
Abstract
Abducens nerve schwannomas are incredibly rare, with very few cases being reported previously. Our patient is the first to have been treated through use of an endoscopic endonasal approach. A 61-year-old woman presented with diplopia over a 1-year period. Magnetic resonance imaging identified a 2.8-cm lesion expanding into her right sphenoid sinus. She underwent an endoscopic endonasal approach for histological diagnosis and clearance of the lesion. Intraoperative exploration found the lesion to be originating from Dorello canal. Histological analysis confirmed a benign schwannoma. Following a multidisciplinary case review, we have followed a conservative approach and she remains well on radiological surveillance. In patients presenting with a sixth nerve palsy/paresis and a concomitant sphenoid lesion, clinicians should consider an abducens schwannoma as a possible diagnosis.
Introduction
Schwannomas represent ∼8% of all intracranial tumors. 1 Originating from the Schwann sheath of cranial nerves, tumors occur from the overproduction of Schwann cells within the sheath. Intracranial schwannomas most commonly present in the vestibulocochlear nerve, with the trigeminal nerve being the second most frequent site. 2 Schwannomas rarely arise from a pure motor nerve, with abducens schwannomas being one of the most rare of these types. Chen first reported a schwannoma of the sixth cranial nerve in 1981. 3
Case Report
A 61-year-old woman presented with diplopia occurring over a 1-year period. She was referred to our unit after a magnetic resonance imaging (MRI) scan identified a 2.8 × 1.6 × 2.1 cm lesion expanding into her right sphenoid sinus (Figure 1). The patient underwent endoscopic exploration with the aim to get histological confirmation and to excise/debulk the lesion.
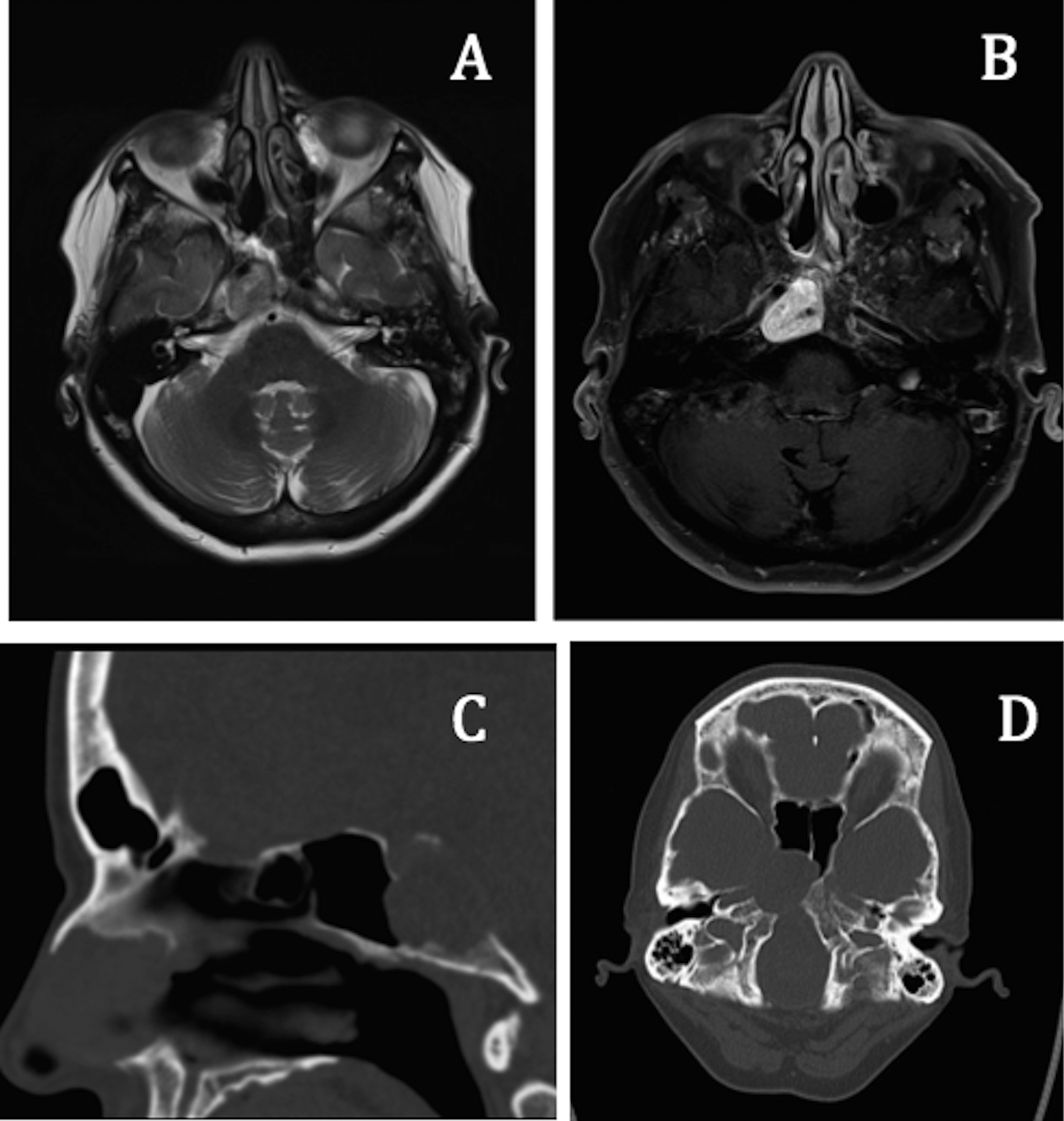
Magnetic resonance imaging (MRI; A and B) and computed tomography (CT; C and D) images showing the mass centered in Dorello canal and extending into the right sphenoid sinus.
During surgery, the intraoperative endoscopic view showed that the lesion was found to be entirely soft tissue in nature and originating from deeper structures (Figure 2). Histology confirmed a benign schwannoma displaying secondary pseudocystic degeneration with no evidence of malignancy.
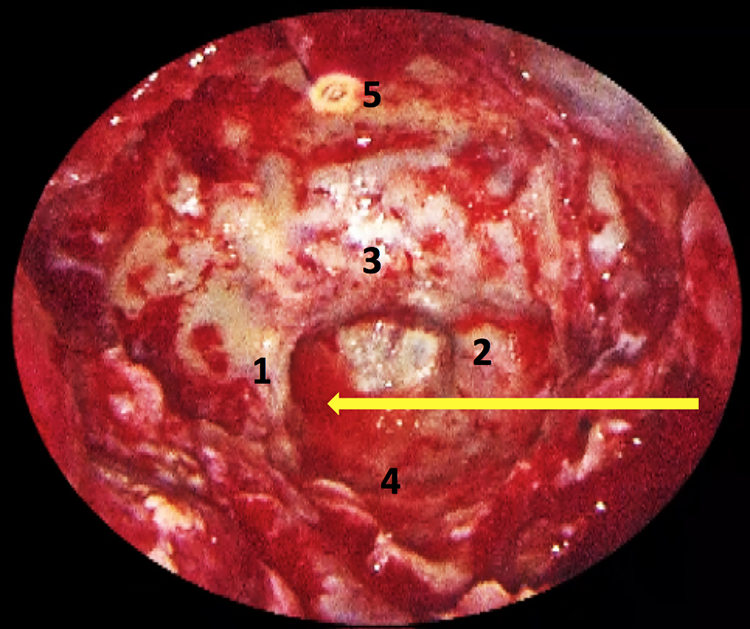
Intraoperative endoscopic view showing the approach to this region of the skull base. 1 = right internal carotid artery (ICA), 2 = left ICA, 3 = sella turcica, 4 = sphenoid floor, 5 = planum sphenoidale. Yellow arrow is pointing to the abducens nerve schwannoma.
The patient had some improvement in her sixth nerve paresis after her surgery with improvement in her diplopia. Visual acuity improved to 6/9 in the right eye and 6/5 in the left eye.
We discussed her case at our multidisciplinary team meeting where a conservative approach was recommended. Her computed tomography (CT) scan and MRI showed no increase in the size of the residual schwannoma at 2 years. She remains well and under radiological surveillance.
Discussion
Abducens schwannomas are extremely rare. The literature has shown that they may occur in the prepontine region, cavernous sinus, the orbit and overlapping areas between the 3.
Abducens schwannomas have been found at approximately the same frequency in the prepontine region as they do around the cavernous sinus. Intraorbital schwannomas are the rarest and only 4 cases have been reported.4-7
Surgery appears to be the primary method of tumor removal via a craniotomy or orbitotomy; however, radiotherapy has also been increasingly used in recent years. 8 Our patient is the first to have been treated using an expanded endonasal approach. Due to its minimally invasive nature when accessing the critical structures within the skull base, the morbidity is often much lower and we recommend this approach to be considered for all patients in whom the tumor extends into the clivus or sphenoid sinus.
The radiological features of schwannomas on CT are the same as brain and enhance after contrast medium is administered. The MRI features are of a well-defined, smoothly, expansile mass that is isointense to hypointense on T1-weighted images and hyperintense on T2-weighted images. They enhance after Gadolinium is administered. 9
In patients presenting with a sixth nerve palsy/paresis and a concomitant sphenoid lesion, clinicians should consider an abducens schwannoma as a possible diagnosis.
Management of abducens nerve schwannoma is based on symptoms and the morbidity of any potential treatment. Our patient’s abducens nerve paresis improved following surgery, and there was no evidence of growth on interval MRI imaging at 2 years. She remains under close clinical and MR surveillance.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.