a pure tone average (PTA) threshold of 67 dB, speech reception threshold (SRT) = 75 dB HL, and speech discrimination score (SDS) = 54% at 80 dB HL presentation level. Postoperative aided PTA threshold of the right ear was 28 db, aided SRT = 30 db, and SDS = 96% at 65dB HL. After excluding cholesteatoma, VSB provides an alternative hearing restoration technique for adults with FDTB and CHL due to stenosis of the external auditory canal and/or ossicular crowding.
Introduction
Fibrous dysplasia (FD) is a benign bone disorder in which the normal bone is progressively replaced by fibrous tissue. It is classified into monostotic (involving only one bone) and polystotic (involving multiple bones) FD. The polystotic form of the disease can rarely be syndromic. It manifests as Mazabraud syndrome when associated with soft tissue myxomas and McCune-Albright syndrome when accompanied by the triad: endocrinopathy, hyperpigmentation, and precocious puberty. 1 The prevalence of FD of the temporal bone (FDTB) is variable and accounts for up to 89% of craniofacial FD, 2 but only 12% of isolated FDTB. 3
Patients with FD usually present with headache, pain, sensory deficit, functional impairment, and infectious complications. 4 The most common presenting complaint of FDTB is hearing loss (58%) 5 and is usually conductive. 2 Conductive hearing loss (CHL) and sensorineural hearing loss (SNHL) can be implicated by different mechanisms. Boyce et al found ossicular crowding and internal auditory canal elongation to be associated with CHL and SNHL, respectively. Despite external auditory canal (EAC) stenosis, no significant correlation was found between the diameter of the EAC and CHL. 2 Computerized tomography (CT) can provide accurate diagnosis and exclude differential bone disorders, 6 with or without histological confirmation. 7 Three FD patterns have been described based on CT findings: mixed ground-glass appearance (pagetoid) in 55%, sclerotic in 34%, and cystic in 11% of patients with FD. 8
Vibrant Soundbridge (VSB; MedEL) middle ear implant was introduced in the late 90s. 9 It has been developed with different coupling techniques to provide strong electromagnetic amplification to the inner ear. 10 Although the device was first indicated for moderate-to-severe SNHL in adults, it has been successfully implanted for mixed and CHL. 11 Vibrant Soundbridge has showed good results in CHL even in the presence of diseased structures in the outer and middle ear including malformations (eg, aural atresia), 12,13 open cavity issues, and otosclerosis. 11 To the best of our knowledge, this is the first case of VSB implantation aimed at restoring hearing implicated by FDTB.
Case Description
A 60-year-old gentleman presented to our otology clinic at King Abdullah Ear Specialist Center in King Abdulaziz University Hospital complaining of unilateral right-sided hearing loss since childhood. He did not have a history of ear pain, discharge, tinnitus, headache, facial or other cranial nerves deficit, or any other otological complaints. Furthermore, he denied any history of previous ear surgeries or any noticeable change in condition since childhood. He was diabetic and undergoing therapy with oral hypoglycemic agents. On examination, he showed severe stenosis of the right EAC with normal overlying skin and pinna. The tympanic membrane could not be visualized due to severe stenosis. He had a normal left EAC and tympanic membrane. Rinne test was negative on the right side and positive on the left, while Weber test was lateralized to the right. ENT, head, and neck examination was otherwise normal, including all cranial nerves.
Audiological evaluation revealed moderately severe to severe CHL on the right side with 67 dB pure tone average (PTA) air conduction threshold, and normal PTA on the left side (Figure 1A). Speech audiometry of the right side showed speech reception threshold (SRT) at 75 dB HL, and speech discrimination score (SDS) of 54% at 80 dB HL and 100% at 100 dB HL presentation level (Table 1). Tympanometry could not be performed on the right side, while the left side showed normal type A curve. CT of the temporal bone showed right temporal bone generalized ground-glass appearance and expansion with intact overlying bone causing EAC stenosis and attic ossicular crowding (Figure 2).
Unaided Versus Aided Speech Audiometric Results for the Right Ear.
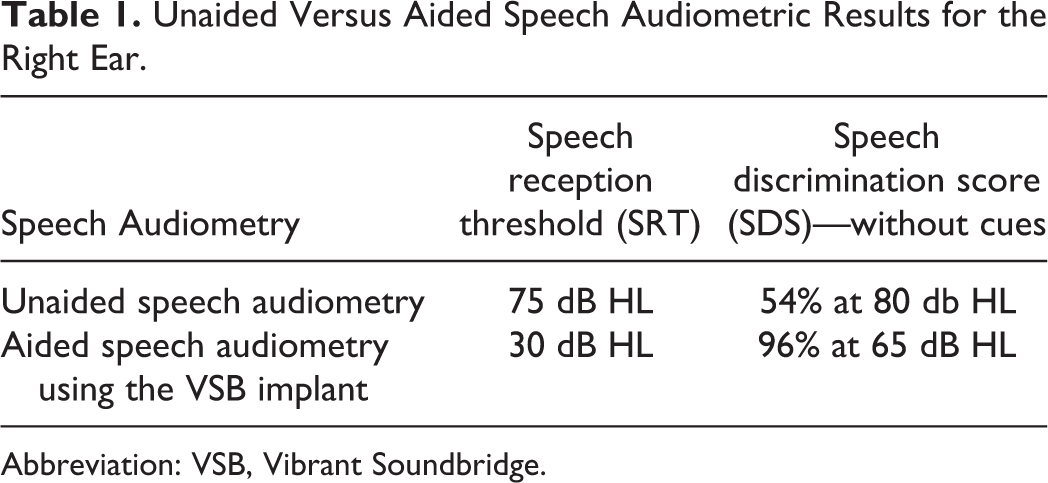
Abbreviation: VSB, Vibrant Soundbridge.
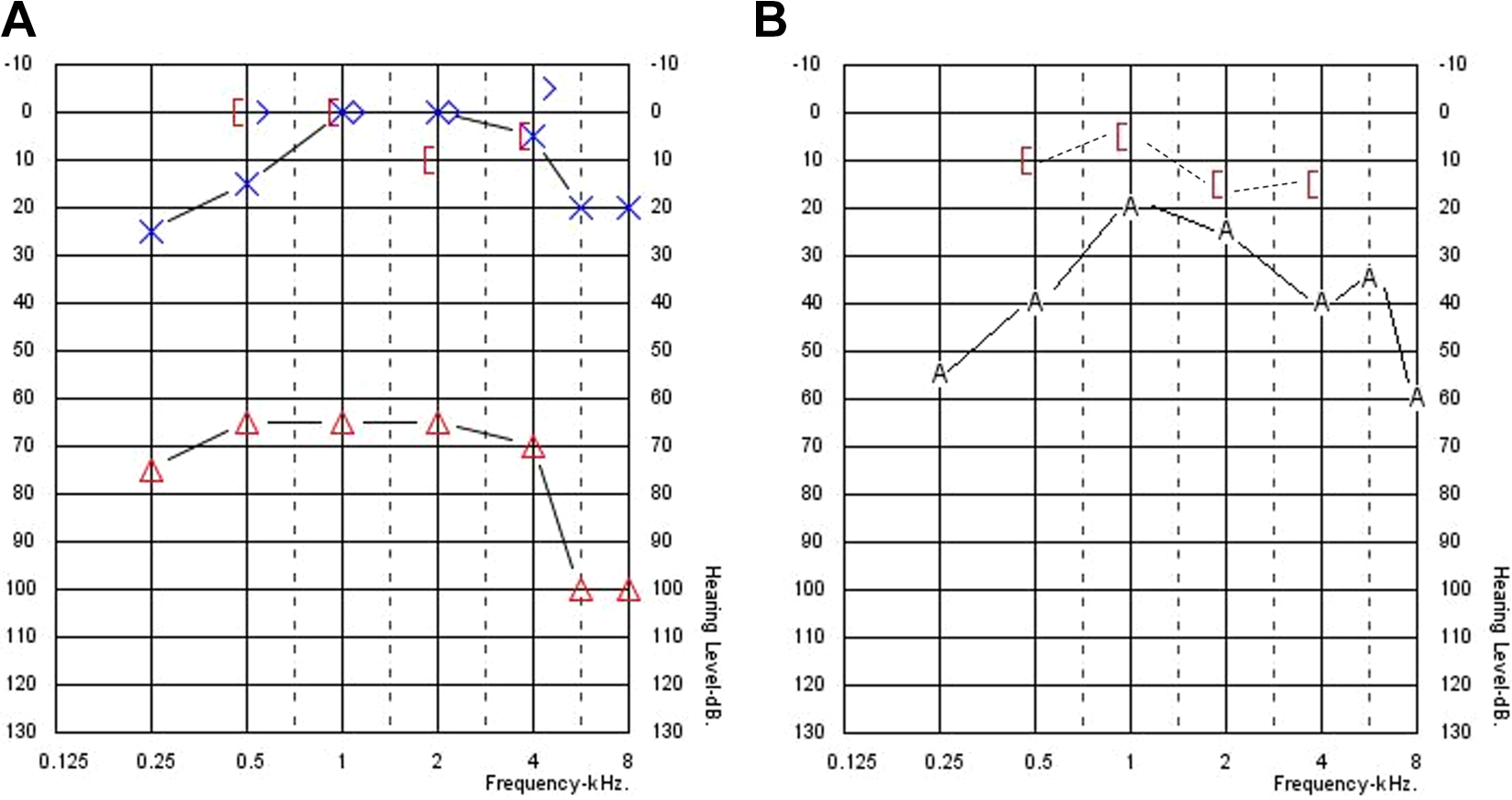
Pure tone audiometry. A, Preoperative pure tone audiometry for both right (red) and left (blue) ears. B, Postoperative aided pure tone audiometry with vibrant soundbridge in the right ear.
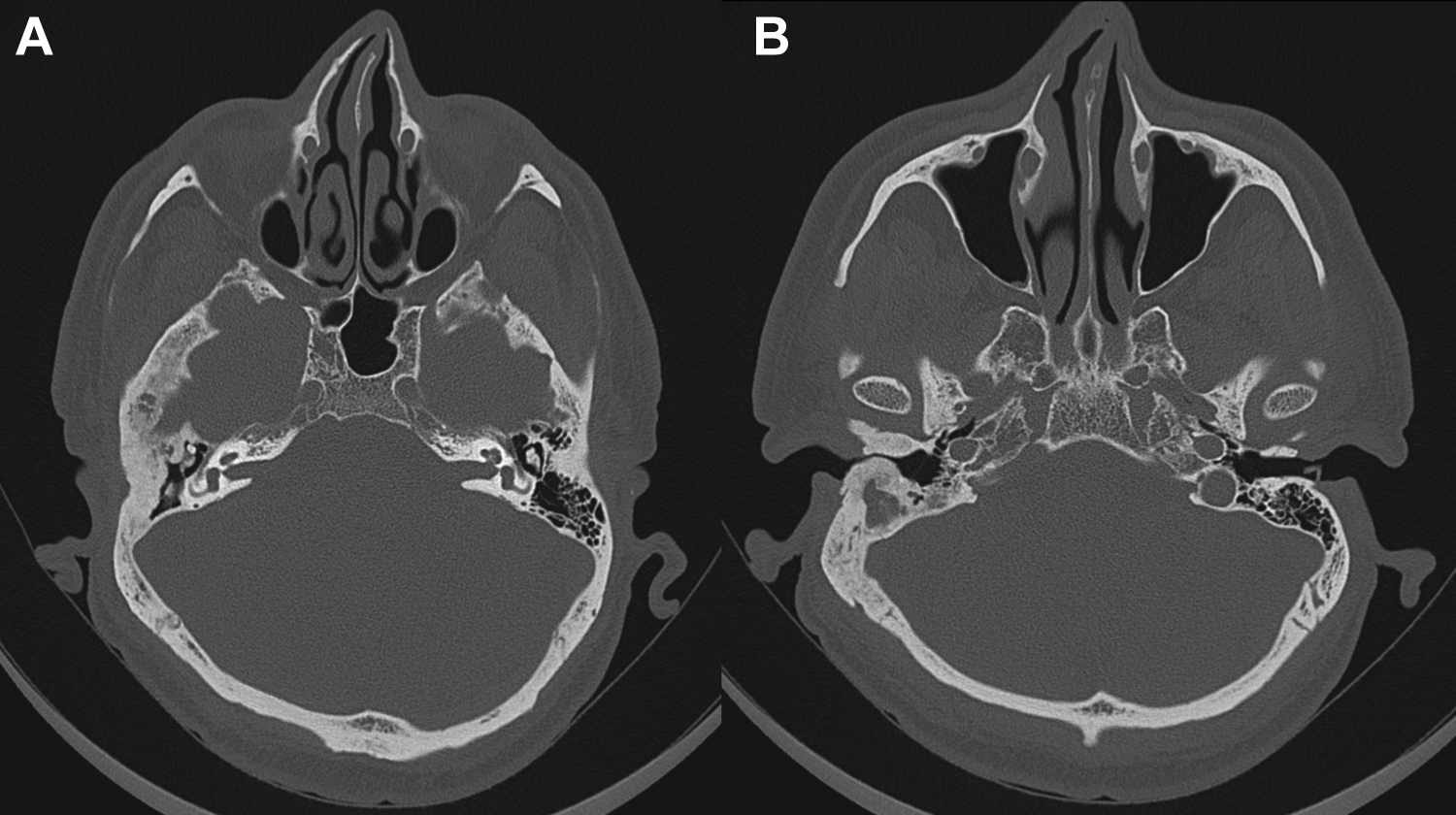
Axial cut computed tomography (CT). A, At the level of the attic; showing ground-glass appearance of the right temporal bone with ossicular crowding. Ottic capsule and internal auditory canal seem to be spared. B, At the level of the external auditory canal (EAC); showing right EAC stenosis caused by bone expansion, with no evidence of EAC cholesteatoma or bone destruction.
The patient was offered different hearing restoration options including canal reconstruction surgery; but he opted for VSB implantation and signed an informed consent. He underwent right transmastoid transposterior tympanotomy VSB implantation, which was performed while monitoring the facial nerve. Using a standard 3-cm post auricular incision, a periosteal (Palva) flap was created to expose the temporal bone. Fragments of bone were obtained for histopathological evaluation, which was negative for malignancy. The middle ear was accessed after performing cortical mastoidectomy and posterior tympanotomy. The patient was found to have lateral ossicular fixation due to attic ossicular crowding and malleus head fixation. After confirming the mobility of stapes using round window reflex, the incus was separated and removed and vibrating ossicular prosthesis (VORP) was coupled to the mobile stapes superstructure. The internal receiver portion of VORP was fixed to the calvarium at 45° from the sinodural angle using self-screwing screws. Soft tissue and skin were closed in 3 layers.
The device was switched-on 4 weeks postoperatively, and the patient received an external audio processor. Aided PTA showed 28 dB threshold PTA, while bone thresholds were within normal and comparable with preoperative PTA (Figure 1B). Aided SRT was 30 dB, and SDS at 65 dB HL presentation level was 96% (Table 1). The patient was followed up for 6 months after surgery and appeared satisfied with the device.
Discussion
Treatment of FD is challenging and continually evolving. Watchful waiting is recommended in cases of asymptomatic slowly growing lesions, especially in the polyostotic form of the disease. 14,15 Bisphosphonates have debatable efficacy in reducing pain, risk of fracture, and rate of growth. 6
Surgery is recommended for severe progressive FDTB with serious complaints, which is met in cases with EAC cholesteatoma secondary to keratin accumulation and entrapment. Surgical management of FDTB with secondary CHL includes canaloplasty, ossicular reconstruction, and mastoidectomy techniques depending on disease severity and the involved segment. 7 A systematic review by Fandiño et al showed hearing improvement in 84% of radical canaloplasty patients with full thickness skin graft. Intact wall mastoidectomy showed an improvement of hearing thresholds in 56%, worsening in 19%, and no change in 25% of patients with FD. Canal wall down mastoidectomy showed hearing improvement in all patients; however, cavity issues and postoperative precautions should be discussed thoroughly. In the same review, only one case report of isolated ossiculoplasty was performed on a patient with middle ear involvement, which showed air-bone gap (ABG) closure postoperatively. 7 Middle ear involvement in cases with EAC stenosis carries higher chances of unsatisfactory hearing restoration. Therefore, majority of these patients require hearing aids or bone conduction hearing implants (BCHI). 5 In children, however, surgery is preferably delayed until skeletal maturation to decrease the risk of recurrence, 6 as the disease tends to become inactive after puberty. 16 Recurrence was lower after total resection with reconstruction (8%) and surgeries performed after bone maturity (14%), when compared with incomplete resection or surgeries performed at a younger age (50%). 17 Overall, surgical reconstruction carries risk of restenosis, graft failure, and EAC cholesteatoma. Due to disease rarity and lack of long-term follow up, the exact incidence of such complications is not well-documented, especially in adults.
In another attempt to restore hearing, transcutaneous bone-anchored hearing aid (BAHA) was implanted in 2 patients with FD with promising results. Prior to BAHA implantation, both patients underwent revision surgery owing to EAC restenosis or resultant recurrent cholesteatoma. 4,5 However, failure of osseointegration is more likely in patients with abnormal bone transformation. 5
In this study, we propose VSB as an alternative for adults with FDTB and CHL due to EAC stenosis and/or ossicular crowding. In the absence of cholesteatoma, VSB can be particularly beneficial in patients with middle ear involvement, who tend to have unsatisfactory results with canaloplasty and/or ossiculoplasty. Moreover, VSB has multiple advantages over conventional hearing aids, BCHI, and canal-reconstruction surgery.
Hearing aids are difficult to use in stenotic EACs either due to FD or owing to a history of several revision surgeries and recurrent ear infections, which cause further occlusion of the EAC. 11
Bone conduction hearing implants that have a percutaneous pedestal require cleaning and maintenance, due to the risk of recurrent local inflammation. Failure of osseointegration is the most common complication related to BCHI 18 and is more likely to occur in FD owing to pathological bone transformation. 7 In a comparison between BAHA and VSB in patients with mixed and/or CHL, the latter was more powerful in closing the ABG with better hearing performance in both quiet and noisy environments, with added gain in SNHL. 19,20 On the other hand, Rivas et al reported a comparable hearing gain between BAHA and VSB in patients with conductive-mixed hearing loss. 21 Ultimately, the effective gain was variable depending on the implant center rather than the used device, according to a recent review by Snik et al. 22
As discussed, surgical reconstruction of the EAC plays an important role in patients with FD with progressive disease and cholesteatoma. Meanwhile, VSB provides excellent hearing outcomes in patients with stable CHL, without disruption of the EAC’s cortical bone that render them prone to restenosis or cholesteatoma.
In conclusion, FD is a rare benign bone disorder in which the normal bone is expanded by a pathological fibrous tissue. After excluding cholesteatoma, the VSB provides an alternative hearing restoration technique for adults with FDTB and CHL due to EAC stenosis and/or ossicular crowding.
Footnotes
Acknowledgments
This research was supported by King Saud University, Deanship of Science Research, and was recommended by Saudi ORL society.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Athair Alradhi is employed by MED-EL GmbH and had clinical support role only, without any marketing activities or any role in manuscript writing.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.